Transcription
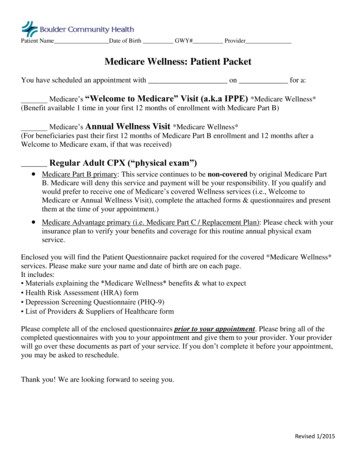
U':JI:!Medicare Annual Wellness VisitQuestionnaireDate:Name:FIRSTLASTHome Address:---s m E ETDate of Birth: --:-:-:-:- MIDDLEMM!DD! CCYYCITYAPT/UNITSTATEZIPGender: 0 Female 0 MaleHome Phone: Day Phone:Cell Phone:ss # : - - - - - - - - - - -NextofKiniforemergency):Name of spouse : - - - - - - - - - - - - - - - - - -Day Phone:Referred by: - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - Insurance: Name - - - - - - - - - - - - - - - - - Phone#Policy# - - - - - - - - - - - - -Group#-------------List any current medical problems or conditions.1)7)2)8)3)9)4)10)5)11)6)12)Childhood Illnesses1}3}5}2}4}6}1}3)5)2)4)6)Chronic IllnessesLast Eye/Glaucoma Exam:Past surgeriesSurgeryDateSurgery1}4)2}5)Date.L
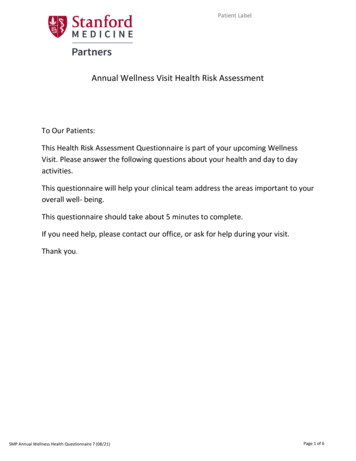
ruyt:LDate of Birth:Patient Name: - - - - - - - - - - - - - - - - - - - List any other hospital actitioners you currently seeName I SpecialtyName I Specialty1)4)2)5)List any allergies to medication. x-ray dyes. or food.AllergyReactionList any medication that you currently take. including over-the-counter.NameStrengthDirectionPrescribed byDo you drink alcohol? . D No D YesIf yes how m u c h ? - - - - - - - - - - - - - - Are others concerned about your drinking?D No D YesDiet: DBalanced DVegetarian DDiabetic Dlow salt Dlow fat Dlow carb D Other:Education: D High school D College D Some College D Trade school D Other:Do you do some form of regular exercise every day? D No DYesIf yes, how much?Marital Status: D MarriedD Single D Divorced D Widowed D OtherOccupation:--------------List everyone in your household including pets:Do you wear seatbelts? . D No D YesHave you ever smoked or chewed tobacco? . DNa D YesIf yes, how much?
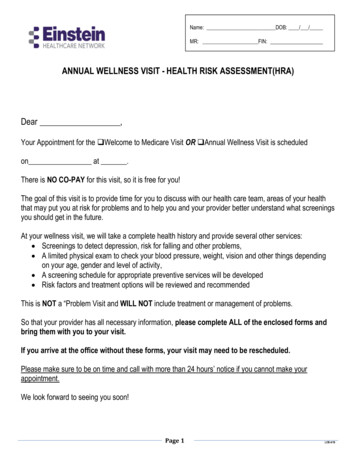
ruyr:: .: Patient Name: - - - - - - - - - - - - - - - - - - -Date of Birth:ROUTINE TASKS: Please indicate ii'l.ou do or do not need hele e erforming these routine tasks1) Feeding yourselfD No D YesIf yes, who helps?2) Getting from bed to chairD No D YesIf yes, who helps?3) Getting to t he toiletD No D YesIf yes, who helps?4) Getting dressedD No D YesIf yes, who helps?5) Bathing or showeringD No D YesIf yes, who helps?6) Walking across the room(includes using cane or wa lker)D No D YesIf yes, who helps?7) Using the telep honeD No D YesIf yes, who helps?8) Taking your medicinesD No D YesIf yes, who helps?9) Preparing mealsD No D YesIf yes, who helps?10) Managing money(like keeping track of expenses or paying bills)D No D YesIf yes, who helps?11) Moderately strenuous housework suchas doing t he laundryD No D YesIf yes, who helps?12) Shopping fo r persona l items like toiletriesor medicinesD No D YesIf yes, who helps?13) Shopping for groceriesD No D YesIf yes, who helps?14) DrivingD No D YesIf yes, who helps?15) Climbing a flight of stairsD No D YesIf yes, who helps?Please list any health problems and causes of death if applicable.Living I DeceasedFatherMotherBrother(s)Sister(s)Mother's fat herMother's motherFather's fatherFather's motherAgeMedical Problems
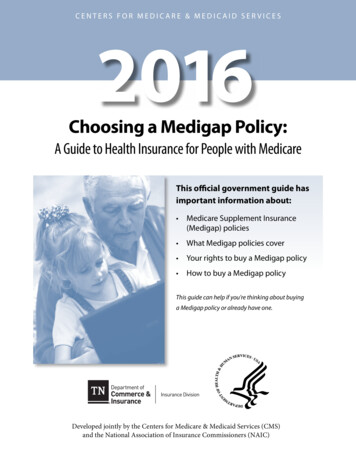
ruyr: .Patient Name: - - - - - - - - - - - - - - - - - - - -Date of Birth:Please record the last year you had the following. If you do not know, leave blank.HepB (shot) .Hearing Exam .Flu vaccine (shot).Hemocult .Pneumonia vaccine (shot) .Lipid Panel .Tetanus Diphtheria vacdne(shot).Mammogram .Zostavax (shot) .Nutritional Therapy .Abdom . Aortic Aneurysm Screening .Pap Smear .Bone Density Scan .Pelvic Exam .Colonoscopy .Prostate Exam .Diabetes Self Management Training .PSA Test .Echocardiogram .Rectal Exam .Eye Glaucoma Exam .Smoking Cessation .Glucose .HEARING: Check NO, YES, or SOME TIMES for each question.1) Do you find it difficult to follow a conversation in anoisy restaurant or crowded room? . D No DYes D Sometimes2) Do you sometimes feel that people are mumbling or notspeaking clearly? . D No D Yes D Sometimes3) Do you experience difficulty following dialogue in the theater? . D No DYes D Sometimes4) Do you sometimes find it difficult to understand a speaker ata public meeting or religious service? . D No D Yes D Sometimes5) Do you find yourself asking people to speak up or repeat themselves? . D No DYes D Sometimes6) Do you find men 's voices easier to understand than women's? . D No D Yes D Sometimes7) Do you experience difficulty understanding soft or whispered speech? . D No DYes D Sometimes8) Do you sometimes have difficulty understanding speechon the telephone? . 0 No D Yes D Sometimes9) Does a hearing problem cause you to feel embarrassed whenmeeting new people? . D No D Yes D Sometimes10) Do you feel handicapped by a hearing problem? . D NoD Yes D Sometimes11) Does a hearing problem cause you to visit friends, relatives,or neighbors less often than you would like? . D No D Yes D Sometimes12) Do you experience ringing or noises in your ears? . D No D Yes D Sometimes13) Do you hear better with one ear than the other? . . D No D Yes D Sometimes14) Have you had any significant noise exposure during work,recreation, or military service? . . . D No D Yes D Sometimes15) Have any of your relatives (by birth) had a hearing loss? . D No D Yes D Sometimes
ruyo::Patient Name: - - - - - - - - - - - - - - - - - - - -Date of Birth:Please write your answer in the space provided.1) Little interest or pleasure in doing things.2)Feeling down, depressed, or hopelessKey:0-Not at all1-Several days 2-More than half the days3-Nearly everydayPlease check the appropriate answer.1) Are you afraid of falling?D NoDYes2) Have you fallen in the past year?DNoDYes3) If yes, circle the circumstances surrounding the fall.Answers:Tripped over somethingLightheadedness or palpitations prior toLoss of consciousnessInjuredNeeded to see a doctorAble to get up on ownDo you have an Advanced Directive (living will)? D No D YesNotes:Authorized Signature: - - - - - - - - - - - - - - - - - - - - - - Date:Reviewed by:Date:J
Please list any health problems and causes of death if applicable. Father Mother Brother(s) Sister(s) Mother's father Mother's mother Father's father Father's mother Living I Deceased Age Medical Problems