Transcription
State of Connecticut2020Annual Report of Long-Term Care FacilityCost Year 2020Name of Facility (as licensed)WV-Crossings East, LLC d/b/a Harbor Village North Health & Rehabilitation CenterAddress (No. & Street, City, State, Zip Code)78 Viets Street, NewLondon, CT 06320-3354Type of Facility Rest Home with Nursing Supervision only(RHNS)Chronic and ConvalescentNursing Home only (CCNH)Report for Year Beginning10/1/2019License Numbers:Medicaid Provider Numbers:For Department Use OnlySequence NumberSigned andAssignedNotarized (Specify)Report for Year ed(Specify)RHNSSequence NumberAssignedMedicare Provider07-5146ICF-IIDSigned and NotarizedDate Received
State of ConnecticutAnnual Report of Long-Term Care FacilityCSP-1 Rev.9/2002General InformationName of Facility (as licensed)License No.WV-Crossings East, LLC d/b/a Harbor Village North H2436Report for Year Ended9/30/2020Page1of37Administrator's/Owner's CertificationMISREPRESENTATION OR FALSIFICATION OF ANY INFORMATION CONTAINED IN THISCOST REPORT MAY BE PUNISHABLE BY FINE AND/OR IMPRISIONMENT UNDER STATE ORFEDERAL LAW.I HEREBY CERTIFY that I have read the above statement and that I have examined the accompanyingCost Report and supporting schedules prepared for WV-Crossings East, LLC d/b/a Harbor Village NorthHealth & Rehabilitation Center [facility name], for the cost report period beginning October 1, 2019 andending September 30, 2020, and that to the best of my knowledge and belief, it is a true, correct, andcomplete statement prepared from the books and records of the provider(s) in accordance with applicableinstructions.I hereby certify that I have directed the preparation of the attached General Information and Questionnaires,Schedule of Resident Statistics, Statements of Reported Expenditures, Statements of Revenues and the relatedBalance Sheet of this Facility in accordance with the Reporting Requirements of the State of Connecticut for theyear ended as specified above.I have read this Report and hereby certify that the information provided is true and correct to the best ofmy knowledge under the penalty of perjury. I also certify that all salary and non-salary expensespresented in this Report as a basis for securing reimbursement for Title XIX and/or other State assistedresidents were incurred to provide resident care in this Facility. All supporting records for the expensesrecorded have been retained as required by Connecticut law and will be made available to auditors uponrequest.{a} Subject to Desk Audit ReviewSigned (Administrator)DatePrinted Name (Administrator)Troy T. GuntulisSubscribed and Swornto before me:Signed (Owner)DatePrinted Name (Owner)State ofDateSigned (Notary Public)Comm. Expires/Address of Notary Public(Notary Seal)/
Table of ContentsGeneral Information - Administrator's/Owner's CertificationGeneral Information and Questionnaire - Data Required for Real Wage AdjustmentGeneral Information and Questionnaire - Type of Facility - Organization StructureGeneral Information and Questionnaire - Partners/MembersGeneral Information and Questionnaire - Corporate OwnersGeneral Information and Questionnaire - Individual ProprietorshipGeneral Information and Questionnaire - Related PartiesGeneral Information and Questionnaire - Basis for Allocation of CostsGeneral Information and Questionnaire - LeasesGeneral Information and Questionnaire - Accounting BasisSchedule of Resident StatisticsSchedule of Resident Statistics (Cont'd)A. Report of Expenditures - Salaries & WagesSchedule A1 - Salary Information for Operators/Owners; Administrators, AssistantAdministrators and Other RelativesSchedule A1 - Salary Information for Operators/Owners; Administrators, AssistantAdministrators and Other Relatives (Cont'd)B. Report of Expenditures - Professional FeesReport of Expenditures - Schedule B-1 - Information Required for Individual(s) Paid on Feefor Service BasisC. Expenditures Other than Salaries - Administrative and GeneralC. Expenditures Other than Salaries (Cont'd) - Administrative and GeneralSchedule C-1 - Management ServicesC. Expenditures Other than Salaries (Cont'd) - DietaryC. Expenditures Other than Salaries (Cont'd) - LaundryC. Expenditures Other than Salaries (Cont'd) - Housekeeping and Resident CareReport of Expenditures - Schedule C-2 - Individuals or Firms Providing Services by ContractC. Expenditures Other than Salaries (Cont'd) - Maintenance and PropertyDepreciation ScheduleAmortization ScheduleC. Expenditures Other than Salaries (Cont'd) - Property QuestionnaireC. Expenditures Other than Salaries (Cont'd) - InterestC. Expenditures Other than Salaries (Cont'd) - Interest and InsuranceD. Adjustments to Statement of ExpendituresD. Adjustments to Statement of Expenditures (Cont'd)F.Statement of RevenueG. Balance SheetG. Balance Sheet (Cont'd)G. Balance Sheet (Cont'd)G. Balance Sheet (Cont'd)G. Balance Sheet (Cont'd) - Reserves and Net WorthH. Changes in Total Net WorthI.Preparer's/Reviewer's 2122232425262728293031323334353637
State of ConnecticutAnnual Report of Long-Term Care FacilityCSP-1A Rev. 6/95State of ConnecticutDepartment of Social Services55 Farmington Avenue, Hartford, Connecticut 06105Data Required for Real Wage AdjustmentName of FacilityPeriod Covered:WV-Crossings East, LLC d/b/a Harbor Village North Health & Rehabilitation CenterAddress of Facility78 Viets Street, NewLondon, CT 06320-3354Report Prepared ByPhone NumberMarcum LLP203-781-9600ItemTotal1.Dietary wages paid 2.Laundry wages paid 3.Housekeeping wages paid 4.Nursing wages paid 5.All other wages paid 6.Total Wages Paid 7.Total salaries paid 8.Total Wages and Salaries Paid (As per page 10 of Report) CCNHPageof1A37FromTo10/1/2019 9/30/2020Date1/10/2021RHNSWages - Compensation computed on an hourly wage rate.Salaries - Compensation computed on a weekly or other basis which does not generally vary, based on thenumber of hours worked.DO NOT include Fringe Benefit Costs.(Specify)
State of ConnecticutAnnual Report of Long-Term Care FacilityCSP-2 Rev. 10/2005General Information and QuestionnaireType of Facility - Organization StructurePhone No. of Facility Report for Year EndedPageof9/30/2020860-447-1416237Name of Facility (as shown on license)Address (No. & Street, City, State, Zip )WV-Crossings East, LLC d/b/a Harbor Village North Health &78 Viets Street, NewLondon, CT 06320-3354CCNHMedicare Provider No.RHNS(Specify)License Numbers:243607-5146Type of Facility (Check appropriate box(es)) Chronic and ConvalescentNursing Home only (CCNH) Rest Home with NursingSupervision only (RHNS) (Specify)Type of Ownership (Check appropriate box) Proprietorship LLC Partnership Profit Corp. Non-Profit Corp.Date Opened Government TrustDate ClosedIf this facility opened or closed during report year provide:Has there been any change in ownershipor operation during this report year?N/AAdministratorName of AdministratorTroy T. Guntulis Yes NoIf "Yes," explain fully.Nursing HomeAdministrator'sLicense No.:Other Operators/Owners who are assistant administrators (full or part time) of this facility.NameLicense No.:N/A001810
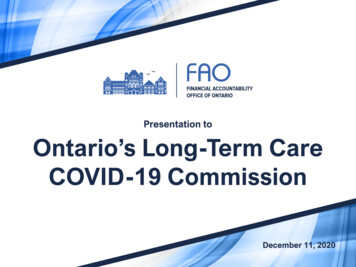
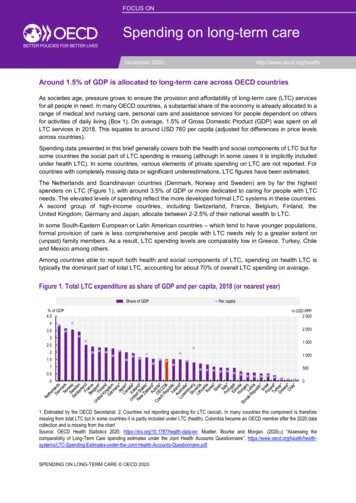
State of ConnecticutAnnual Report of Long-Term Care FacilityCSP-3 Rev. 10/2005General Information and QuestionnairePartners/MembersName of FacilityLicense No.Report for Year EndedPageofWV-Crossings East, LLC d/b/a Harbor Village North H2436 9/30/2020337State(s) and/or Town(s) inLegal Name of Partnership/LLCBusiness AddressWhich RegisteredWachusett Ventures, LLC11 Mayor Thomas J.MA, CTMcGrath Hwy, MA 02169Name of Partners/MembersSee attachedBusiness AddressTitle% Owned
SPE’s for all OPCOs and PROPCOsWachusett Ventures LLC (100%)4849-4821-1757.1Raymond A.Dennehy, IIISteven VeraWakefield CapitalLLC(20%)(20%)(60%)Joel E. KirchickPatrick FrioliWilliam Coccola(90%)(5%)(5%)
State of ConnecticutAnnual Report of Long-Term Care FacilityCSP-3A Rev. 10/2005General Information and QuestionnaireCorporate OwnersName of FacilityLicense No.Report for Year EndedPageofWV-Crossings East, LLC d/b/a Harbor Villag24369/30/20203A37If this facility is owned or operated as a corporation, provide the following information:Legal Name of CorporationBusiness AddressState(s) in Which IncorporatedN/AName of Directors, OfficersN/ANames of Stockholders Owning at Least 10%of SharesN/ABusiness AddressTitleNo. SharesHeld by Each
State of ConnecticutAnnual Report of Long-Term Care FacilityCSP-3B Rev. 10/2005General Information and QuestionnaireIndividual ProprietorshipName of FacilityLicense No.Report for Year EndedPage24369/30/20203BWV-Crossings East, LLC d/b/a Harbor Village NorIf this facility is owned or operated as an individual proprietorship, provide the following information:Owner(s) of FacilityN/Aof37
State of ConnecticutAnnual Report of Long-Term Care FacilityCSP-4 Rev. 10/2005General Information and QuestionnaireRelated Parties*Name of FacilityLicense No.WV-Crossings East, LLC d/b/a Harbor Village North H2436Report for Year Ended9/30/2020Are any individuals receiving compensation from the facility related throughmarriage, ability to control, ownership, family or business association? YesAre any individuals or companies which provide goods or services,including the rental of property or the loaning of funds to this facility,related through family association, common ownership, control, or businessassociation to any of the owners, operators, or officials of this facility?Name of RelatedIndividual or CompanyWachusett Ventures, LLCBusinessAddress36 Washington St. Suite 395,Wellesley Hills, MA 02481 of37If "Yes," provide the Name/Address andcomplete the information on Page 11 of the report. Yes NoIf "Yes," provide the following information:Also ProvidesGoods/Services toNon-Related PartiesYesNo%** NoPage4Description of Goods/ServicesProvidedManagement Fee* Use additional sheets if necessary.** Provide the percentage amount of revenue received from non-related parties.Indicate WhereCosts are Includedin Annual ReportCostPage # / Line # ReportedPg. 16/ Line m12550,572Actual Cost to theRelated Party342,871*Note: Facility self-disallowed more than the difference between thecost reported and actual cost to RP. Therefore, no additionaladjustment necessary.*
State of ConnecticutAnnual Report of Long-Term Care FacilityCSP-5 Rev. 9/2002General Information and QuestionnaireBasis for Allocation of CostsName of FacilityLicense No.Report for Year EndedPageofWV-Crossings East, LLC d/b/a Harbor Village N9/30/20205372436If the facility is licensed as CDH and/or RCH or provides AIDS or TBI services with special Medicaid rates, costsmust be allocated to CCNH and RHNS as follows:ItemMethod of AllocationDietaryNumber of meals served to residentsLaundryNumber of pounds processedHousekeepingNumber of square feet servicedNumber of hours of routine care provided by EACHNursingemployee classification, i.e., Director (or Charge Nurse),Registered Nurses, Licensed Practical Nurses, Aides andAttendantsDirect Resident Care ConsultantsNumber of hours of resident care provided by EACHspecialist (See listing page 13 )Maintenance and operation of plantSquare feetProperty costs (depreciation)Square feetEmployee health and welfareGross salariesManagement servicesAppropriate cost center involvedAll other General Administrative expensesTotal of Direct and Allocated CostsThe preparer of this report must answer the following questions applicable to the cost information provided.1. In the preparation of this Report, were allIf "No," explain fully why such allocation was not Yes Nocosts allocated as required?made.N/A2. Explain the allocation of related company expenses and attach copy of appropriate supporting data.N/A3. Did the Facility appropriately allocate and self-disallow direct and indirect costs to non-nursing home cost centers?(e.g., Assisted Living, Home Health, Outpatient Services, Adult Day Care Services, etc.) YesN/A NoIf "No," explain fully why such allocation was notmade.
State of ConnecticutAnnual Report of Long-Term Care FacilityCSP-6 Rev. 9/2002General Information and QuestionnaireLeases (Excluding Real Property)Operating Leases - Include all long-term leases for motor vehicles and equipment that have not been capitalized. Short-term leases or as needed rentalsshould not be included in these amounts.Name of FacilityLicense No.Report for Year EndedPageof24369/30/2020637WV-Crossings East, LLC d/b/a Harbor Village North HealthRelated * toOwners,Operators,AnnualOfficersDate ofTerm ofAmountAmountDescription of Items LeasedName and Address of LessorYesNoLease**Leaseof LeaseClaimedACPL A Hanger Company, 4850 Joule Street, Suite A1,Reno NV 89502Quadient Leasing, USA, 478 Wheelers Farms rd, Milford,CT 06461First DataEcolab, Inc.Xerox Financial Services Lease contract service fee, Omnisound 300 E,Omnicsound 500 Pro OmniStim FX2 Pro etc.Postage Machine Dish Machine Copy Machines 11/01/1403/26/1939 Months02/05/15Credit Card Machine Monthly asneededMonthly 05/01/16Is a Mileage Log Book Maintained for All Leased Vehicles ? Yes* Refer to Page 4 for definition of related. If "Yes," transaction should be reported on Page 4 also.** Attach copies of newly acquired leases.*** Amount should agree to Page 22, Line 6e. l ***25,068
State of ConnecticutAnnual Report of Long-Term Care FacilityCSP-7 Rev. 6/95General Information and QuestionnaireAccounting BasisName of FacilityLicense No.Report for Year Ended24369/30/2020WV-Crossings East, LLC d/b/a HarThe records of this facility for the period covered by this report were maintained on the following basis: Accrual CashPage7of37 Modified CashIs the accounting basis for thisperiod the same as for the Yesprevious period? NoIndependent Accounting FirmName of Accounting Firm1 Marcum2 CliftonLarsonAllen34Services Provided by This Firm (describe fully )If "No," explain.Address (No. & Street, City, State, Zip Code)555 Long Wharf Drive, New Haven, CT 06511300 Crown Colony Plaza, Ste 310, Quincy, MA 021691Cost Report Preparation, Advisory Reimbursement Services, Tax 7,6582Assurance Services 7,9683 4 Charge for Services Provided 15,626Are These Charges Reflected in the Expenditure Portion of This Report? If Yes, Specify Expense Classification and Line No.Page 15, Line 1d Yes NoLegal Services InformationName of Legal Firm or Independent Attorney1 See Attached2345Address (No. & Street, City, State, Zip Code )1 See Attached2345Services Provided by This Firm (describe fully )1See AttachedTelephone NumberSee Attached See Attached2 3 4 5 Charge for Services Provided Are These Charges Reflected in the Expenditure Portion of This Report? If Yes, Specify Expense Classification and Line No. Yes NoPage 15, Line 1e
State of ConnecticutAnnual Report of Long-Term Care FacilityCSP‐7 Rev. 6/95General Information and QuestionnaireAccounting BasisName of FacilityLicense No.Report for Year EndedWV‐Crossings East, LLC d/b/a Harbor24369/30/2020The records of this facility for the period covered by this report were maintained on the following basis: Accrual CashIs the accounting basis for thisperiod the same as for theprevious period?Page7aof37 Modified Cash Yes NoIf "No," explain.0Independent Accounting FirmName of Accounting Firm1234Services Provided by This Firm ( describe fully )Address (No. & Street, City, State, Zip Code)1 2 3 4 Charge for Services Provided 0Are These Charges Reflected in the Expenditure Portion of This Report? If Yes, Specify Expense Classification and Line No. Yes NoLegal Services InformationPage 15, Line 1dName of Legal Firm or Independent Attorney1New London Probate Court2SIEGEL, O'CONNOR, O'DONNELL & BECK, P.C.3LAW OFFICE OF JASON G. DEGENARO, LLC4CT Corporation5Dorsi & Dorsi6NixonPeabody7Healthcare Services Group8CourtCallAddress (No. & Street, City, State, Zip Code )1181 State St, Room 2, PO Box 148, New London, CT 063202150 Trumbull St. Hartford, CT 06103329 Water St., Guilford, CT 064374PO Box 4349, Carol Stream, IL 601975537 Washington Ave, West Haven, CT 065166100 Summer St, Boston, MA 0211073220 Tillman Dr, Ste 300, Bensalem, PA 1902086383 Arizona Circle, Los Angeles, CA 90045Services Provided by This Firm ( describe fully )Telephone ip 2,9892General Matters Relating to Employees; Union Decertification 55,6903Collections 1,0004Domestic Representation 1505Real Estate Tax Abatement 29,048(4,500)6NixonPeabody Prior Year Adjustment 7NLRB Settlement 9378CourtCall appearance for probate 113Charge for Services Provided Are These Charges Reflected in the Expenditure Portion of This Report? If Yes, Specify Expense Classification and Line No. Yes NoPage 15, Line 1e85,427
State of ConnecticutAnnual Report of Long-Term Care FacilityCSP-8 Rev. 9/2002Schedule of Resident StatisticsName of FacilityLicense No.WV-Crossings East, LLC d/b/a Harbor Village North Health & Rehabilit2436Report for Year Ended9/30/2020Page8Period 10/1 Thru 6/30Total AllLevels1. Certified Bed CapacityA. On last day of PREVIOUS report talCCNH128128128B. On last day of THIS report period2. Number of ResidentsA. As of midnight of PREVIOUS report period128128122122B. As of midnight of THIS report period3. Total Number of Days Care Provided During pecify)Period 7/1 Thru 10891891G. Total Care Days During Period (3A thru F)Total Number of Days Not Included in Figures in4. 3G for Which Revenue Was Received for ReservedBedsA. Medicaid Bed Reserve DaysB. Other Bed Reserve 661671676655115. Total Resident Days (3G 4A 4B)43,68343,68332,74632,74610,93710,937A. MedicareB.Medicaid (Conn.)C.Medicaid (other states)D. Private PayE.State SSI for RCHF.Other (Specify)122of37122RHNS(Specify)
State of ConnecticutAnnual Report of Long-Term Care FacilityCSP-9 Rev. 9/2002Schedule of Resident Statistics (Cont'd)Name of FacilityLicense No.2436WV-Crossings East, LLC d/b/a Harbor VillageReport for Year Ended9/30/2020 Yes4. Were there any changes in the certified bed capacity during the report year?If "YES", provide the following information:Date ofChangePlace of Change(Specify)CCNH RHNS(1)(2)Change in BedsLost(3)(1)Page9of37 NoCapacity After ChangeGained(2)(3)(1)(2)(3)CCNHRHNS(Specify)Reason for Change5. If there was any change in certified bed capacity during the report year (as reported in item 4 above) provide the number ofRESIDENT DAYS for 90 days following the change.CCNHChange in Resident Days1st change2nd change3rd change4th change6. Number of Residents and Rates on September 30 of Cost YearMedicareMedicaidItemNo. of ResidentsPer Diem Ratea. One bed rm.b. Two bed rms.c. Three or morebed ious201.31415.007. Total Number of Physical Therapy TreatmentsA. Medicare - Part BB. Medicaid (Exclusive of Part B)1. Maintenance Treatments2. Restorative TreatmentsC. OtherD. Total Physical Therapy Treatments8. Total Number of Speech Therapy TreatmentsA. Medicare - Part BB. Medicaid (Exclusive of Part B)1. Maintenance Treatments2. Restorative TreatmentsC. OtherD. Total Speech Therapy Treatments9. Total Number of Occupational Therapy TreatmentsA. Medicare - Part BB. Medicaid (Exclusive of Part B)1. Maintenance Treatments2. Restorative TreatmentsC. OtherD. Total Occupational Therapy TreatmentsOther State 11,4027,9777,9771,5591,5596,55716,0936,55716,093
State of ConnecticutAnnual Report of Long-Term Care FacilityCSP-10 Rev. 9/2002Report of Expenditures - Salaries & WagesName of FacilityWV-Crossings East, LLC d/b/a Harbor Village North HealthLicense No.Report for Year Ended2436Pageof1037(Specify)Hours9/30/2020 YesAre time records maintained by all individuals receiving compensation? NoTotal Cost and HoursItemA. Salaries and Wages*1. Operators/Owners (Complete also Sec. Iof Schedule A1)2. Administrator(s) (Complete also Sec. IIIof Schedule A1)3. Assistant Administrator (Complete also Sec. IVof Schedule A1)4. Other Administrative Salaries (telephoneoperator, clerks, receptionists, etc.)5. Dietary Servicea. Head Dietitianb. Food Service Supervisorc. Dietary Workers6. Housekeeping Servicea. Head Housekeeperb. Other Housekeeping Workers7. Repairs & Maintenance Servicesa. Engineer or Chief of Maintenanceb. Other Maintenance Workers8. Laundry Servicea. Supervisorb. Other Laundry Workers9. Barber and Beautician Services10. Protective Services11. Accounting Servicesa. Head Accountantb. Other Accountants12. Professional Care of Residentsa. Directors and Assistant Director of Nursesb. RN1. Direct Care2. Administrative**c. LPN1. Direct Care2. Administrative**d. Aides and Attendantse. Physical Therapistsf. Speech Therapistsg. Occupational Therapistsh. Recreation Workersi. Physicians1. Medical Director2. Utilization Review3. Resident Care***4. Other sSocial Workers/Case ManagementMarketingOther (Specify)See Attached ScheduleA-13. Total Salary * Do not include in this section any expenditures paid to persons who receive a fee for services rendered or who are paid on a contract basis.** Administrative - costs and hours associated with the following positions: MDS Coordinator, Inservice Training Coordinator andInfection Control Nurse. Such costs shall be included in the direct care category for the purposes of rate setting.*** This item is not reimbursable to facility. For Title 19 residents, doctors should bill DSS directly. Also, any costs for Title 18 and/or otherprivate pay residents must be removed on Page 28.
WV-Crossings East, LLC d/b/a Harbor Village North Health & Rehabilitation Center9/30/2020Attachment Page 10/13Schedule of Other Salaries and Wages (Page 10)CCNHRHNSPosition Hours Medical Records 33,6621,512Total 33,6621,512 (Specify)Hours- - Hours--Schedule of Other Fees (Page 13)CCNHRHNSService Hours Pro Fees - Nurse ConsultantPro Fees - Medical ServicePhysician Services - OtherPro Fees - Consulting - IVPro Fees - Other - Ancillary tal 24,933- (Specify)Hours- - Hours--
State of ConnecticutAnnual Report of Long-Term Care FacilityCSP-11 Rev. 10/2005Schedule A1 - Salary Information for Operators/Owners; Administrators,Assistant Administrators and Other Related Parties*Name of FacilityLicense No.WV-Crossings East, LLC d/b/a Harbor Village North Health & RehabiliReport for Year sationReceivedSalary PaidNameCCNHRHNS(Specify)Fringe Benefitsand/or OtherPayments(describe fully)Full Description ofServices RenderedSection I - Operators/OwnersSection II - Other related partiesof Operators/Owners employedin and paid by facility (EXCEPTthose who may be theAdministrator or AssistantAdministrators who areidentified on Page 12).* No allowance for salaries will be considered unless full information is provided. Use additional sheets if required.** Include all employment worked during the cost year.TotalHoursWorkedLine WhereClaimed onPage 10Name and Address of AllOther Employment**
State of ConnecticutAnnual Report of Long-Term Care FacilityCSP-12 Rev. 10/2005Schedule A1 - Salary Information for Operators/Owners; Administrators,Assistant Administrators and Other Related Parties*Name of Facility (as licensed)License No.WV-Crossings East, LLC d/b/a Harbor Village North Health & Rehabi2436Report for Year onReceivedSalary PaidNameCCNHRHNS(Specify)Fringe Benefitsand/or OtherPayments(describe fully)Full Description ofServices RenderedLine WhereTotal Hours Claimed on Name and Address of AllWorkedPage 10Other Employment**Section III - Administrators***Troy T. on IV - AssistantAdministrators*No allowance for salaries will be considered unless full information is provided. Use additional sheets if required.** Include all other employment worked during the cost year.*** If more than one Administrator is reported, include dates of employment for each.2,080
State of ConnecticutAnnual Report of Long-Term Care FacilityCSP-13 Rev. 9/2002B. Report of Expenditures - Professional FeesName of FacilityLicense No.2436WV-Crossings East, LLC d/b/a Harbor Village NorthItem*B. Direct care consultants paid on a feefor service basis in lieu of salary(For all such services complete Schedule B1)1. Dietitian2. Dentist3. Pharmacist4. Podiatrist5. Physical Therapya. Resident Careb. Other6. Social Worker7. Recreation Worker8. Physiciansa. Medical Director (entire facility)b. Utilization Review(Title 18 and 19 only) monthly meetingc. Resident Care**d. Administrative Services facilityCCNHReport for Year Ended9/30/2020Total Cost and HoursHoursRHNSHoursPage13of37(Specify)Hours8,320 Monthly11,286 Monthly307,3693,76933,600 Monthly1. Infection Control Committee(Quarterly meetings)2. Pharmaceutical Committee(Quarterly meetings)3. Staff Development Committee(Once annually)e. Other (Specify)9. Speech Therapista. Resident Careb. Other10. Occupational Therapista. Resident Careb. Other11. Nurses and aides and attendantsa. RN1. Direct Care2. Administrative***b. LPN1. Direct Care2. Administrative***c. Aidesd. Other12. Other (Specify)See Attached ScheduleB-13 Total Fees Paid in Lieu of 3826,0009,175* Do not include in this section management consultants or services which must be reported on Page 16 item M-12 and supported by required information, Page 17.** This item is not reimbursable to facility. For Title 19 residents, doctors should bill DSS directly. Also, any costs for Title 18 and/or other private pay residents mustbe removed on Page 28.*** Administrative - costs and hours associated with the following positions: MDS Coordinator, Inservice Training Coordinator and Infection Control Nurse. Suchcosts shall be included in the direct care category for the purposes of rate setting.
State of ConnecticutAnnual Report of Long-Term Care FacilityCSP-14 Rev. 6/95Report of ExpendituresSchedule B1 - Information Required for Individual(s) Paid on Fee for Service Basis*Name of FacilityLicense No.WV-Crossings East, LLC d/b/a Harbor Village North He2436Report for Year EndedPageof9/30/20201437Related** to Owners,Operators, OfficersExplanation of RelationshipYesNoName & Address of IndividualFull Explanation of ServiceParagon Rehabilitiation, 303 N Hurstbourne Pkwy,Louisville, KY 40222PT/OT/ST N/APharmerica, PO Box 409251, Atlanta, GA 30384Pharmacist / IV Consultant N/AIPC Healthcare, 3 Barker Ave. White Plains, NY10601Medical Director N/ADentist N/ARN's, DON N/AWorldwide Staffing, 2222 Sedwick Rd, Durham,NC 27713LPN N/ACeltic Consulting, 507 East Main Street, Ste 308,Torrington, CT 06790Nurse Consultant N/A LTC Management LLCMed Solutions, 1010 N 102nd St, Ste 300, Omaha,NE 68114* Use additional sheets if necessary.** Refer to Page 4 for definition of related.
State of ConnecticutAnnual Report of Long-Term Care FacilityCSP-15 Rev. 9/2018C. Expenditures Other Than Salaries - Administrative and GeneralName of FacilityLicense No.2436WV-Crossings East, LLC d/b/a Harbor Village NItem1. Administrative and Generala. Employee Health & Welfare Benefits1. Workmen's Compensation2. Disability Insurance3. Unemployment Insurance4. Social Security (F.I.C.A.)5. Health Insurance6. Life Insurance (employees only)(not-owners and not-operators)7. Pensions (Non-Discriminatory)(not-owners and not-operators)8. Uniform Allowance9. Other (Specify )See Attached Scheduleb. Personal Retirement Plans, Pensions, andProfit Sharing Plans for Owners andOperators (Discriminatory)*c.d.e.f.Report for Year Ended9/30/2020TotalCCNH 116,748116,748419,893275,244419,893275,244 1,5281,52814,88114,881 of37RHNS(Specify) Bad Debts*Accounting and AuditingLegal (Services should be fully described on Page 7)Insurance on Lives of Owners andOperators (Specify )*g. Office Suppliesh. Telephone and Cellular Phones1. Telephone & Pagers2. Cellular Phonesi. Appraisal (Specify purpose andattach copy )* 181,41315,62685,427181,41315,62685,427 47,45347,453 14,3664,96614,3664,966j. Corporation Business Taxes (franchise tax )k. Other Taxes (Not related to property - See Page 22)1. Income*2. Other (Specify )See Attached Schedule3. Resident Day User FeeSubtotal 7,9607,960 833,6962,019,201833,6962,019,201* Facility should self-disallow the expense on Page 28 of the Cost Report.Page15(Carry Subtotals forward to next page)
*** DO NOT Include Holiday Parties / Awards / Gifts to StaffWV-Crossings East, LLC d/b/a Harbor Village North Health & Rehabilitation CenteAttachment Page 159/30/2020Schedule of Other Employee BenefitsDescriptionCCNH(Specify)RHNSEmployee Background CheckNursing Home week expensesEmp Ben - Employee Drug ScreenEmployee recognitionMeals & Ent. - Nursing AdminMeals & Ent. - A&GMeals & Ent. - MarketingMeals & Ent. - Dietary 8,8552,6132,04850921629626777Total 14,881 - -Schedule of Other TaxesDescriptionCCNH(Specify)RHNS-Total - - -
State of ConnecticutAnnual Report of Long-Term Care FacilityCSP-16 Rev. 9/2002C. Expenditures Other Than Salaries (cont'd) - Administrative and GeneralName of FacilityLicense No.2436WV-Crossings East, LLC d/b/a H
WV-Crossings East, LLC d/b/a Harbor Village North Health & Rehabilitation Center 10/1/2019 9/30/2020 Address of Facility 78 Viets Street, NewLondon, CT 06320-3354 Report Prepared By Phone Number Date Marcum LLP 203-781-9600 Item Total CCNH RHNS 1. Dietary wages paid 2. Laundry wages paid 3. Housekeeping wages paid 4. Nursing wages paid 5.