Transcription
VIRTUAL MEDICAL CENTERFROM OPERATIONAL TO GARRISONLTC(P) Sean J. Hipp – DirectorMr. Jeffery Burgwin – Deputy DirectorMAJ Daniel Yourk – Deputy Director for Operations“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDSlide 1As of: 18 November 2019
DisclosurePresenter’s have no relevant financial or non-financial interests to disclose.Disclosure will be made when a product is discussed for an unapproved use.This continuing education activity is managed and accredited by AffinityCE incollaboration with AMSUS. AffinityCE and AMSUS staff as well as Planners andReviewers, have no relevant financial or non-financial interests to disclose.Commercial Support was not received for this activity“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDSlide 2As of: 18 November 2019
PURPOSE, OUTLINE AND DISCLOSUREPurpose: To have a better understanding of the Virtual Medical Center and how it can be a force multiplier in thedelivery of military medicine from operational to garrison.Outline:1.The Problem/ Multi-Domain Operations2.Benefits of Virtual Health3.Strategic Overview4.Creating Solutions5.Operational Programs6.Virtually Integrated Patient Readiness & Remote (VIPRR) Clinic7.Tele Behavioral Health Integration with the Enterprise8.VMC Cooperative Initiatives9.Administrative Initiatives10.SummaryDisclosure: The view(s) expressed herein are those of the author(s) and do not reflect the official policy or position of BrookeArmy Medical Center, the U.S. Army Medical Department, the U.S. Army Office of the Surgeon General, the Department of theArmy, the Department of the Air Force and Department of Defense or the U.S. Government."“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDSlide 3As of: 18 November 2019
MULTI-DOMAIN OPERATIONS“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDRef: COL Jeremy Pamplin – Director TATRCSlide 4As of: 18 November 2019
TYRANNY OF DISTANCE“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDRef: COL Jeremy Pamplin – Director TATRCSlide 5As of: 18 November 2019
BENEFITS OF VIRTUAL HEALTH VH is a is a force multiplier in Operational AO’s to preserve combatpower Improves the readiness of our medical force Projects medical capabilities to the point of need Improves patient & peer-to-peer access to specialty providersregardless of geographic location Mitigates travel risks and demandsCommanders must fight and win in acomplex environment. They do thisthrough maintaining lethality andpreserving combat power forward. Wemust leverage medical technology toenable treatment and managingSoldier care far-forward, in thefoxhole, whether through enhancingmedical capabilities of the Medic orconsultation to specialty providersfrom the point of need.“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDSlide 6As of: 18 November 2019
STRATEGIC OVERVIEW Service VH efforts now fall under a single MHS VH Strategy aligned to asingle MHD VH POM which the DHA will manage effective Oct 19.Virtual Medical Center InitiativesGoal 1: Develop VH support for the WarfighterGoal 2: Support the MHS Clinical CommunitiesGoal 3: Use VH to Improve Access to Quality Care forMHS BeneficiariesGoal 4: Manage Costs Through and Within VH1234Centralized VH PrivilegingXXXXVirtual Health Care Coordination ApplicationXXXXMobile Medic for the EnterpriseADVISORRemote Health MonitoringAMEDDC&S SynchronizationCoding Auditing and EducationIntegration with BH ResourcesTele-Critical Care NetworkPATH/HELP IntegrationCoordination of EHR access at MTFsEducation of Providers and StaffCart Education and TrainingSynchronization with MHSXXXXXXXXSynchronization with Joint Surgeons OfficeX“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDXXXXSlide 7XXXXXXXXXXXXXXXXXAs of: 18 November 2019
MHS Virtual Medical Center Construct OCT19“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDSlide 9As of: 18 November 2019
CREATING SOLUTIONSHow do we make sure that there is a Ready Medical Force for Multi-Domain Operations?VMC synchronizes medicalservices across theenterprise supportingoperational and garrisonforces anytime, anywhere 18 time zones 30 countries and territories Over 30 clinical specialties“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDSlide 10As of: 18 November 2019
MOBILE MEDIC – TRAIN AS YOU FIGHTGarrisonOperational Mobile Medic teamconsists of a group ofthe Army’s CombatHealth Specialists (68W)dedicated to providingmobile Virtual Healthsupport at the point ofneedField TrainingBenefits Improve access to care Reduced time Service Members are away from training Increased 68W primary care skills Capability to bridge time/distance factors Medical force multiplier for prolonged field care situations“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDSlide 11As of: 18 November 2019
To provide a full spectrum of on-demand consultationservices to operational forces for contingency support.Call: 833-ADVSRLN(833-238-7756)#1 Critical Care#2 SpecialtyServices#3 EmergencyDepartment#4 USAISRBurn Center#5 VeterinaryMWD#6 TrainingOption#7 ChemicalCasualtyTo coordinate training with ADVISOR email DoD.advissor training@mail.mil“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDSlide 12As of: 18 November 2019
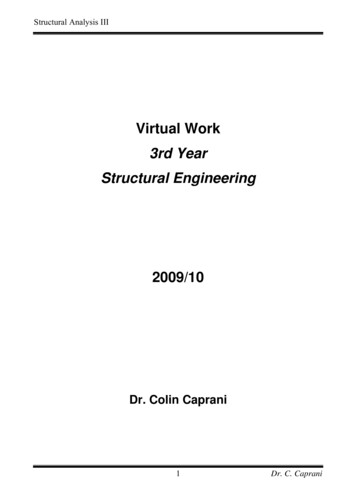
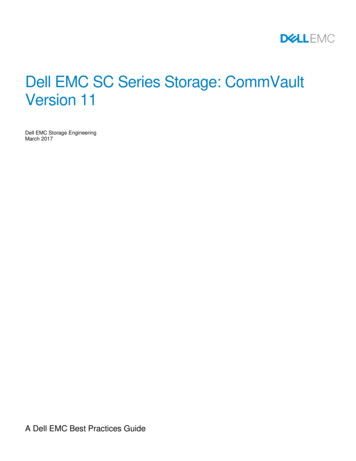
REAL-WORLD EXAMPLESDate10 JUL 1712 NOV 1729 APR 1830 MAY 1825 SEPT 17Service ConsultedInfectious DiseaseGeneral SurgeryToxicologyInfectious DiseaseInfectious DiseaseOriginating Site ofCallDisposition ofCallOperational ImpactPotential CostAvoidanceAVOIDED EVACPatient remained in country and was managed by local providerrather than evacuating the patient to LRMC, Germany 115,000AVOIDED EVACConsult resulted in the development of a treatment plan thatallowed the originating site provider to manage the patient locally 115,000AVOIDED EVACConsult resulted in the development of a treatment plan thatallowed the originating site provider to manage the patient locally 42,000OB Felty, AfghanistanAVOIDED EVACConsult resulted in the development of a treatment plan thatallowed the originating site provider to manage the patient locally 70,000CameroonDowngradedUrgency of EvacDowngraded the evacuation priority from Urgent to Routine:Prevented Urgent Evacuation 80,000 (EstimatedDowngraded the evacuation priority from Urgent to Routine:Prevented Emergent Evacuation 80,000 (EstimatedWest AfricaAfrica (Specific location unknown)Al Udeid, QatarDifference)06 FEB 17Critical CareCameroonDowngradedUrgency of Evac23 JUN 19Orthopedic SurgeryAfricaAVOIDED EVACConsult resulted in the development of a treatment plan thatallowed the originating site provider to manage the patient locally 115,00002 JUL 19Veterinary ServicesEgyptDowngradedUrgency of EvacDowngraded the evacuation priority from Urgent to Routine:Prevented Emergent Evacuation 80,000 (Estimated27 OCT 19Infectious DiseaseNigerAVOIDED EVAC- Severe Plasmodium falciparum malaria – ADVISOR providerprovided recommended treatment plan and avoided EVAC. 115,000Potential Aircraft Cost Avoidance:(Referencesfor cost avoidance analysis listed in notes section of this slide)LTC(P) Sean J. Hipp,MD/sean.j.hipp.mil@mail.mil/1-844-V-MEDCEN 812KDifference)Difference)*Analysis does not include cost associated with EVAC Personnel/medical attendants, the Risk of anUrgent evacuation or the degradationof operational capabilityUNCLASSIFIEDSlide 13Astoof:the18unit*November 2019
“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDSlide 14As of: 18 November 2019
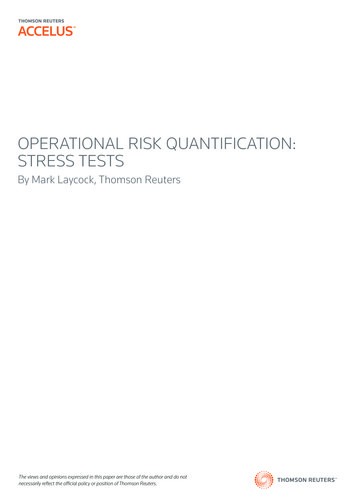
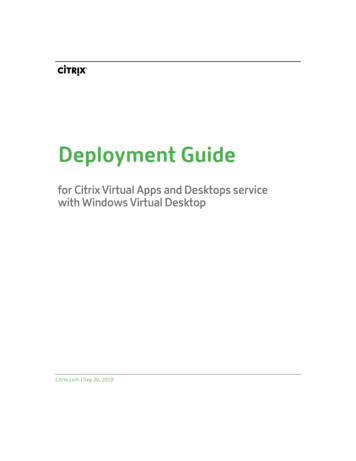
VIPRR Clinic Metrics (FEB – OCT 2019)FEB - OCT 2019 Monthly VIPRR Clinic Encounters by Service120012091000902# of VIPRR Clinic Encounters2912001062800FEB - OCT 20191400412100081113 yMAYAir ForceJUNMarinesJULNavyAUGNot ListedSEPCoast GuardOCTGrand Total04961Highlights:ArmyAir ForceMarines The VIPRR Clinic completed 5,174 virtual medical readiness appointments from FEB – OCT 2019NavyNot ListedCoast Guard VIPRR Clinic no-show rate 2.84% Overall Patient Satisfaction with Provider (JOES) 94.5% VIPRR Clinic providers have provided medical readiness support to Service Members Assigned to 948 different Unit Identification Codes (UICs)and enrolled to 62 different MTFs (Parent DMIS ID) across the world.“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDSlide 15As of: 18 November 2019
Global Support!“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDSlide 16As of: 18 November 2019
CONUS Support“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDSlide 17As of: 18 November 2019
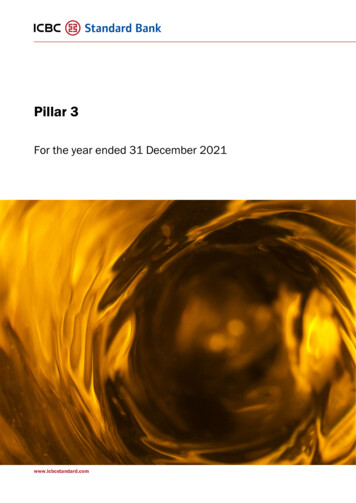
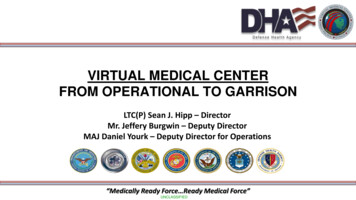
VIRTUAL BEHAVIORAL HEALTH CONSTRUCT There are 3 Army Behavioral Health hubs that areregionally aligned Regional Health Command Atlantic, Augusta, GeorgiaRegional Health Command Central, San Antonio, TexasRegional Health Command Pacific, Honolulu, Hawaii3 hubs will fall under the VMC construct Oct 19Gaps/Barriers Need a leader to track and coordinate capacity acrossthe enterpriseConnect to the operational space and report toleadership in theaterEnterprise education about services offered at the TBHhubsNeed to incorporate into VHCAANeed to track schedule with TELMED detail codeNeed to incorporate AF/NAVY BH paperworkNeed to coordinate connection to AF/Navy resourcesHawaii, HILeader: LCDRGraceyClinical personnel:11San Antonio, TXLeader: Dr. DulinClinical personnel:21UNCLASSIFIEDClinical personnel: 9Leverage Capacity“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, MD/sean.j.hipp.mil@mail.mil/1-844-V-MEDCENAugusta, GALeader: Mr. OrrSlide 18As of: 18 November 2019
PATH/HELP OVERVIEW Established 2004 at Tripler Army Medical Center Asynchronous, web-based, HIPAA compliant, secure,provider-to-provider, multi-media, air evacuation /patient movement not limited to just deployedproviders PATH: https://path.tamc.amedd.army.mil Established 2014 at Portsmouth NH as a huband-spoke linked to PATH server HELP: https://help.nmcp.med.navy.mil“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDSlide 19As of: 18 November 2019
PATH/HELP Specialty Support“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDSlide 2020As of: 18 November 2019
Virtual Medical Center-Europe:Bringing the MEDCEN to the Warfighter Every DayEvery Day across VMC-Europe: 41 ADSM Mission Days saved by nottravelling for healthcare 35 synchronous video Virtual Healthvisits (sVH) are performed through 79operational and 56 fixed sites across 3COCOMs 10 Operational Virtual Health Visits areperformed 300 providers across 42 Specialtiesperforming Virtual Health One in twenty surgeries started atLRMC with a sVH visit6,000 sVH visits in 201814,000 Mission Days savedfor Commanders in 2018“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDVMC-Europe’s Capabilities: Integrated Asynchronous andSynchronous VH Operations Link HELP with sVH visits Interoperable, scalable web-basedconnectivity platform User platform & connectivitymethod immaterial Dynamic scheduling for patients,providers, and Nurse Presenters Bring the MEDCEN to the pointof need Personalized training for Providersand Presenters Integrate VH into daily useVirtual Health Conservesthe Fighting Force!Ref: Regional Health Command EuropeSlide 21As of: 18 November 2019
Virtual Critical CareLeveraging information and communication technologies allows a smallernumber of doctors & nurses to care for a larger number of geographicallyisolated, critically ill, patients anytime and anywhere. This system enables: Standardization of best practice medicine (quality)Decreased network disengagements (cost savings)Higher acuity and volume of spoke site admissions (readiness)On-demand operational VH support for the warfighter (lethality)“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDRef: CAPT Konrad Davis, MD, NMCSDSlide 22As of: 18 November 2019
Joint Incentive Fund (JIF) FY20-22 JIF Application The MHS is pursuing a JIF grant to beginmerger of the VA Tele-ICU and DOD VirtualCritical Care programs. If approved, this will merge VA (VISN 10 23) with DOD (TCC) programs. This will likely take 5-7 years for completeintegration.Long-Term Vision is a single federal TCCsystem involving DOD and VA hub &spoke sites, which allows DOD providersto transfer garrison beds to VA networkfor support if/when they need to focustheir support on the operational spaceor even to provide garrison-basedsupport for man-made and/or naturaldisasters.“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDRef: CAPT Konrad Davis, MD, NMCSDSlide 23As of: 18 November 2019
Remote Health MonitoringFuture Growth: Expand to new sites forenrollment Add new categoriesunder each of the 3 armsDHARemote Health MonitoringSAMHS RHMVirtual Medical CenterHealthy LifestyleHLPNCR RHMNCR CMIOSymptom MonitoringB/P MonitoringDisease ManagementDREAM“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDSlide 24As of: 18 November 2019
Virtual Video Visits (V3) UpdateDescription – VH at Patients’ Locations includes the utilization of two-way interactive audio video involving a health provider in afacility and a patient in their home or another secure location for primary and specialty care.VH IT PMO ExecutingMHS PlatformPurchase in FY20Access / Satisfaction Another access point is createdfor beneficiaries Immediate care at home, placeof business, etc. should drivesatisfactionPatient at Home w/ videodevice and necessaryperipheralsProviderSupported asappropriate by:Provider and Patient interact via two-way interactiveaudio video platform. As appropriate, NAL can triagepatients who need to see another clinician.MHS V3enterprisesolution on trackfor selection andfunding in FY20NurseAdvice LineProductivity Lower acuity triaged outside clinic Likely to reduce no show and left withoutbeing seen rates Likely to decrease ED and urgent carevisits based on civ sectorCost Avoidance Decrease in cost per visit- Primary Care- Specialty Care Decrease in PMPM“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDSlide 25As of: 18 November 2019
CENTRALIZED VIRTUAL HEALTH PRIVILEGINGDHA-PI 6025.13 – Quality (Credentialing)“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDSlide 26As of: 18 November 2019
VIRTUAL HEALTH CARE COORDINATION APPLICATION Virtual Health appointments, referral documents andclinic availability are easily updated by clinic staff Coordinates provider, virtual health care coordinator &virtual health cart information across the enterprise Automated notifications are sent to patients, referralcoordinators and nurses Periodic Health Assessments (PHA) are beingscheduled through Virtually Integrated PatientReadiness and Remote Care Clinic (VIPRR) in VHCCA Currently supports 12 Distant Site MTFs, 45 originatingsite clinics, 54 providers, 500 appointments createdand 260 users around the world“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDSlide 27As of: 18 November 2019
SUMMARYFocusQuad AimThe Virtual Medical Center construct is focused on creating programs and processes Increased Readinessthat support operational readiness and multi-domain operations Better Care Better HealthFuture state increases synchronization between the military services and activeconnections between garrison and the operational space Increased Readiness Better CareFunding will continue to be aligned under the Military Health System and theVirtual Medical Center will be aligned under the Defense Health Agency Lower Cost“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDSlide 28As of: 18 November 2019
QUESTIONS?If you would like to earn continuing education credit for this activity,please visit: http://amsus.cds.pesgce.comHurry, CE Certificates will only be available for 30 Days after this event!“Medically Ready Force Ready Medical Force”LTC(P) Sean J. Hipp, FIEDSlide 29As of: 18 November 2019
Army Medical Center, the U.S. Army Medical Department, the U.S. Army Office of the Surgeon General, the Department of the Army, the Department of the Air Force and Department of Defense or the U.S. Government." . San Antonio, TX . Leader: Dr. Dulin. Clinical personnel: 21. Augusta, GA.