Transcription
2011 Pro g ram Y eaRCancer Program Annual ReportSumma Akron City andHospitalsSt. Thomas HOspitalsim pro vin g outcom es w ith p er s o n a l i z e d t r e a t m e n t s
Contents3Summa Health System4Medical Director’s Report6Melanoma Report 20118Melanoma – Volumes, Demographics, Survival Rates11Cancer Registry Summary 201112Statistics 2011 Primary Sites15Reports16C olon Cancer: Reducing Time to Initiation of ColonCancer Adjuvant Chemotherapy Following Surgery18Accomplishments20Clinical Trials Review22Clarence’s Story: Ipilimumab Clinical Trial ECOG160826Russell’s Story: Ipilimumab Clinical Trial ECOG160829Cancer Committee Members 201130Definition of Terms31Locations – Cancer Care Centerswww.summahealth.org/cancer
Summa Health SystemSumma Health System – headquartered in Akron,Ohio – is one of the largest integrated healthcaredelivery systems in the state. Formed in 1989 withthe merger of Akron City and St. Thomas Hospitals,this nonprofit system now encompasses a network of: Hospitals Community-based health centers A health plan A multi-specialty group practice An entrepreneurial entity Research and medical education Multiple foundationsSumma serves more than one million patients eachyear in comprehensive, acute, critical, emergency,outpatient and long-term/home-care settings andrepresents more than 2,000 licensed inpatient bedsin the following clinical settings: Summa Akron City Hospital Summa Barberton Hospital Summa St. Thomas Hospital Summa Wadsworth-Rittman Hospital Summa Western Reserve Hospital Summa Rehab Hospital Robinson Memorial Hospital, an affiliate ofSumma Health System Crystal Clinic Orthopaedic CenterOutpatient care is extended throughout Summit,Portage and Medina counties in multiple communityhealth centers. Providing superior, multi-specialtypatient care, medical research and continuingmedical education, Summa is consistently rankedone of the best healthcare providers in the country.Various Summa Health System hospitals, servicelines, joint ventures and affiliates are recognized bythe following organizations: American College of Surgeons Commission onCancer (CoC) American Nurses Credentialing Center American Osteopathic Association’s HealthcareFacilities Accreditation Program (HFAP) Centers for Medicare and Medicaid Services Magnet Recognition by American NursesCredentialing Center National Accreditation Program for BreastCenters (NAPBC) Premier Healthcare Alliance The American Heart Association The Joint Commission on the Accreditation ofHealthcare Organizations Thomson Healthcare (formerly Solucient) U.S. News & World ReportOur MissionThe mission of Summa Health System is toprovide the highest quality, compassionate care toour patients and members and to contribute to ahealthier community.Our VisionSumma Health System will be recognized asone of the finest healthcare organizations in theUnited States and will be the preferred provider ofhealthcare services in our service area.Our Values Personal and organizational integrityQuality, caring organizational environmentExcellence in leadershipValuing one anotherIndividualityRespect and fair treatmentOpen communicationsTeamworkCommunity serviceS U M M A H E A LT H . O R G / C A N C E R3
Medical Director’sR eportAs we look back over 2011, we see continued development and progress in thecancer program at Summa Health System. Summa provides the majorityof cancer care in the Akron region with 1,303 analytic cases accessioned atSumma Akron City and St. Thomas Hospitals.These newly-diagnosed cases represent a broadspectrum of malignant diseases. The data reflectsthe national experience with cancer as reported inthe literature, with about two-thirds of patientsbeing age sixty or older.Three-fourths of Summa’s oncology patients areresidents of Summit County, with the remaining 25percent drawn from communities in Portage, Stark,Medina and Wayne counties.Breast cancer remains the most commonly diagnosedmalignancy, while lung cancer continues to be thesecond most frequently diagnosed malignancy.Other frequently noted malignant diagnoses include:colorectal, prostate, lymphoma, uterine cancer andbladder.Patients are given the opportunity to participatein investigational clinical trials utilizing the latestavailable drugs and treatment techniques.Eight percent of Summa’s patients chose thisoption for their care, which is well above thenational average of less than one percent. Thislevel of participation in clinical trials qualifies aprogram for recognition at the “commendation”level by the American College of SurgeonsCommission on Cancer, an honor which fewprograms earn.Highlights from 2011 include: Accredited by the American College of SurgeonsCommission on Cancer, with commendation(CoC) U .S. News & World Report named SummaAkron City and St. Thomas Hospitals as #1 forcancer care in Akron4CANCER PROGRAM 2 0 1 1 ANNUAL REPORT
O ncology nursing staff participated in theMagnet Survey, which validated the high qualityof nursing care patients receive at Summa AkronCity and St. Thomas Hospitals A process improvement intervention led byFred Slezak, M.D., and Sameer Mahesh, M.D.,shortened the time between patients’ colorectalcancer surgery and when adjuvant chemotherapycould begin, which improves patient outcomes C ontinued participation in several communityoutreach programs, including: An evidence-based survivorship programknown as “A Time to Heal” he successful “I Can Cope” program wasTagain offered in 2011 he “Breast Education and ScreeningTTogether” (BEST) program provides freescreening and diagnostic mammograms towomen. Summa Screens” project created to“encourage age-appropriate cancer screeningfor women P romotion of Kim Moeller, MSN, RN, ACNSBC, OCN to manager for outpatient infusion atthe Cooper Cancer Center P romotion of John Shanahan, MS, DABR tochief medical physicist of Radiation OncologyIn this report, Dr. John A. Jakob provides anoverview of new treatment options for patients withadvanced melanoma. Also included are two articleswhich share the unique perspectives of two patientswith melanoma who are participating in the clinicaltrials of these new drugs.R. Douglas Trochelman, M.D.Medical DirectorOncology Service LineSumma Health System A dded new staff member, hematologist andmedical oncologist, John Jakob, M.D., to themedical staff of Summa Health Center at LakeMedina and Parkview Cancer CenterS U M M A H E A LT H . O R G / C A N C E R5
MelanomaR eport 2 0 1 1John Jakob, M.D., Ph.D.Medical Oncologist and HematologistSumma Health SystemJohn A. Jakob, M.D., Ph.D. is board-certified in internalmedicine, medical oncology and hematology, with adoctorate in cancer genetics.Breakthroughs in the treatment of advanced melanomaAdvanced melanoma, a skin cancer, is an oftenlethal condition which claims 8,000 to 10,000 livesannually in the United States.Despite intense research conducted during the past40 years, very few advances were made in extendingthe survival of these patients.VemurafenibandIpilimumabThese two recently approved, very different, therapieshave been shown to improve the survival of advancedmelanoma patients at Summa and in national studies.6CANCER PROGRAM 2011 ANNUAL REPORTThis changed in 2009, when vemurafenib, a neworal medication, was found to produce dramaticresponses in some patients with advanced disease.Subsequently, vemurafenib was also shown toincrease survival in patients with susceptible tumors.In 2010, ipilimumab, an antibody given as anintravenous (IV) therapy, was shown to improvethe survival of advanced melanoma patients. Bothvemurafenib and ipilimumab, two very differenttherapies, were approved by the FDA for use inpatients with advanced melanoma.Vemurafenib, the oral agent, is also known asZelboraf, its commercial name. It inhibits the B-RAFprotein, whose activation by genetic mutationis found in roughly half of advanced melanomatumors; the B-RAF protein is involved in regulationof cell growth.
96%of cancer cases were diagnosed in men and women age 40 andover at Summa’s Akron City Hospital in 2011.Not surprisingly, a patient’s tumor (but not thepatient!) must be tested for a mutation in theBRAF gene to determine eligibility for vemurafenibtreatment. The test can take ten days to complete,but if the mutation is found, then the patient is anappropriate candidate for vemurafenib therapy.Vemurafenib is administered as four 240-mg. tabletstaken twice daily. This therapy is strictly outpatient,with only periodic visits to a medical oncologistrequired. Generally, it is well tolerated; however,some patients experience fatigue, rashes, and skinphotosensitivity.There is also a risk of secondary skin cancers,consisting of unrelated, distinct tumors calledsquamous cell carcinomas which can be treated withthe assistance of a dermatologist and/or surgeon.The new IV therapy, ipilimumab, has severaldifferences when compared with vemurafenib, theoral therapy. Ipilimumab effectively reprogramsthe body’s immune system to aggressively fight themelanoma cancer cells. Importantly, all patients withadvanced melanoma are eligible for this treatment,regardless of the status of their tumor’s BRAF gene.The term “melanoma” denotes several subtypesof cancer, including: “mucosal” (arising from themucous membranes) and “acral-lentiginous” (arisingon the hands and feet). These types of melanomasometimes harbor mutations in the c-KIT gene andare a very active area of investigation. Lastly, “uveal”melanoma, a tumor that arises in pigment cells ofthe eye, is a rare condition whose genetic profile hasbeen clarified in the past two years.In summary, the care of patients with advancedmelanoma has changed greatly during the pasttwo years, with FDA approval of two medications,ipilimumab and vemurafenib. Although thesemedications differ in mechanism and meansof administration, they both extend survival inmetastatic disease. Our oncologists work with ourpatients with this diagnosis to formulate a care planto utilize these new therapies in an effective fashionin order to maximize patient outcomes and qualityof life during treatment for advanced melanoma.In addition, this therapy must be given in atraditional chemotherapy unit. Ipilimumab alsohas a unique side effect profile; because the body’simmune system has been “activated,” inflammationof the gastrointestinal tract, liver and skin canpresent unique challenges for the patient and his/her oncologist.S U M M A H E A LT H . O R G / C A N C E R7
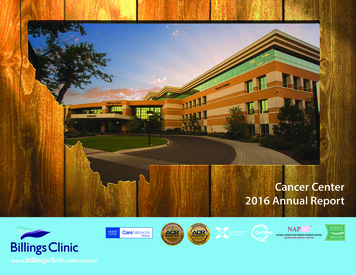
MelanomaVolumes, Demographics, Survival RatesG raph 12011 Melanoma Cases – HistologiesSumma Akron City and St. Thomas Hospitals – 28 casesAcral LentiginousMalignant Melanoma1Melanoma in situ1Superficial SpreadingMelanoma2Malignant Melanoma240510152025G raph 22011 Melanoma Cases – Age at DiagnosisSumma Akron City and St. Thomas Hospitals – 28 392%40-4950-5960-6970-7980-89G raph 32011 Melanoma Cases – Race DistributionSumma Akron City and St. Thomas Hospitals – 28 cases8Caucasian97%African American3%CANCER PROGRAM 2011 ANNUAL REPORT90-9930
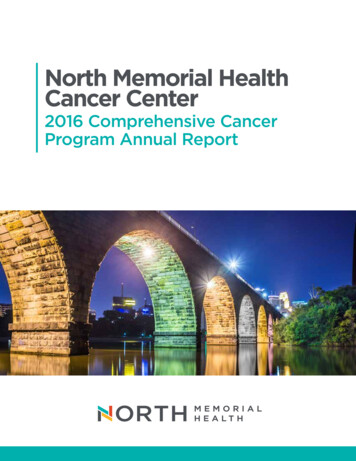
G raph 4Melanoma Five-Year Survival by AJCC StageSumma Akron City and St. Thomas Hospitals (Cases DXD 2003-2005)100%89%78%78%80%60%50%40%20%0%n/aStage IStage IIStage IIIStage IVAll StagesG raph 5Melanoma Five-Year Survival by Year – All StagesSumma Akron City and St. Thomas Hospitals (Cases DXD 2003-2005)100%80%60%40%20%0%Year 1Year 2Year 3Year 4Year 5G raph 6Melanoma Five-Year Observed Survival – By StageSumma Akron City and St. Thomas Hospitals (Cases DXD 2003-2005)100%Stage IStage II80%Stage III60%N/AStage IV40%20%0%Year 1Year 2Year 3Year 4Year 5S U M M A H E A LT H . O R G / C A N C E R9
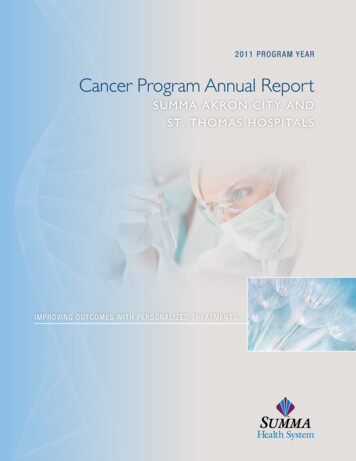
G raph 7Melanoma Five-Year Observed SurvivalNational Cancer Database (Cases DXD 2003-2005)100%Stage 0Stage I80%Stage II60%Stage III40%Stage IV20%0%Year 0Year 1Year 2Year 3Year 4Year 5G raph 82011 Analytic Melanoma Cases by AJCC StageSumma Akron City and St. Thomas Hospitals – 28 casesNCDB – 40,926 cases80%70%Summa Akron Cityand St. Thomas 10%0%0%Stage 0Stage IStage IIStage IIIStage IVG raph 92011 Melanoma Cases – Gender DistributionSumma Akron City and St. Thomas Hospitals10Male46%Female54%CANCER PROGRAM 2011 ANNUAL REPORT5%
Cancer RegistrySummary 2 0 1 1The cancer registry is an essential component of theCommission on Cancer accredited cancer program.The Cancer Program at Summa Akron City and St.Thomas Hospitals achieve their goals by collectingand reporting quality cancer data in support of theirbusiness planning and outreach initiatives.Data collected by the cancer registry is an invaluabletool in the fight against cancer. As an accreditedCoC facility the registry collects demographicand disease specific data elements on each cancerpatient presenting for diagnosis or treatment. Theinformation collected is utilized by physicians,administration and other healthcare professionals.Among the many uses are: Measuring quality outcomes Tracking community outreach initiatives Supporting clinical, diagnostic, and treatmentresearch Evaluating the effectiveness of current treatmentmodalities Presenting data for individualized patienttreatment planning Submitting to local and national databases forincidence and outcome comparisonS U M M A H E A LT H . O R G / C A N C E R11
Statistics2011PrimarySitesSumma Akron City& St. ThomasHospitalsPrimary SiteTotalAll Sites1302MF566736Class of 0810Non-Hodgkin's723537690Corpus wn 5231Other Digestive Sites221111221Esophagus20164202Ovary20020180Other Oral Sites15105140Stomach1495140Larynx1192101Multiple Myeloma1129110Connect/Soft Tissue1156100Cervix Uteri11011100Brain (Malignant)1156100Vulva10010104Anus/Anal Canal93690Liver95490Tongue73470Other Brain Sites62460Hodgkins62460Other Skin55050Other Female Sites40430Testis44040Nasal/Sinus32130Other Blood/Bone her Chest Sites22020Bone21120Other Urology Sites21120Hypopharynx11010Brain (Benign)101001303566737126240Total12SexCANCER PROGRAM 2011 ANNUAL REPORT
45%of all new cancer cases diagnosed in 2011 at Summa Akron City andSt. Thomas Hospitals were breast, lung or colorectal cancers.2011 Data SummarySumma Akron City Hospital’s cancer registryaccessioned 1,303 new cancer cases for 2011. Thefollowing graph illustrates the most frequent primarysites seen at this facility.Top Five SitesSumma Akron City and St. Thomas n-Hodgkin'slymphoma72050100150200250Number of CasesThe top five sites for all patients are breast, lung,colorectal, prostate and non-Hodgkin’s lymphoma.The gender distribution for these top sites isrepresented in the graph below.Female/Male Top SitesSumma Akron City and St. Thomas Hospitals250MaleFemale200Numberof kin'slymphomaS U M M A H E A LT H . O R G / C A N C E R13
DemographicsThe majority (74 percent) of the patients presentingto Summa Akron City and St. Thomas Hospitalsreside in Summit County. This is represented by thefollowing chart.County of Residence Primary Payor at DiagnosisSumma Akron City and St. Thomas Hospitals14SUMMIT 74%HMO51%PORTAGE 11%MEDICARE33%MEDINA5%MEDICAID6%STARK4%INSURANCE NOS 6%WAYNE2%NOT INSURED4%OTHER4%OTHER1%Follow-UpContinuing EducationMeaningful survival and outcome measures requirereliable tracking of disease, recurrence and vitalstatus for the lifetime of each patient record.Accurate follow-up data enables Summa to compareoutcomes with regional, state or national statistics.The successful follow-up rate at Summa Akron Cityand St. Thomas Hospitals for the last five yearsis 92% and the rate since the established registryreference year (2000) is 87%. Both rates are abovethe CoC requirement of 90 percent and 80 percentrespectively.In 2011 registry staff attended the Ohio Associationof Cancer Registrars 41st Annual EducationConference, the NAPBC Pursuing ExcellenceThrough Accreditation Workshop and the FourthAnnual Vincent and Nancy DiGirolamo OncologySymposium in addition to other local and regionalevents.CANCER PROGRAM 2011 ANNUAL REPORT
2011 ReportsProfessional EducationEight cancer-related educational activities wereheld in 2011DatePrograms01/2011Shaping the Future – An Overview Presentation on the 7th Edition AJCC Cancer Staging Manual01/2011NCDB Edits – Find-Correct – Submit Error Free02/2011Understanding the NAPBC Components and Standards06/2011Oncology Nursing Society Chemotherapy/Biotherapy Course07/2011Entering the Era of Personalized Medicine in Non-Small Cell Lung Cancer08/2011Summa Thinks Pink 2011 Starting the Conversation10/2011The Fourth Annual Vincent and Nancy DiGirolamo Oncology Symposium12/2011How to Find What the Edits MissCancer Conferences 2011During 2011, there were 52 Cancer Conferencesconducted. Case specific presentations included401 cases. Of these case presentations, 401 wereprospective and none were retrospective.52Cancer Conferencesconducted in 2011SUMMAHEALTH . ORG / CANCER15
Colon CancerREDUCING TIME TO INITIATIONOF COLON CANCER ADJUVANTCHEMOTHERAPY FOLLOWING SURGERYA presentation at an American Society of ClinicalOncology (ASCO) Gastrointestinal CancersSymposium inspired Summa oncologist SameerA. Mahesh, M.D. to think about ways to improveoutcomes for colorectal cancer patients.1Colorectal cancer is the third leading cause of cancermortality in the Western world.2 Surgery, followedby adjuvant chemotherapy (AC), has been provento improve overall survival in certain patients withcolon cancer after surgery.However, a recent data analysis suggests that alonger time to AC is associated with worse survivalamong patients with resected colorectal cancer. Infact, the results indicated relative overall survivaldecreases by 14 percent for every four-week delayin initiation of AC.Study findings suggest that timing of AC plays acritical role in the management and outcomes ofpatients with colorectal cancer and clinicians shouldtake steps to avoid delays in access to chemotherapy.Dr. Mahesh also is the process improvement directorfor Summa’s oncology services department.The results of the meta-analysis intrigued him. Hedecided to take a second look at the elapsed timebetween surgery and the initiation of chemotherapyat Summa’s Cooper Cancer Center.The analysis showed 24 percent of patientsundergoing colon cancer surgery in 2010subsequently received chemotherapy followingsurgery. The process took a median of 41 days fromdate of discharge to the patient’s first chemotherapysession (a range of 12 to 166 days).Dr. Mahesh knew this was an opportunity toimprove patient outcomes, but he also knew heneeded help.A multidisciplinary team comprised of anoncologist, surgeon, administrator, cancercare nurse navigator and Six Sigma processimprovement experts was formed with the goalof reducing the time it took for a patient to beginadjuvant chemotherapy following surgery.The first step was analyzing how patients flowedthrough the colorectal cancer treatment process.Previously, starting AC was a serial process,beginning with:1. Patient’s post-operative visit to surgeon2. Patient’s initial visit to medical oncologist3. Surgical placement of port in patient4. Initiation of adjuvant chemotherapy in patientBiagi JJ, Raphael M, King WD, Kong W, Mackillop WJ, Booth C. The impact of time to adjuvant chemotherapy (AC) on survival in colorectal cancer (CRC): A systematicreview and meta-analysis. J Clin Oncol 29: 2011 (suppl 4; abstr 364)2Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin, 2005:55(2):74-108.3 Biagi JJ, Raphael M, King WD, Kong W, Mackillop WJ, Booth C. Association between time to initiation of adjuvant chemotherapy (AC) and survival in colorectal cancer(CRC): A systematic review and meta-analysis. JAMA, 2011; 305(22):2335-2342. Published online June 4, 2011.1 16CANCER PROGRAM 2011 ANNUAL REPORT
Sameer A. Mahesh, M.D.Hematology/Medical Oncology“All of the steps in theprocess were scheduledand completed serially,”said Dr. Mahesh. “This wasinefficient, for both patientsand clinicians. And, moreimportantly, it delayedthe start of a patient’schemotherapy.”“We knew we could do better,” he said. “Instead ofa sequential, serial process, what was needed was forthese steps to be scheduled concurrently.”The team’s goal was to reduce the time from amedian of 41 days to a median of 28 days as wellnarrow down the standard deviation.In order to accomplish their goal, the team beganto look at their clinical processes from a differentperspective.“We initiated a program of concurrent scheduling ofappointments by the colorectal cancer nurse navigator(CRCN) which began as soon as the pathologyreport became available,” Dr. Mahesh said.Utilizing the CRCN to coordinate appointmentsfor patients who required adjuvant chemotherapysignificantly reduced the time to start ofchemotherapy from date of discharge, moving froma median of 41 days to 27 days.Dr. Mahesh and his team expect this successto eventually translate into better colon canceroutcomes for patients as well as increase patientsatisfaction since moving through the system wouldbe a quick and effortless processAnother plus – the change required no additionalfunding.Reasons for a delay in time to AC may be due topatient factors such as postoperative complications,comorbid conditions or health system logistic factorssuch as delays in referral or wait times.With healthcare reform efforts and increasingdemands for transparency from healthcare consumeradvocates, timely access to adjuvant chemotherapywill be cited and tracked as a quality indicator.Clinicians should reexamine their clinical processesand take steps to eliminate bottlenecks andinefficiencies.Dr. Mahesh has some advice for other healthcareproviders looking to improve their own clinicalprocesses and patient outcomes.“Analyze the process and eliminate or modifyroadblocks to improve patient care,” he said.“Sometimes, the solutions are quite simple.”ResultsnTTCD-days (median)Range (days)SD (days)Status prior to program194112-16631Status after program1627 (p 0.01)*12-6914* Modified Mood Median TestAUTHORS:Karen Bochert, Brian Rentschler, Chris Powers, Frederick Slezak, M.D., Sameer A. Mahesh, M.D., MBBS; Summa Health System, Akron, OHContact Dr. Sameer A. Mahesh at (330) 376-1043 ormaheshs@summahealth.org for more information about this project.S U M M A H E A LT H . O R G / C A N C E R17
Cancer Care ProgramA ccomplishments 2 0 1 1ProgrammaticClinical Developed System-wide order sets for chemo/infusions treatments American College of Surgeons Commission onCancer – Received three year accreditation with Cross-trained radiation and medical oncologystaff throughout the System Implemented Dietitian Services at the Coopercommendation.Cancer Center eight hours a week offering Applied for American College of Radiologyindividual counseling and group programs forRadiation Oncology Accreditationpatients Established data benchmarks; working toward Implemented a post acute treatmentNQMBC accreditation for the Breast Centerpsychosocial follow-up pilot for patients; began Continued to increase patient and familyrecruiting patients in the first quarter of 2011attendance to/participation in supportive careprograms Magnet status was achieved at Akron Cityand St. Thomas Hospitals. Oncology nursingstaff participated in the Magnet Survey whichvalidated the high quality of nursing carepatients receive at Summa.1 in Akron#18CANCER PROGRAM 2 0 1 1 ANNUAL REPORTU.S. News & World Reportnamed Summa Akron City and St. ThomasHospitals as #1 for cancer care in Akron.
QualityCommunity Outreach Conducted revision meetings in regards to the Expanded programming into Medina CountyMy Journey Treatment Planner for system-wide Applied for additional funding sources utilization and implement changes.to continue “Summa Screens,” Summa’s Utilized LEAN to improve patient care processesmammography program for the uninsured andQuality Improvement Projects Palliative Care – Sooner Than Later Patients to be served include those diagnosedwith Stage III & IV cancers: metastaticmelanoma or renal cell carcinoma, advancedlymphoreticular malignancy and any otherpatients who physicians and staff feelunderinsured. Increased patient, provider and staff awarenessand knowledge of common physical andpsychosocial needs of survivors as well as waysto access multi-disciplinary treatment resourcesat Summa Health System through in-servicetrainings and community presentationsincreased support for symptom control orpsychosocial support and spiritual supportmight be necessary Palliative Care consult can take place in thePalliative Care Clinic, Center for SeniorHealth, Radiation Oncology Center or theInfusion Center in the Cooper Cancer CenterPerformance Improvements Colon LEAN Project: Reducing Timeto Initiation of Colon Cancer AdjuvantChemotherapy Following Surgery (see article onpage 16).SUMMAHEALTH . ORG / CANCER19
Clinical TrialsR eviewMelanoma Clinical Trials at Summa Health SystemProtocol: ECOG 1609Protocol: ECOG 2607A Phase III Randomized Study of AdjuvantIpilimumab Anti-CGTLA4 Therapy versus HighDose Interferon alpha-2b for Resected High-RiskMelanomaA Phase II Trial of Dasatinib in KIT-Positive Patientswith Unresectable Locally Advanced or Stage IVMucosal, Acral and Vulvovaginal MelanomasEligibility Criteria: Stage IIIB or IIIC or IV, nomelanoma (acral, vagina and/or vulva or othermucosal surface); measurable disease, must be KITpositive, prior treatment allowed but no targetedtherapy permitted, prior treatment more than 4weeks before study entry, mandatory central tissuereviewocular or mucosal melanoma, completely resectedwith negative margins within 12 weeks of studyenrollment, no prior adjuvant treatment afterresection, recurrent melanoma included, more than30 days since radiation therapy and more than 4weeks since IL-2 or other chemotherapy20CANCER PROGRAM 2011 ANNUAL REPORTEligibility Criteria: metastatic or unresectable
100Over 100 active clinical trials are ongoingat Summa Health SystemThere’s only one way to end cancer: research“You have cancer.”Fifty years ago, many cancer treatments we take forgranted today did not exist.Currently, researchers are conducting more than100 clinical studies to evaluate a wide range ofnew treatment options, including surgical andradiation therapy techniques, various chemotherapycombinations and improvements in supportivecare for patients who are undergoing treatment forcancer.But by investing in clinical research, the NationalCancer Institute, along with pharmaceutical andbiotechnology companies, have made significantprogress in developing effective treatments for manyforms of cancer.Improving outcomes for cancer patients is a teameffort. Clinicians rely on patients’ participation inresearch studies to continue to improve care andoutcomes across the nation for all cancer patients –now and in the future.It’s only three words, but receiving a cancerdiagnosis changes everything. Not just for patients,but for everyone who loves and cares for them.These advances would not have been possiblewithout patients who chose to enroll in studies toevaluate the safety and efficacy of new treatments.Summa Health System supports one of themost active clinical research programs in theregion, participating in multiple national researchorganizations which are funded by the NationalCancer Institute and the pharmaceutical industry.For more information regarding cancer clinicalSumma researchers also have establishedcollaborative relationships with local universitiesand medical programs to expand opportunities forpatients to participate in clinical research studies.research and cancer registry,trials at Summa or for a complete list of openprotocols and corresponding sites, pleasecontact Joyce Neading, program director, cancer(330) 375-4221 or neadinja@summahealth.org.8%About eight percent of our patients (asopposed to the national average of lessthan one percent) participated in investigationalclinical trials offered at Summa.S U M M A H E A LT H . O R G / C A N C E R21
Clarence Rohr22CANCER PROGRAM 2 0 1 1 ANNUAL REPORT
Ipilimumab Clinical Trial ECOG1608Clarence’sIpilimumab (Yervoy) was shown to be thefirst treatment ever to improve overallsurvival in advanced melanoma patients.1S toryIt all began in 2006 when Clarence Rohr noticed asmall dark spot on his face.“I had just a little speck on my left cheek,” he said.Rohr, a soft-spoken, 84-year-old semi-retired farmerfrom Doylestown, Ohio, didn’t think it was anythingserious.“I went in and they took it out,” he said. “Thenthey told me I had the melanoma.”Clarence hoped the surgery to remove the lesionwould be the end of it. He was eager to get backto doing the things he loves - working with his twosons on their 135-acre family farm and helping themmanage Bass Lake, their fishing business.Bass Lake encompasses a series of 30 ponds andlakes which are stocked with various types of gamefish, including: bass, bluegill, striped bass, walleyeand crappie. It is open to weekend anglers andClarence also sells fish to people who wish to stocktheir own ponds. The Rohrs’ acreage also producesmore than 20,000 bales of hay each year to sell.Following the removal of the lesion on his cheek,Clarence returned to farming, tending the familygarden and helping anglers enjoy a day of fishing.Four years later, however, the melanoma returned.Clarence noticed new lesions on his ear and neck.In August 2010, Clarence made an appointmentwith Sameer A. Mahesh, M.D., an oncologist at theJean and Milton Cooper Cancer Center at SummaAkron City Hospi
Contents 3 Summa Health System 4 Medical Director's Report 6 Melanoma Report 2011 8 Melanoma - Volumes, Demographics, Survival Rates 11 Cancer Registry Summary 2011 12 Statistics 2011 Primary Sites 15 Reports 16 Colon Cancer: Reducing Time to Initiation of Colon Cancer Adjuvant Chemotherapy Following Surgery