Transcription
Foundations and Trends R in Electronic DesignAutomationVol. XX, No. XX (2018) 1–67c 2018 H. Yin, A. O. Akmandor, A. Mosenia and N.K. JhaDOI: 10.1561/XXXXXXXXXXSmart HealthcareHongxu Yinhongxuy@princeton.eduElectrical EngineeringPrinceton UniversityArsalan Moseniaarsalan@princeton.eduElectrical EngineeringPrinceton UniversityAyten Ozge Akmandorakmandor@princeton.eduElectrical EngineeringPrinceton UniversityNiraj K. Jhajha@princeton.eduElectrical EngineeringPrinceton University
Contents1 Introduction22 What is Smart Healthcare?2.1 The Smart Healthcare Framework . . . . . . . . . . . . .2.2 Clinical Healthcare . . . . . . . . . . . . . . . . . . . . . .2.3 Daily Healthcare . . . . . . . . . . . . . . . . . . . . . . .56893 Emerging Smart Healthcare Systems3.1 IBM Watson . . . . . . . . . . . . . . . . . . .3.2 Open mHealth . . . . . . . . . . . . . . . . . .3.3 HDSS: Health Decision Support System . . . .3.4 SoDA: Stress Detection and Alleviation System3.5 Energy-efficient Health Monitoring System . . .4 Design Considerations121314152027315 Innovations & Trends5.1 NeST: Synthesizing Compact Deep Neural Networks5.2 Compressive Sensing: Reducing Computation Loads .5.3 MedMon: Defending Against Wireless Attacks . . . .5.4 OpSecure: Exchanging Keys via Light . . . . . . . .5.5 SecureVibe: Exploiting the Vibration Side Channel . .ii.353538414649
iii6 Looking Forward6.1 Unsatisfactory Datasets and Machine Learning Models . .6.2 Protocol Standardization and Infrastructure Support . . . .6.3 Fog Computing as an Alternative to the Cloud . . . . . . .545455567 Conclusion59References61
AbstractInternet-of-Things and machine learning promise a new era for healthcare. The emergence of transformative technologies, such as Implantableand Wearable Medical Devices (IWMDs), has enabled collection andanalysis of physiological signals from anyone anywhere anytime. Machinelearning allows us to unearth patterns in these signals and make healthcare predictions in both daily and clinical situations. This broadens thereach of healthcare from conventional clinical contexts to pervasive everyday scenarios, from passive data collection to active decision-making.Despite the existence of a rich literature on IWMD-based and clinical healthcare systems, the fundamental challenges associated withdesign and implementation of smart healthcare systems have not beenwell-addressed. The main objectives of this article are to define a standard framework for smart healthcare aimed at both daily and clinicalsettings, investigate state-of-the-art smart healthcare systems and theirconstituent components, discuss various considerations and challengesthat should be taken into account while designing smart healthcare systems, explain how existing studies have tackled these design challenges,and finally suggest some avenues for future research based on a set ofopen issues and challenges.H. Yin, A. O. Akmandor, A. Mosenia and N. K. Jha. Smart Healthcare. Foundationsand Trends R in Electronic Design Automation, vol. XX, no. XX, pp. 1–67, 2018.DOI: 10.1561/XXXXXXXXXX.
1IntroductionA rapidly aging population and the dramatic increase in the cost ofin-hospital healthcare have led to the recognition of the importance ofefficient healthcare systems [Nia et al., 2015] and fostered several novelresearch directions at the intersection of healthcare, data analytics,wireless communication, embedded systems, and information security.Implantable and Wearable Medical Devices (IWMDs), which facilitatenon-invasive prevention, early diagnosis, and continuous treatmentof medical conditions, are envisioned as key components of modernhealthcare [Ghayvat et al., 2015, Mukhopadhyay, 2015, Mosenia et al.,2017b]. The computational power, energy capacity, and networkingcapabilities of IWMDs have improved significantly in the last decadewhile their sizes have decreased drastically. These technological advanceshave brought daily healthcare systems from a distant vision to the vergeof reality. Furthermore, the emergence of Internet-of-Things (IoT) andthe introduction of new computing/networking paradigms (such asCloud computing and Fog computing), which make possible systemsconsisting of several heterogeneous sensing and computing devices, haverevolutionized traditional healthcare and provided an opportunity toreplace in-hospital medical systems with Internet-connected IWMD-2
3based systems, thus bringing us to the dawn of a new era of smarthealthcare.Smart healthcare does not have a unique definition. However, ourbroad interpretation of smart healthcare is that besides clinical usage,it also utilizes IWMDs to gather, store, and process various types ofphysiological data during daily activities. Smart healthcare systems mayrely on wireless connectivity to take advantage of external resources,e.g., computational/storage resources available on nearby devices or theCloud, or inform a clinician about the patient’s medical condition. Hence,smart healthcare offers a proactive approach to early detection andeven prevention of medical conditions. It even enables physicians andclinicians to assist patients in their home environment where they can becontinuously monitored with the help of numerous Internet-connectedhealthcare systems. This reduces the need for institutionalization andhospitalization, and is especially beneficial to the disabled and elderly.It also has the potential to reduce healthcare costs significantly andenhance the quality of life of patients.Since the introduction of the first IWMD (an implantable pacemaker)in 1958, several types of IWMDs have been developed and introduced inthe market, ranging from sweat-analyzing devices [Gao et al., 2016] toInternet-connected multi-sensor continuous long-term health monitoringsystems [Nia et al., 2015, Pantelopoulos and Bourbakis, 2010]. However,despite a rich body of literature on IWMD-based and clinical healthcaresystems (see [Pantelopoulos and Bourbakis, 2010], [Mosenia et al.,2017b], and [Musen et al., 2014] for a comprehensive survey), thefundamental challenges associated with design and implementation ofsmart healthcare systems have not yet been well-addressed. The maingoals of this article are to define the scope of smart healthcare andinvestigate state-of-the art smart healthcare systems, their constituentcomponents, their design considerations, and how existing studies havetackled these challenges. In particular, we do the following. We present a novel framework for smart healthcare, which aimsto support both in-patient and out-patient health monitoring anddiscuss and compare clinical and daily healthcare. We describe several emerging smart healthcare systems, including
4IntroductionIBM Watson [High, 2012], Open mHealth [Estrin and Sim, 2010],Health Decision Support System (HDSS) [Yin and Jha, 2017],Stress Detection and Alleviation system (SoDA) [Akmandor andJha, 2017], and an energy-efficient system for continuous healthmonitoring of a patient’s medical condition over the long term[Nia et al., 2015]. We discuss several considerations and challenges that should betaken into account while designing smart healthcare systems. We describe five research trends for addressing these design considerations, including compact deep neural networks and compressivesensing to drastically reduce computation energy and storage, andMedMon, OpSecure, and SecureVibe to enhance security of healthcare systems. Finally, we discuss several future research directions, includingthe need to obtain medical datasets and machine learning modelsfor them, standardization and infrastructure, and the promisingrole that Fog computing can play in smart healthcare.The rest of the article is organized as follows. In Chapter 2, we presenta smart healthcare framework that enables exploitation of the rapidclinical-to-daily healthcare expansion. In Chapter 3, we analyze fiveemerging systems that act as enablers of smart healthcare. In Chapter 4,we discuss associated design considerations and challenges in thesesystems, including efficiency, security, accuracy, cost, responsiveness,maintainability, scalability, reliability and fault tolerance. In Chapter 5,we describe five emerging research trends that address some of thesechallenges. In Chapter 6, we discuss open issues and future researchdirections. Finally, we conclude in Chapter 7.
2What is Smart Healthcare?Modern healthcare saves human lives and improves the quality oflife. The average life expectancy has increased by five years in thepast two decades [Salomon et al., 2013]. The wide-ranging impact ofhealthcare on billions of people around the globe has spurred enormousinterdisciplinary research efforts and remarkable innovations. However,for decades, healthcare has been confined to clinics/hospitals. It hasfailed to utilize patient data obtained from the daily context, thusmissing out on the ability to catch a disease in its early stages. Recentyears have seen such deficiencies beginning to get addressed by advancesin daily healthcare enabled by IWMDs, i.e., Wearable Medical Sensors(WMSs) and Implantable Medical Devices (IMDs). The possibility ofdaily healthcare monitoring, in conjunction with conventional clinicalhealthcare, promises to usher in a new era of smart healthcare.In this chapter, we present a novel smart healthcare frameworkthat captures the rapid clinical-to-daily healthcare expansion. Thisframework defines the scope of smart healthcare, thus helps unifyvarious fragmented healthcare tasks under one umbrella.5
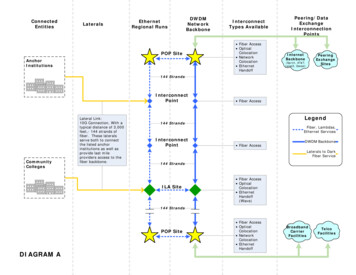
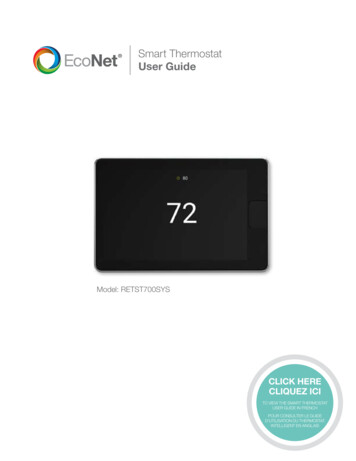
6What is Smart Healthcare?2.1The Smart Healthcare FrameworkDepending on where healthcare takes place, smart healthcare can bedivided into two major parts: (i) daily healthcare, depicted on the leftof Fig. 2.1, and (ii) clinical healthcare, depicted on the right of Fig. 2.1.These two parts are separated by the clinical boundary.The upper section of Fig. 2.1 summarizes the five major tasks thatneed to be carried out by smart healthcare: Disease prevention: (i) daily prevention Disease diagnosis: (ii) daily and (iii) clinical diagnosis Disease treatment: (iv) clinical and (v) daily treatmentsThese five tasks fall under three categories that correspond to the threemost critical challenges of modern healthcare: prevention, diagnosis,and treatment of human diseases. Each task constitutes a vibrantresearch field that includes challenging research topics such as fitnesstracking, daily disease diagnosis, physician variance reduction, treatmentplan selection, and precision medicine (summarized in bullet points inFig. 2.1). These five tasks need to be carried out in a sequential andcircular manner, as indicated by the arrows in Fig. 2.1. This directedloop is referred to as the smart healthcare loop.We call healthcare systems ‘smart’ when they have a decision-makingability. This ability is enabled by data analytics, as shown in the lowersection of Fig. 2.1. Information distillation starts with various data typesof interest that may assist decision-making. Data types vary from physiological and environmental readings in the daily context to physicianobservations and laboratory test results in the hospital/clinic. Thesedata must be efficiently captured, processed, and securely transmitted tothe upper levels of the healthcare system, assisted by machine learningengines, such as WEKA [Hall et al., 2009] and TensorFlow [Abadi et al.,2016], to extract health inferences. These health inferences form anintegral part of the tasks in the loop.
2.1. The Smart Healthcare Framework7Smart HealthcareDaily HealthcareClinical Boundary(ii) Daily Diagnosis WMS-based diagnosisClinical Healthcare(iii) Clinical Diagnosis Physician variance reduction Personalized diagnosis PME reduction(i) Daily Prevention Fitness checkupActivity trackingEmotion analysisDisease risk prediction(v) Daily Treatment Out-patient therapyAmbient healthcareDisease status monitoringPrecision medicine(iv) Clinical Treatment Systems & Analytics Health server Edge IWMDsMachinelearning engineSystems & Analytics CDSS EHRsData Physiological dataEnvironmental dataGenetic dataHistorical recordsDemographicsTreatment plan selectionTreatment method evaluationIn-patient monitoringPrecision medicineMachinelearning engineData Physician observationsLaboratory test resultsGenetic dataHistorical recordsDemographicsFigure 2.1: The smart healthcare framework.
8What is Smart Healthcare?Next, we zoom into clinical healthcare and then daily healthcareand discuss them in detail.2.2Clinical HealthcareDespite remarkable progress over the past few decades, the clinicalhealthcare system in the U.S. is still far from being optimal. For example,a recent study [Makary and Daniel, 2016] shows that PreventableMedical Errors (PMEs) accounted for more than 251,000 deaths in 2013,making it the third leading cause of death in the U.S. hospitals afterheart disease and cancer. This is substantially higher than the 98,000deaths due to preventable medical errors mentioned in the 1999 IOMreport [Kohn et al., 2000].Computerized information systems, e.g., Clinical Decision SupportSystems (CDSSs) and Electronic Health Records (EHRs), provide physicians and healthcare providers with intelligently filtered clinical suggestions, thus can greatly improve the quality of clinical healthcare.More than 66% of EHR-based CDSSs have been shown to significantlyimprove clinical practice in the long run [Hunt et al., 1998]. As a result,more hospitals and clinics are adopting CDSSs and EHRs to assistphysicians. This was aided by the Health Information Technology forEconomic and Clinic Health Act of 2009 that was accompanied by a 27B federal disbursement.The sharp increase in the amount of patient-specific clinical dataprovides a fertile resource for machine learning algorithms to derivehealthcare inference. Rapid algorithmic advancements in machine learning have even enabled super-human clinical decision-making performance. For example, a deep Convolutional Neural Network (CNN) hasbeen shown to perform on par with 21 board-certified dermatologistsin skin cancer classification [Esteva et al., 2017]. CheXNet, a 121-layerCNN, was able to beat the average performance of four radiologistsin pneumonia detection and analysis [Rajpurkar et al., 2017]. DeepPatient [Miotto et al., 2016] deploys a three-layer stack of auto-encodersto capture the regularities and dependencies in the aggregated EHRsof 700,000 patients. It uses the extracted rules for disease risk predic-
2.3. Daily Healthcare9tion and achieves very high accuracy on 76,214 test patients with 78diseases. With the help of massive parallel deep learning on Graphical Processing Units (GPUs), DeepBind analyzes millions of genomesequences (previously between 10,000 and 100,000) to identify causaldisease variants [Alipanahi et al., 2015]. This speeds up exploration ofrelationships among DNA, key molecules in cells, and associated diseaserisks, thus assisting with the development of precision medicine [Leunget al., 2016].However, clinical healthcare is still restricted to hospitals/clinics. Ithas very limited access to the daily health status of patients, a contextin which most diseases actually develop and are treated [Estrin and Sim,2010]. This can lead to many deficiencies. For example, daily health dataform an extremely important and sometimes the only information sourcefor physicians and CDSSs for making diagnostic decisions. Relying onself-reported symptom recalls from patients can be quite error-prone,given that symptoms often may not even be noticeable by an individual.These shortcomings point to the need to complement clinical healthcarein the daily scenario.2.3Daily HealthcareAs opposed to decades-long advancements in clinical innovations, dailyhealthcare is an emerging research field. It requires a steady, consistent,accurate, yet user-transparent, data acquisition mechanism. This hasonly been made feasible by recent advancements in low-power sensorsand signal processing techniques.The past decade has witnessed the deployment of many disruptivesensors in IWMDs, stationary sensors in house/office/gym, and embedded sensors in mobile phones. These sensors can consistently andpersistently collect vast amounts of health-related data in the dailycontext to enable decision-making. This falls under an IoT paradigmwhere things communicate and cooperate with each other pervasively toachieve common goals [Atzori et al., 2010]. The IoT framework containsthree hierarchical computation layers: sensor, edge, and the Cloud. Inthe context of healthcare, the three IoT layers sequentially transform
10What is Smart Healthcare?health-related data, such as physiological signals and environmentalreadings, into purposeful healthcare inferences, such as disease diagnosisand activity prediction, thus delivering smartness to daily healthcare.With the need to support billions of devices, the current IoT frameworksuffers from a limited sensor energy budget, constrained communication bandwidth, limited server storage, and a wide attack surface formalicious adversaries [Li et al., 2011, Halperin et al., 2008, Yin et al.,2015]. These shortcomings lead to significant design challenges, such asthe need for efficiency and security. We discuss these design considerations in Chapter 4 and the techniques to address these challenges inChapter 5.Hitherto, two major approaches have been used to obtain healthcareinference along the IoT hierarchy: A top-down approach from the Cloud: this approach starts fromthe Cloud to obtain population-level inferences and extract generalrules. The data amount that such an approach needs to tackleis large, typically terabytes (1012 B) or more. Consequentially,this approach suffers from high analysis costs for data collection,storage, and pre-processing. IBM Watson1 uses this approach, asexplained in detail in Chapter 3. A bottom-up approach from the sensor/edge: this approach startswith the user side to obtain individualized inferences. It typicallyassembles and analyzes the data from relatively smaller patientgroups. As a result, it enables a fine-grained analysis that canlead to more accurate individualized models. The amount of datathat needs to be analyzed is typically in the megabytes (106 B)to gigabytes (109 B) range, hence much smaller than the topdown approach. Hence, it reduces associated costs for machinelearning model generation. Examples using this approach includeOpen mHealth [Estrin and Sim, 2010], HDSS [Yin and Jha, 2017]and SoDA [Akmandor and Jha, 2017], as explained in detail inChapter 3.1IBM Watson, https://www.ibm.com/watson.
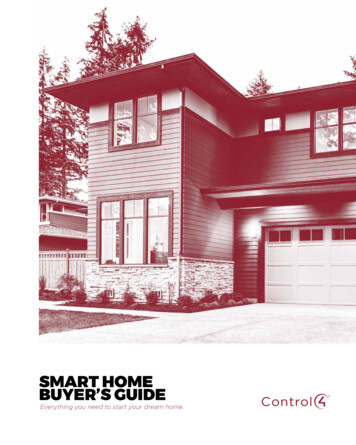
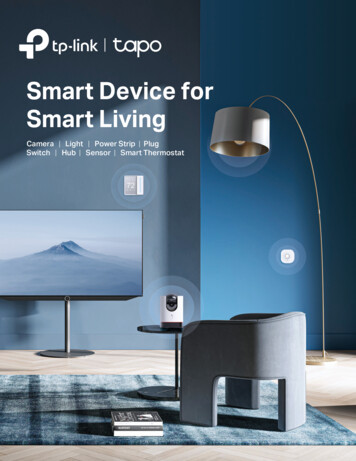
2.3. Daily Healthcare11Hybrid inference modeloutfinal H(out1, out2)General modelout1 G(input1)Individualized modelout2 I(input2)Training data acquisitionCloudSensor/edgeModel costHighLowData amountLarge (TB)Small (MB)/medium (GB)TargetGeneral rulesIndividual traitsFigure 2.2: A hybrid inference model for daily healthcare.However, neither approach is mature yet. A top-down approach,which yields a generalized population-level model, may fail to cater toindividual patients by not being able to accommodate his/her personaltraits. This is also a fundamental research question faced in personalizeddiagnosis and precision medicine. On the other hand, the bottom-upapproach, which yields an individualized model, is limited by the factthat analysis of data from a single patient group may fail to yield generalrules applicable at the population level. This may lead to inferencemodels that perform well within the group, but are not generalizableto other groups since the features may not be drawn from the sameprobability distribution.To address the above concerns, we describe a potential inferencemodel for smart healthcare as an ensemble of both generalized andindividualized models. We refer to it as a hybrid inference model, asshown in Fig. 2.2. The meta learner function H(·) accepts inputs fromboth the generalized function G(·) and individualized function I(·) asits base learners. This can effectively: tune a generalized model to each individual, given his/her personalphysiological traits, and augment an individualized model with additional ground truthsand larger knowledge base.
3Emerging Smart Healthcare SystemsThere is a need for ubiquitous healthcare to improve human well-being.Modern healthcare systems have become smart based on unprecedentedadvances in data analytics and increasingly pervasive based on rapiddeployment of IoT.In this chapter, we review several systems from the smart healthcaredomain, including: (i) IBM Watson that extracts rules from the medicalliterature to answer health-related questions [High, 2012], (ii) OpenmHealth that aims at daily chronic disease prevention based on datacollected from mobile phone applications [Estrin and Sim, 2010], (iii)HDSS that enables disease diagnosis based on WMSs and machinelearning ensembles [Yin and Jha, 2017], (iv) SoDA that focuses oncontinuous stress detection and alleviation via integration of WMS datawith machine learning algorithms [Akmandor and Jha, 2017], and (v) anenergy-efficient system that tackles continuous monitoring of a patient’smedical conditions over the long term [Nia et al., 2015].12
3.1. IBM Watson3.113IBM WatsonIBM Watson is a cognitive system that combines deep Natural Language Processing (NLP), hypothesis generation, and dynamic learningto generate confidence-based responses [High, 2012]. It is capable of condensing information from an immense amount of unstructured and noisydata: scientific articles, textbooks, user manuals, guidelines, frequentlyasked questions, plans, laboratory notes, news, and proprietary data.The extracted knowledge base is stored as a Watson corpus. Watsongenerates a unique corpus per target domain. Due to its significant NLPcapabilities, Watson has tackled a wide range of target domains, suchas engineering, medicine, law, and finance [Chen et al., 2016].Watson uses its corpus for question-answer style inferences. When anew question is raised, it (i) captures the main question features, (ii)acquires the candidate answers across hundreds of hypotheses generatedby the corpus, (iii) compares answers through reasoning algorithms,and then (iv) selects the answer that has the highest confidence score.This top-down approach, i.e., starting with reading all available information in the target domain, yields amazing results but at a very highcost. For example, IBM Watson won against human champions in theJeopardy Clash Knowledge Test in 2011. It read roughly 200M pagesof content to acquire its corpus to prepare for this test. It had to relyon 90 IBM Power750 processors and 16 terabytes of RAM during thecompetition [Chandrasekar, 2014].In the healthcare domain, Watson’s better-than-human contentreading capability enables it to answer health-related questions in bothdaily and clinical scenarios. It can scan and analyze content from a widerange of medical resources: scientific journals, patents, drug and diseaserelated ontologies, clinical trials, EHRs, laboratory and imaging data,genomic data, claims data, and web social content [Chen et al., 2016].This has led to three major applications of Watson in healthcare: Oncology: Watson can compare a patient profile with relevantclinical trials/records to evaluate and rank cancer treatment options. It cuts down time costs involved in reviewing the literatureand EHRs dramatically. For example, it took Watson 10 min-
14Emerging Smart Healthcare Systemsutes to finalize a treatment plan for a 76-year old brain-tumorpatient, while this process took human experts roughly 160 hoursto complete [Wrzeszczynski et al., 2017]. Drug discovery: Watson can identify novel drug targets and newuses of existing drugs. For example, it successfully identified 15 newdrug candidates for a malaria parasite from a drug candidate poolavailable from a pharmaceutical company [Chen et al., 2016]. Todo so, it first checked the literature, identified relevant drugs thathave been shown to be effective for malaria parasite mitigation,and then checked the candidate drug’s similarity in terms ofchemical structures and action mechanisms. Genomics: Watson can unearth new associations and relationshipsbetween genes, proteins, drugs, and diseases. It can also rank andpredict the most likely driver mutation and the alteration typeof DNA in a patient’s tumor to enhance personalized treatments.This provides physicians with more therapeutic options.3.2Open mHealthThe Open mobile Health (mHealth) project is aimed at daily chronicdisease prevention and management based on data collected from healthcare applications in mobile phones and devices [Estrin and Sim, 2010].There were more than 13,000 health-related applications available onApple’s iPhone by 2012 [Localystics, 2012]. These applications enablepatients to electronically record and track their vital physiological signson a daily basis, thus enabling satisfactory user-centered outcomes.For instance, WellDoc is a mobile phone based diabetes managementapplication that uses messages and prompts to track the glucose levelof its users [Quinn et al., 2011]. A randomized controlled trial observedthat WellDoc leads to a significant reduction in glycated hemoglobinamong its users and a 20% reduction in clinical visits and emergencycare usage [Quinn et al., 2011].Open mHealth aims to standardize the fragmented mHealth applications deployed on mobile phones. It proposes open Application
3.3. HDSS: Health Decision Support System15Programming Interfaces (APIs) built around a minimal set of commoncommunication protocols [Estrin and Sim, 2010, Chen et al., 2012]. Thisenables the sharing of data and application modules between variousdevices, across different operating systems, and over multiple chronicdiseases.InfoVis was the first standard data visualization tool developed inthe Open mHealth project [Chen et al., 2012]. It accepts data inputsfrom lower-level lego-like reusable software modules: Data ProcessingUnits (DPUs) and Data Visualization Units (DVUs). Each DPU andDVU performs a general-purpose task. Multiple DPUs and DVUs workcollaboratively to deliver application-level functionalities.Chen et al. have developed DPUs and DVUs for an mHealth application called Post-Traumatic Stress Disorder (PTSD) explorer that helpsPTSD patients manage acute distress symptoms [Chen et al., 2012].Mobile applications can offer unique standard care to PTSD patients,given that such patients seldom seek in-person consultation due to theattached stigma, logistical barriers, and hard-to-notice symptoms [Hogeet al., 2004]. The DPUs and DVUs enable a direct visualization ofthe self-reported PTSD checklist scores and blood glucose levels [Chenet al., 2012]. Given an open architecture based on shared APIs, thesePTSD DPUs and DVUs can also be used for other applications, suchas the visualization of self-reported chronic pain measurements frompatients [Chen et al., 2012].3.3HDSS: Health Decision Support SystemThe Health Decision Support System (HDSS) enables disease diagnosisin both in- and out-of-clinic scenarios through the integration of WMSdata to CDSSs [Yin and Jha, 2017]. HDSS has a multi-tier structure,starting with a WMS tier, backed by robust machine learning, thatenables diseases to be tracked individually by a disease diagnosis module.It sequentially structures the information framework for daily healthmonitoring, initial clinical checkup, detailed clinical examination, andpost-diagnostic decision support.HDSS has two major parts to support daily and clinical healthcare:
16Emerging Smart Healthcare Systems(i) Pervasive Decision Support System (PHDS), shown on the left ofFig. 3.1 and (ii) PHDS-assisted CDSS (CDSS ), shown on the right ofFig. 3.1. PHDS acts on WMS data for daily disease diagnosis. CDSS tackles clinical diagnosis. HDSS has four major tiers. Tier-1 assists withdaily health monitoring. The decision modules in Tier-1 are trainedusing clinical domain knowledge. This transmits physician expertiseacross the clinical boundary, and can thus help individuals withoutprofessional medical training to effectively track their diseases. Whenan alert is raised at Tier-1, it passes symptom records, stored as diseaseonset records, across the clinical boundary. Tier-2 provides immediatedecision support to physicians for an incoming patient based on basicclinical measurements. Tier-3 entails a more detailed diagnostic analysisbased on detailed laboratory measurements. Finally, Tier-4 providespost-diagnostic treatment, prescription, and lifestyle suggestions. Higherlevel tiers gather more information than lower-level ones, but at highertime and energy costs. HDSS operates across these tiers in a sequentialand closed-loop manner, as indicated by the large arrow behind thefour tiers in Fig. 3.1.HDSS deploys various Transitions (T ) to facilitate the flow of information among the various tiers, as depicted by indexed arrows in Fig. 3.1.When an alert is raised at Tier-1, a transition TIN passes disease-onsetrecords across the clinical boundary. At Tier-2, HDSS aggregates thedata with additional physician insights, and then passes the data tothe diagnosis engine through T1 . The diagnosis engine contains librariesaccessible by machine learning engines, such as WEKA [Hall et al.,2009] and TensorFlow [Abadi et al., 2016]. If a diagnosis requires furtherlaboratory measurements, T2 transfers HDSS to Tier-3. Otherwise, T20transfers HDSS to Tier-4. In either case, diagnostic suggestions areimmediately available to physicians. When T2 occurs, Tier-3 reaches thediagnosis engine through T3 . The engine orders appropriate laboratorytests via T4 , after which test results are fed back to the diagnosis enginevia T5 . Diagnosis at Tier-3 consumes more time and expense comparedto Tier-2. For example, it can take 12-16 hours to acquire a blood testreport (even longer for te
ical healthcare systems, the fundamental challenges associated with . In this chapter, we present a novel smart healthcare framework that captures the rapid clinical-to-daily healthcare expansion. This framework defines the scope of smart healthcare, thus helps unify