Transcription
Winton Woods City Welcometo the WintonWoodsCity SchoolDistric!.ThefollowingInformationis providedto maketheenrollmentprocessas easyas possiblefor youandyourchild!Pleasereadover required documentscarefully.Incomplete enrollments mav not be accepted. .PROOF OF RESIDENCYConfirm the residence reported is within the district. See reverse side for proof of residency requirements.BIRTH CERTIFICATEVerify date of birth by a certified "original" birth certificate and copy the birth certificate for school records. A passport/ or court orderdesignating parentage and date of birth may also be used as an alternative to the birth certificate. A child whose 5th birthday falls on orbefore August 1st is eligible to enter Kindergarten, and one whose 6th birthday falls on or before August 1st and who has successfullycompleted an accredited kindergarten, Montessori program, or equivalency is eligible to enter 1st grade for that year, provided all otherrequirements are met. Rv. 11/2012-PROOF OF CUSTODY - only the parents/legal guardian can enroll a childVerify child custody by the birth certificate or certified copies of any child custody orders or decrees. Child custody orders or decrees must befiled with the court and signed by a judge or magistrate. Notarized agreements not filed with the court and signed by a judge ormagistrates are not acceptable. Ohio law requires the parent/custodian provide the school with the most recent copy of any court actionregarding custody.PROOF OF STUDENT IN GOOD STANDINGWe ask parents and students to verify their disciplinary status with their previous school by answering the question on the enrollment form.Students are not permitted to enroll in another school system if they are under any expulsion or pending expulsion.PROOF OF IMMUNIZATIONGrades Pre-School thru 12th must show proof of current & completed immunizations at the time of enrollment. Rv. 10/2012VERIFICATIONOF INDIVIDUAL ENROLLING CHILDVerify identity of the individual enrolling the child (driver license preferred or other photo ID) to confirm that it is the person with custody andempowered to make educational decisions on the child's behalf.SCHOOL RECORDSElementary -IeUer or current grade report from previous schoolto verify grade level must be provided.Middle School- to create a student's class schedule and verify grade level the most recent grade report or schedule must be provided.High school- to create a student's class schedule, the most recent transcript (unofficial copy may be used) must be provided.IEP/MFE placement decisions are made based on the review of the current lEP and MFE.All required documents must be presented at the time of enrollment. Incomplete enrollments mav not be accepted.*Due to state laws and/or board policy, Winton Woods requires the above documents to be shown to school officials when your child (ren) isbeing registered. Thank you in advance for providing these documents.Office hours for registration are: Mon-Fri 8:00am - 3:00pm Phone (513) 619-2360 Fax (513) 619-2363OS/2013
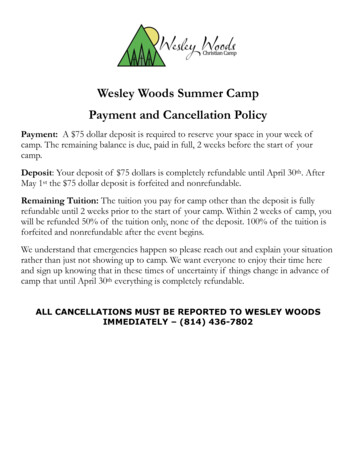
WINTONWOODS QTYSŒIOOLDISTRICfproceduresforPROOF OF RESIDENCYBefore any student is enrolled in the Winton Woods City School District the student's parent or legalguardian* must prove legal residence in the District.Families whose primary residence is outside of the School District must apply for Open Enrollment duringthat time frame, to be eligible to attend Wmton Woods Gty Schools.All applicantsmust submit no less than three proofs of residency. One must be from Column A.Documents must he pre-printed with .the name .and address. of the student's parent or guardian* and must bepresented at the Enrollment Center at the time of registration.These documents will also be required for any change of address.All applicants must submit at least one documentfrom Column A plus two documents from either Column B or C:ColumnAColumnBColumnCA utility bill or work order datedwithin the past 60 days,including:·Copyof deed, mortgage paymentreceipt or contract for newconstruction Energy bill·Valid driver's license·Current vehicle registration Valid Ohio photoidentification card Valid passport·Lease or rental agreement-signedby owner/manager (must listnames of all occupants) Home telephone billDated within the past year:·W-2 fonn·Propertytax bill Affidavit signed by home owneror resident with whom parents areresidingPlease call first to assure thatnotary is in.Forest Park Tax Office-1201W.Kemper Road 595-5211 (closedTuesday and ThursdaY,)Greenhills Tax Office-11100Wmton Road 825-2100Sl1ringfield Township - residentsmay call the Enrollment Center619-2360·Section 8 agreement-signed copy·Cable billDated within the past 60 days: Letter from approvedgovernment agencyo Payroll stubo Bank or credit card statement* Legalguardianship·Waterbillrequires additional documentation from a court or agency.Office hours for registration are: Mon-Fri 8:00am - 3:00pm Phone (513) 619-2360 Fax (513) 619-23630512013
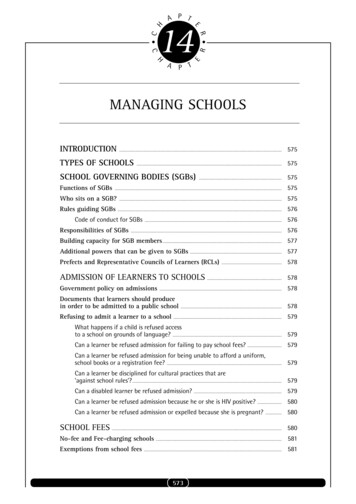
General Fact Sheet*Buildings may have policies or procedures specific to their environment.1M1M1M1M1M1MIMSchool Hours -NO SUPERVISION for students before school'hours.9:30 am until 12:00 am OR 1:25 pm until 3:55 pmo Pre-School9:10 am until 4:10 pmo Kindergarten -28:35 am until 3:35 pmo Grades 3-48:00 am until 3:00 pmo Grades 5-67:30 am until 2:30 pmo Middle School8:00 am until 3:07 pmo High SchoolAbsences - Please contact Office before school. Please send a note upon your student's return to school.School Fees - General fees for the school year are as follows:Kindergarten: 301·2: 403·6: 507·8: 709·12: 70 base fee- total high school fees will vary due to individual course costs, seefee schedule. Fees are payable by cash, check, or money order made out toWWCS. Students are not able to participate in extracurricular activitiesincluding field trips until the fees are paid. Fees are assessed in order to coverthe cost of consumable materials used in various courses.Tardy -:-If a student is not in class at the time school begins he/she must come to the Office upon arrival and signin. Please call and send a note when your student is tardy.Lunch Prices - prices are subject to changeo Primary, Elementary, and Intermediate 2.20 for a full lunch; .50 for milko Middle School and High School 2.70Prices vary for snacks. Applications for Free/Reduced Lunches are sent home with each student at thebeginning of the year and must be renewed each year.District Calendars - available at the beginning of the school year in the school offices.Medicationso Students are not permitted to have ANY TYPE OF MEDICATION on their person. The only exception to thisis with certain emergency medication by written order of the doctor and prior approval of the district nurse.o School employees cannot dispense any medication unless we have the proper forms signed by a parent andfor prescription medications by the parent and the student's doctor.o ALL MEDICATIONS (and proper forms) must be brought to school by an adult.OOffice hours for registration are: Mon-Fri 8:00am - 3:00pm Phone (513) 619-2360 Fax (513) 619-236305/2013
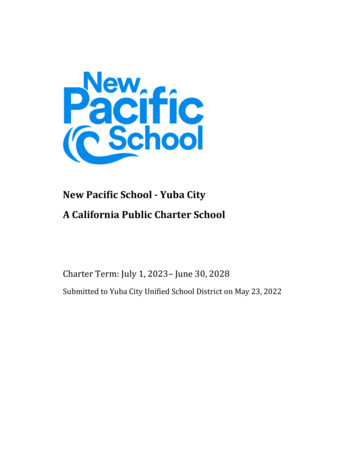
111111111111 111111111111111111FOR SCHOOL DISTRICT PERSONNEL ONLYSchool Year 20 '/20Entry DateEntry CodeRecords Requested j jHome Rm/TchrHome SchoolGradeAssessment Date.JInt.Section 1Please Circle One: Student is aStudent's1. US Citizen3. Foreign Exchange Student2. Non-US Citizen/ImmigrantInformationLast Name (as it appears on Birth Certificate)Birthday (mm1dd 1VY)First NameBirth city and countryNative LanguageCircle Gender:Called NameMiddleContact NumbersHome-' 1 ' IMale or FemaleMother's Maiden NameCel/-Student's S.S#Work---- Home AddressPrevious School DistrictZipStateCityCityName of SchoolDate Last AttendedState ----------------------Is there joint custody of this student?YFatherOtherYWINTONNWOODSSCHOOL DISTRICT REGISTRATIONStepmotherStepfatherGuardianNAre there custody documents filed with the courts?YearStudent lives with? Circle all that applyWho has legal custody? Circle all that applyMother/FORM1
FAMIL V INFORMATIONSection teHome PhoneCellLegal CustodyY NSpeaks English Y eHome PhoneCellY NZipWorkEmailReceives MailingsEmailReceives MailingsY NZipWorkParent/GuardianLegal CustodyY NSpeaks English Y Nlanguage SpokenSection 3Is the Student an IMMIGRANT YOUTH: Circle one YN (An immigrant youth is a child that meets all three of the following)1. Child is between ages 3 - 212. Child was not born in the U.S.3. Child has not attended one or more schools in anyone or more of the states for more than 3 academic years.list any other Ohio school district enrolledJ'-'Section 4SPECIALEDUCATIONSERVICES(if currentlv receiving special education services please check this box).If yes Circle All that apply:lEPETRMFE504Circle all that applv: I have provided a current copylEP MFE S04 I have not provided a current copyList all Disabilities:Section 5Is this student currently under a suspension or expulsion from another school district? Circle Y orHas student: been in Winton Woods before? YIf Yes, Year attendedJEP MFE 504NNAttended vocational school Y N ProgramWINTONWOODSSCHOOL DISTRICT REGISTRATIONrr:FORM2
Section 6HOME LANGUAGE SURVEYWhat language did your child speak when he/she first learned to talk?What language does your childuse most often at home?-'-What language do you use most often with your child?What language do the adults most often speak at home?How long has your child attended school in the u.S?I·,When did your child first enter a school in the U.S.?Section 7FOR COURT APPOINTED GUARDIANSGuardian's NameONLY, PLEASE COMPLETE THE FOLLOWING INFORMATION:Name of agency(From birth certificate) Name of birth parentsContact #--'School District of ResidencyAddress of birth parentsName of Surrogate ParentContact #Section 8Copy of training on file? Y N RequestedPlease Read and Initial eachI have received a copy of Winton Woods City Schools Dress Code Guidelines:I understand that Incomplete Immunization Records will disrupt my child's start date/attendanceAnd if entering the country my child (ren) must be tested for TB or in the process to be tested before starting schoolSection 9SIBLlNG(S)ATTENDING WINTON WOODS lSection 10PLEASEPRINT NAMESIGNATUREOF LEGALGUARDIANRELATIONSHIPOFFICEUSEONLY:Birth Cert.ImmzIDCust DocGr.verifiedOther PORSp. EdESLDress code Inti.InternetLunchWINTONlEPCont./LeaseEmer CardRec. ReqIRN #WOODS SCHOOL DISTRICT REGISTRATIONUtility ----'Health Ree.Enr. By:FORM3Expulsion'¡Ent. By:DATE
111111111111111111111111111111EMERGENCY MEDICALAUTHORIZATION FORMTeacherGradeSchoolPURPOSE OF THIS FORM: To enable parents and guardians to authorize the provision of emergency treatment for children who become ill or injured whileunder the school's authority, when parents or guardians cannot be reached. Please be sure to complete each blank.Student LAST NAMEStudentrmsrNAMEStudent Home AddressSex (MlF)CityHome Phone NumberDate of BirthZip CodeStateSiblings in District: First and Last 's NameMother's AddressMother's Home Ph. #Mother's Wk. Ph. #Father's NameMother's Cell Ph. #Father's AddressFather's Home Ph. #Father's Wk. Ph. #Step Parent's NameFather's Cell Ph. #Step Parent's AddressStep Parent's Home Ph. #Step Parent's Wk. Ph. #Step Parent's Cell Ph. #NAMES OF RELATIVE / CARE PROVIDER / ALTERNATE CONTACT (WHO TO CONTACT IN THE ABSENCE OF PARENT! ddressDaytime Phone #RelationshipIf there are any medical conditions, please check this boxNote: Details regarding noted medical conditions should be noted below* * * * * PARTDI OR PART II BELOW MUST BE COMPLETED AND SIGNED* ****PART I - TO GRANT CONSENT. I hereby give consent for the following medical care providers / local hospital to be called.Doctor's NamePhone#AddressDentist's NamePhone#AddressMedical Specialist (optional)Phone#AddressLocal HospitalER Phone #AddressInthe event reasonable attempts to contact me have been unsuccessful, I hereby give my consent for (l) the administration f any treatment deemed necessary byabove named doctor, or in the event the desiguated preferred practitioner is not available, by another licensed physician or dentist, and (2) the transfer of the childto preferred hospital or any hospital reasonably accessible. This authorization does not cover major surgery unless the medical opinions of two other licensedphysicians or dentists, concurring in the necessity for such surgery, are obtained prior to the performance of such surgery.Facts concerning the child's medical history including medical conditions (ex. Diabetes, asthma, significant allergies, ADHD, autism, Down Syndrome,hearing/vision impairments, etc.) and medications being taken to which a physician should be alerted:DateSignature of Parent! Guardian --;:::;-:--:--;---;--:---:-: -. :-:-;-:- -;-:-:--:--:--:- -;-NOTE: The above information will be shared with appropriate staff as necessary. This includes, but is not limited to, administrators.drivers.foodservice staff, custodians, coaches and substitute employees. Please notify the school nurse of any concerns.-:- ;;;-;-teachers, support steff, busDO NOT COMPLETE PART II IF YOU COMPLETED PART IPART II - REFUSAL TO CONSENT. I DO NOT give my consent for emergency medical treatment of my child. Inthe event of illness or injury requiringemergency treatment, I wish school/district authorities to take the following action:DateSignature of Parent! Guardian
111111111111111111111111111111Race/Ethnicity ReportingDue to mandated data collection and reporting requirements from the United States Department of Education (USDOE),the Ohio Department of Education is changing the reporting of race/ethnicity information.Please complete the boxes below in regards to your child's race/ethnicity. If you fail to complete the informationbelow, the District will use observer identification to complete this form.BOXlStudent Name:Last NameMiddle NameFirst NameBOX2Is your child of Hispanic/latinoHeritage?DNoOVes(Continue below)Persons of Mexican. Puerto Rican, Cuban, Central or South American, or other Spanish culture or origin regardless of race.BOX3Is your child multiracial?OVesDNo(Continue below)Persons having origins in two or more of the racial! ethnic groups list below in Box4BOX4BOX5Select more than one of the following if youchecked "Yes" in Box 3 above:D WhitePersons who have origins in any of the original peoples ofEurope, North Africa, or the Middle East.D Black or African AmericanPersons who have origins in any ofthe black racial groupsIn AfricaD AsianPersons having origins in any ofthe original people of theFar East, Southeast Asia, or the India subcontinent, Thisarea includes, for example: Cambodia, China, India, Japan,Korea, Malaysia, Pakistan, the Philippine Islands, Thailand,and VietnamD American Indian or Alaskan NativeSelect one of the following if you checked"No" in Box 3 above:D WhitePersons who have origins in any of the original peoples ofEurope, North Africa, Dr the Middle East.D Black or African AmericanPersons who have origins in any of the black racial groupsin AfricaD AsianPersons having origins in any of the original people of theFar East, Southeast Asia, Dr the India subcontinent, Thisarea includes, for example: Cambodia, China, India, Japan,Korea, Malaysia, Pakistan, the Philippine Islands, Thailand,and VietnamD American Indian or Alaskan NativePersons having origins in any of the original people ofNorth and South America (including Central America) andwho maintain tribal affiliation or community attachmentPersons having origins in any of the original people ofNorth and South America (including Central America) andwho maintain tribal affiliation or community attachmentD Native Hawaiian or Other Pacific IslanderD Native Hawaiian or Other Pacific IslanderPersons having origins in any of the original peoples ofHawaii, Guam, Samoa, or other Pacific Islands.Parent IGuardian Signature,Persons having origins in any of the original peoples ofHawaii, Guam, Samoa, or other Pacific Islands.Oate:,
111111111111WINTON WOODS CITY SCHOOLSAUTHORIZATION TO RELEASE INFORMATIONEnrolling to enter grade:Parent/GuardianDate of BirthM.I.First Name(print) Student's Last Name(print) Parent/GuardianName:DateSignature authorizing the release of school records to Winton Woods City SchoolsPrint contact namePhoneFaxAddressCityStatePrevious SchooI/Institution NamePhoneFaxAddressCityStatePresent School/InstítuûonNameAttn: Registrar/RecordsZip CodePrint contact nameZip CodeClerkIs student currently under an expulsion or suspension?YESNOIf records are not available, please return our request indicating the reason:( ) No records available() Sending partial recordsReason(s):Students' withdraw date:.!/!/Records Clerk Signature: Discipline Records - Suspensions/ExpulsionsTranscript of subjects and gradesAttendance RecordOhio Proficiency / Standardized Test ResultsHealth RecordsDate: Court Orders (Custody, Restraining, etc)All Other personally identifiable dataPsychological or Other Individual Test Results*lEP & Special Education Records, if applies"504 or other Intervention Plans*Fax or Email records to: (Johnson.Kim@wintonwoods.org)( ) Primary North 73 Junefield Avenue, Cincinnati, Ohio 45218 Phone 513.619.2390 Fax 513.619.2398( ) Primary South 825 Lakeridge Drive, Cincinnati, Ohio 45231 Phone 513.619.2470 Fax 513.619.2479( ) Elementary School 1501 Kingsbury Drive, Cincinnati, Ohio 45240 Phone 513.619.2490 Fax 513.619.2497( ) Intermediate School825 Waycross Road, Cincinnati, Ohio 45240 Phone 513.619.2450 Fax 513.619.2451( ) Middle School147 Farragut Road, Cincinnati, Ohio, 45218 Phone 513.619.2440 Fax 513.619.2452( ) High School 1231 West Kemper Road, Cincinnati, Ohio 45240 Phone 513.619.2420 Counselor Fax 513.619.2415( ) Student Services 8 Enfield Street, Cincinnati, Ohio 45218, Phone 513.619.2320 Fax 513.619.2339( ) Enrollment Center 8 Enfield Street, Cincinnati, Ohio 45218, Phone 513.619.2360 Fax 513.619.2363Please send the above records, if available for this student, as soon as possible. Pursuant to Section 5 Paragraph C of 325 ILCS 5015"any elementary or secondary school requested to forwarded a copy of a transferring student's record to the new school shall complywithin 10 days of receipt unless the record has been flagged pursuant to subsection (a) notification by Dept. of a person'sdisappearance). "WWCS RegistrarDateAdmission Date
FROM THE NURSE'S OFFICEEmergency CardsPlease complete both sides ofthe emergency card (remember to sign the appropriate section for consent on theback of the card). Give names and numbers of those adults preferably in the Winton Woods area who are ableto help your child in case of emergency or illness. Student will only be released to those listed on theemergency card.Medication ProcedureNo student will be given medication at school unless the proper forms have been completed and themedication has been delivered to the school by an adult. A medicationform must be completedby the.physician and parent for each prescription medication and a.form must be completed bythe parent for each over. the counter medication. Use one fonn for each medication. Medications can only be given as directed on thefonn. A physician/parent authorization must be on file in the office before a student can carry and selfadminister an inhaler or Epi-pen.Health Exclusion PolicyThe following categories of students will be excluded from school until the situation has been remedied: A student who has not been fully immunized per state health guidelines. A student with symptoms of a communicable disease. A student with head lice and/or nits. A student with a communicable rash. A student with a temperature of 100 degrees or greater. A student must be fever free without feverreducing medication for 24 hours before returning to school.Head LiceThe Winton Woods City School District has a "no nits" policy, as do most schools in the area. This means thatallHce and nits must be removed from a child's hair before returning to school. Each school has writteninformation detailing how to become free of head lice and nits. If your child has lice or nits, please inform theschool so the rest of his/her class can be checked. We try to maintain confidentiality and try to be sensitive tothe child's need.Screening ProceduresThe State of Ohio has mandated that vision, hearing, and scoliosis screenings be perfonned at certain gradelevels. If you have questions about this, feel free to contact the nurse.Please call with any questions or health 9-2320Winton Woods District Nursesrevised 9/12
Dear Parents of Students New to the Winton Woods City School District:The Ohio State Department of Health and the Winton Woods City School District Boardof Education require certain immunizations upon entrance to school. The following recordsmust be completed in order for students to fulfill registration requirements:Proof of Immunizations1.DPT (Diptheria, Pertussis, Tetanus) At least four doses are required, If the 4th. dose wasgiven beforethe. th·birthday, a5th dose is required.ORTD (Tetanus, Diptheria) At least 3 doses are required if immunization process isstarted after age six.Tdap or TD Booster (Tetanus, Diptheria, Pertussis) required for grades 7-11If the 3rd dose was given before the 4th2.POLIO At least 3 doses are required.birthday, a 4th dose is required.3.MMR (Measles, Mumps, Rubella) 2 doses are required4.HEPATITIS B 3 doses are required5.Varicella6.Hib (haemophilus-b)7.PPD (Tuberculosiscountry.(chicken pox) 1 dose required for grades 5-8Second dose required for grades K- 4required for pre-school (see guidelines)skin test) required for students entering from a foreignHealth is a very important part of a child's achievement and well-being. It is important foryou to share with us any information about your child's health that requires the cooperationbetween family and school.Sincerely,Patricia D' Arcy, DirectorDepartment of Teaching and Learningpp-88-303bRevised 1/14
111111 II 1111PARENT NOTIFICATION OF HEALTH REQUIREMENTSDATE:STUDENT'SGrade: (student is now entering)NAME:DATEOFBIRm:NAME OF PREVIOUS SCHOOL:CITY/STATE:Gender: M or F:PARENTCONTACTNUMBER:-------- --'PHONENUMBER:Facts concerning this student's medical history (ex: Diabetes, Asthma, Allergies (food,environment, & medicine), physical impairment, conditions requiring medications, etc.)*For severe conditions please contact your School Nurse prior to student starting school.Has this student ever had a positive TB (tuberculosis) skin test?Was a chest x-ray done?Date:Has this student BEEN IN a foreign country in the last 5 years? YESNameofCountryReason for visit:NOLength ofvisit:Returned to United States from visit (Month/Y ear):Has this child ever attended a Winton Woods City School before? Yes or NoIf YES, name of last school attended:Current immunization records MUST BE PROVIDEDin order to complete the enrollment process.I have been informed of the items needed to complete registration for school for my son/daughter.Parent SignatureRevised 9/12
111111111111 11111111111111 IIIIWINTON WOODS CITY SCHOOLSMEDICINE RELEASE FORMAll medications must accompany this form, must be in the original container,and must be delivered to the school by an adult.*THIS SECTION TO BE COMPLETED BY PARENT OR LEGAL GUARDIAN*Use separate form for each medicationStudent's Teacher:Dosage:,Time to be given during school hours(i.e. lunchtime, 12:00p.m. etc.)Description of Medication: Possible side effects:-----------In signing this fonn, I will assume responsibility for safe delivery of the medication to the school, I will beresponsible for providing written notification by myself and my physician of any change in the use of themedication or the prescribed treatment, and I release and agree to hold the Board of Education, its employeesand its officials harmless from any and all liability foreseen or unforeseen for damages or injury resultingdirectly or indirectly from this authorization.Parent/Guardian Signature:Home Phone:Date:Emergency Phone:*TIDS SECTION TO BE COMPLETED BY PHYSICIAN FOR PRESCIPTION MEDICATIONS*Use separate form for each medicationStudent's Name:Medication:Dosage:Time to be given during school hours:(i.e. Lunchtime, 12:00 p.m. etc.)Description of Medication:Possible side effects:Special instructions:---'-Physician's Name: (print)Phone:Physician's Signature:Date:Date of initiation of medication:-------------Date to discontinue: -------This permission is valid only for the current school year.All medication must be picked up from the school by an adult by the last day of school or it will be discarded.A student may carry and/or administer his/her own medication if so ordered,in writing, by both the physician and parent.pp-88-303cRV2/07
111111111111STUDENT NETWORKAND INTERNET ACCEPTABLE USE AND SAFETY AGREEMENTPlease complete the following information:Student User's Full Name (please print):Homeroom/Advisory:.Student ID:School:Grade:Parent/Guardian's Name (please print):--'- Please see back side for parent/student signaturesTo access e-mail and lor the Internet at school, students under the age of eighteen (18) must obtain parent permission and mustsign and return this form. Students eighteen (18) and over may sign their own forms.Use of the Internet is a privilege, not a right. The Governing Board's Internet connection is provided for educational purposes only.Unauthorized and inappropriate use will result in a cancellation of this privilege.The Board has implemented technology protection measures, which protect against (e.g. block/filter) Internet accessto visualdisplays/depictions/materialsthat are obscene, constitute child pornography, or are harmful to minors. The Board also monitorsonline activity of students in an effort to restrict access to child pornography and other material that is obscene, objectionable,inappropriate and lor harmful to minors. Nevertheless, parents/guardians are advised that determined users may be able to gainaccess to information, communication, and/or services on the Internet that the Board has not authorized for educational purposesand/or that they and/or their parents/guardians may find inappropriate, offensive, objectionable or controversial.Parents/Guardians assume this risk by consenting to allow their students to participate in the use of the Internet. Students accessingthe Internet through the school's computers assume personal responsibility and liability, both civil and criminal, for unauthorized orinappropriate use of the Internet.The Board has the right, at any time, to access, monitor, review and inspect any directories, files and/or messagesresiding on or sentusing the Board's computers/networks.Messages relating to or in support of illegal activities will be reported to the appropriateauthorities.As the parent/guardian of this student, I have read the Student Network and Internet Acceptable Use and Safety Policy andGuidelines, and have discussed them with my child. I understand that student accessto the Internet is designed for educationalpurposes and that the Board has taken available precautions to restrict and lor control student accessto material on the Internetthat is obscene, objectionable, inappropriate and/or harmful to minors. However, I recognize that it is impossible for the Board torestrict access to all objectionable and lor controversial materials that may be found on the Internet. I will not hold the Board (orany of its employees, administrators or officers) responsible for materials my child may acquire or come in contact with while on theInternet. Additionally, I accept responsibility for communicating to my child guidance concerning his/her acceptable use of theInternet -i.e., setting and conveying standards for my daughter/son to follow when selecting, sharing and exploring information andresources on the Internet. I further understand that individuals and families may be liable for violations.7540.03 Fl/page 1 of 2NEDLA 2009
Parent/GuardiansTo the extent that proprietary rights in the design of a website hosted on the Board's servers would vest in my child upon creation, I.agree to assign those rights to the Board.Please check each that applies: , ;I give permission for my child to use and accessthe Internet at school and for the Board to issue an Internet/e-mail accountto my child.I give permission for my child's image (photograph) to be published online, provided only his/her first name is used.I give permission for the Board to transmit "live" images of my child (as part of a group) over the Internet via a web cam.I authorize and license the Board to post my child's classwork on the Internet without infringing upon any copyright mychild may own with respect to such class work. , understand only my child's first name will accompany such classwork.Parent/Guardian's Signature:Date:StudentI have read and agree to abide by the Student Network and Internet Acceptable Use and Safety Policy and Guidelines. I understandthat any violation of the terms and conditions set forth in the Policy and Guidelines is inappropriate and may constitute a criminaloffense. As a user of the Board's computers/networkand the Internet, I agree to communicate over the Internet and theNetworking in an appropriate manner, honoring all relevant laws, restrictions and guidelines.Student's Signature:Date:-,-Teachers and building principals are responsible for determining what is unauthorized or inappropriate use. The principal may deny,revoke or suspend access to the Network/Internet to individuals wh
*Duetostate laws and/or board policy, Winton Woodsrequires the above documents tobeshown toschool officials whenyour child(ren)is being registered. Thankyouinadvance forproviding thesedocuments. Office hours forregistration are: Mon-Fri 8:00am - 3:00pm Phone (513) 619-2360 Fax(513) 619-2363 OS/2013