Transcription
DIRECTIONS TO DR. AMIREH’S OFFICEFROM FREEWAY 41, GO EAST ON HERNDON TO CEDAR.LEFT ON CEDARLEFT ON ELEVENTH (WHICH IS 1ST STOP LIGHT)TURN RIGHT INTO 4TH DRIVEWAY ON THE RIGHTOFFICE IS LOCATED AT THE VERY BACK, LAST OFFICE ON THE LEFT1642 E. HERNDON #106FRESNO CA, 93720IF YOU HAVE ANY QUESTIONS CALL OUR OFFICE(559) 447-1432****DO NOT GOOGLE, GPS, NOR MAP QUEST OUR ADDRESS BECAUSE IT WILL TAKE YOUTO A DIFFERENT LOCATION****PLEASE COMPLETE NEW PATIENT PACKET TO THE BEST OF YOUR ABILITY AND BRINGWITH YOU THE DAY OF YOUR APPOINTMENT. PLEASE ARRIVE 3O MINUTES PRIOR TOYOUR SCHEDULED APPOINTMENT IF YOU HAVE QUESTIONS ON HOW TO FILL OUT THEPACKET. PATIENTS WHO ARRIVE TO THEIR SCHEDULED APPOINTMENTS WITHOUTMAJORITY OF THE PATIENT PACKET COMPLETE WILL BE RESCHEDULED. THANK YOU1
Valley Pain ManagementNew Patient PacketPatient’s NameDOB DateChief ComplaintGENERAL HISTORY1) Have you ever had or do you have an allergic reaction to medication or IV dye? YES NOIf yes please list the medication2) Do you have a history of MRSA? YES NO if yes, what year3) Are you seeing a cardiologist? Yes No if yes, please list:4) Do you have a pacemaker and or AICD/defibrillator: YES NO date of implant:manufacture:5) Are you on any blood thinners? YES NO if yes, name of medicationand name of the prescribing doctor:6) Have you had any problems with anesthesia? YES NOSPECIFIC MEDICAL HISTORY YES NO Asthma/COPD YES NO Stroke YES NO Hepatitis YES NO Kidney trouble YES NO Diabetes YES NO Seizures Yes NO Hx. Of Cancer YES NO Meningitis YES NO Paralysis YES NO Thyroid Problems YES NO High Blood Pressure YES NO Heart troubleExplain in detail:Other illness not mentioned?SURGICAL HISTORYHave you ever had surgery within the last 5 years? Please list:2Year
CONTINUE ON BACK PAGE Medications: Please list all medications you are currently taking or bring a list – thank youMedication:TestXrayMRICT scanBone scanNCS/EMGNoneDose:Frequency:Please indicate which diagnostic test(s) you have had done:Whenwhat facility3
PATIENT DEMOGRAPHICSDATE:Last Name: First Name:Date of Birth:Age: Sex: M FHome Phone:Work Phone:Cell Phone: SSN:Mailing Address:City: Zip Code:Email Address:Emergency Contact 1 & Relation: Phone:Emergency Contact 2 & Relation: Phone:INSURANCE INFORMATIONPrimary Insurance:Secondary Insurance:Name of primary holder other than yourself:Is This Work Related? Yes NoClaim #DOB:If yes, what is date of injury?Adjuster Name & Number:Is this A Personal Injury Case: YesNo If yes, need Attorney Information:Attorney Phone: Fax:Responsible Party if Patient under the age of 18:Referring Physician:Primary Care Physician:Assignment of BenefitsI understand that this authorization allows the release to Anesthesia Consultants of Fresno of the medicalbenefits for services rendered.Signature:4Date:
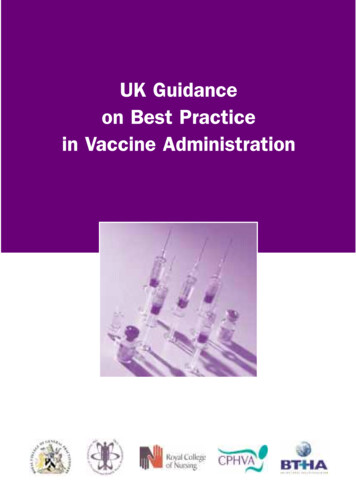
In which part of the body do you feel the pain? (Please indicate inthe diagram below).5
GnawingYes No SharpYes No ShootingYes No SpasmodicYes No SqueezingYes No StabbingYes No ThrobbingYes No Toothache like Yes No Vague PainYes No Associated SymptomsDizzinessYes No FeverYes No HeadacheYes No Joint PainYes No Muscle AtrophyYes No Muscle SpasmsYes No MyalgiaYes No NauseaYes No NumbnessYes No TinglingYes No WeaknessYes No Weight lossYes No Aggravated SymptomsAny activity or movementYes No Describe:Bending overYes No Bending to the sideYes No CarryingYes No Climbing StairsYes No Cold EnvironmentYes No Coughing/SneezingYes No Doing excessive workYes No DrivingYes No ExerciseYes No ExtensionYes No FlexionYes No Head TiltingYes No HeatYes No Keyboard typingYes No LiftingYes No Overhead movementYes No Overhead workYes No Prolonged sittingYes No Prolonged standingYes No ValsalvaYes No WalkingYes No Sensitive to touchYes No Chief Complaint: lower or upper extremities Low back pain Low back pain radiating to bilateral LE Low back pain radiating to left LE Low back pain radiating to right LE Neck pain Neck pain radiating to bilateral UE Neck pain radiating to left UE Neck pain radiating to right UE Foot pain Hand pain Other (where)Onset of Pain / / Date Days Weeks Months Years OtherWhat triggered your pain Carrying/ Lifting Bending/ Twisting Pushing/ Pulling Fall MVADo you have an attorney Yes NoAre you presently involved in litigation? Yes No OtherHPIPain Level 0- Pain free 1-3 Mild pain 4-6 Moderate pain 7-9 severe pain 10 Extreme/Excruciating painPain DescriptionAchingBurningYes No Yes No ColickyConstrictingCrampingDullYes Yes Yes Yes No No No No 6
Weight ChangesYes Flu VaccinationYes If yes, when:MusculoskeletalLimitation of movementYes Muscle crampsYes Back painYes Bone painYes Joint painYes Muscle painYes StiffnessYes Joint swellingYes SkinChange in hair or nailsYes Dry skinYes Mole changesYes RashesYes Skin discolorationYes UlcerationsYes Recurrent skin infectionsYes What helps Relieve the PainApplication of ColdYes No Application of HeatYes No Lying SupineYes No MassagingYes No MedicationYes No RestYes No SittingYes No StretchingYes No Other comments:Treatments TriedPrescription MedicationYes No HeatYes No IceYes No Physical TherapyYes No For how long:Tens UnitYes No AcupunctureYes No ChiropracticYes No For how long:NeurosurgeryYes No MassageYes No InjectionsYes No What kind: circle one or more:No No No No No No No No No No No No No No No HEENTYes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes No No No No No No No No No No No No No Yes Yes Yes RespiratoryCoughYes HemoptysisYes Nocturnal choking/gaspingYes Shortness of breathYes TB exposureYes WheezingYes No No No HeadachesBlurred visionCataractsChanges in visionDizzinessDouble sUse of hearing aidsVertigoLumbar ESI’s SI injectionfacet injectionsscsIT pumpcervical ESI’sOther:Quality of SleepPlease circle one:PoorNormalInsomniaUnremarkableNeckNeck PainStiffnessEnlarged thyroidREVIEW OF SYMPTOMSGeneralChange in appetiteChillsFatigueFeverNight sweatsWeaknessNo No Yes Yes Yes Yes Yes Yes No No No No No No 7No No No No No No
CardiacChest painEdemaHigh blood pressureIrregular heartbeatPalpitationsShortness of breathYes Yes Yes Yes Yes Yes GastrointestinalAbdominal painYes Change in bowel habitsYes ConstipationYes DiarrheaYes HeartburnYes NauseaYes Change in bowel habitsYes Social History:No No No No No No Marital Status: circle oneMarriedSingleSeparatedDivorcedCommon lawWidowedDomestic partnerDo you smoke Yes No Caffeine Intake Yes No CoffeeSodasTeaEnergy drinksNo No No No No No No Alcohol intake: circle oneNoneOccasionallySeldomdailyUrinaryYes Yes Yes Yes Yes No No No No No NeurologicalYes Yes Yes Yes Yes Yes No No No No No No DysuriaFrequencyHematuriaUrinary incontinenceFlank essPeripheral VascularCrampsYes Intermittent claudicationYes Varicose VeinsYes EndocrineHeat or cold intoleranceYes Excessive sweatingYes DiabetesYes Excessive urinationYes PsychiatricAnxietyYes DepressionYes Sleep disturbanceYes IrritabilityYes Mood swingsYes Do you consume illicit drugs: Yes No What is your education level?Grammar schoolHigh SchoolCollegePost GraduateOther:What is your occupation? Please circle:EmployedJob TitleUnemployedWorker’s CompensationPermanently DisabledOther:No No No No No No No THANK YOU FOR FILLING OUT OUR FORMS No No No No No 8
directions to dr. amireh's office from freeway 41, go east on herndon to cedar. left on cedar left on eleventh (which is 1st stop light) turn right into 4th driveway on the right office is located at the very back, last office on the left 1642 e. herndon #106 fresno ca, 93720 if you have any questions call our office (559) 447-1432