Transcription
California Children’s Services(CCS) RedesignProvider Access & Provider NetworkTechnical WorkgroupKick-off WebinarMarch 18, 2015
Welcome&IntroductionsAnastasia Dodson, DHCS
Overview of AgendaDavid Banda, DHCS
CCS Redesign Technical WorkgroupsThe Provider Access and Provider Network TechnicalWorkgroup (TWG) is one of six workgroups created to facilitateand inform the CCS Redesign process. The other TWGs are: Data; Eligibility / Health Conditions; Outcome Measures / Quality; County / State Roles and Responsibilities; and Health Homes / Care Coordination / Transitions.-4-
Provider Access & Provider NetworkTechnical Workgroup DescriptionThe Provider Access and Provider Network TWG will beresponsible for providing the RSAB with relevant informationregarding the CCS program.The CCS program has established standards for all pediatricspecialty and subspecialty care across the State that will bemaintained in any organized delivery system developedthrough the redesign process.-5-
Provider Access & Provider NetworkTechnical Workgroup DescriptionThe focus of this workgroup will be to explore further potentialfor expanding the CCS network of providers, consider ways toaddress geographic disparities in access and providershortages, look at managed care access standards, andconsider provider credentialing and access standards for anorganized delivery system under CCS redesign.In addition, DHCS and UCLA will encourage coordination withJanet Coffman and her team at UCSF, who have conductedsignificant research on the supply of pediatric specialists inCalifornia, provider access issues, and potential for workforcedevelopment.-6-
Provider Access and Provider NetworkTWG Potential TopicsThe final list of topics will be identified and prioritized by the ProviderAccess and Provider Network TWG in conversation with the RSAB andother TWGs. Suggestions include: Provider paneling, current certification criteria (for hospitals, individual providers,and special care centers) and potential for expanding Setting and maintaining standards of care and provider networks across theState, and requirements of health plans and any CCS organized delivery systemfor evaluating and maintaining those standards Access to specialty providers in rural counties, and potential for schedulingmultiple same-day appointments for long-distance travel or providing additionaltravel resources to families/caregivers Potential for incorporating telemedicine and home-based health care intoenrollees’ care plan for care maintenance.-7-
Provider Access and Provider NetworkTWG MembersCo-Chairs: Nick Anas, MD – President, Children’sSpecialty Care Coalition; Pediatricianin Chief, Director Pediatric IntensiveCare Unit (CHOC Children's Hospital) David Banda – Health ProgramSpecialist (DHCS)Members: Amy Carta – Assistant Director SantaClara Valley Health & Hospital System;California Association of PublicHospitals and Health Systems Arlene Cullum – Director, Women’sAnd Children’s Ambulatory Services(Sutter Health)Members, continued: Nathan Davis – Vice President ofFinance (CCHA) David Hodge, Jr – Executive Director,Ambulatory Care (Valley Children'sHospital) Tony Maynard – Board Member /Patient (Hemophilia Council of CA) Kathryn Smith – Associate Directorfor Administration (CHLA) Abbie Totten – Director, Govt.Programs and Strategic Initiatives(Health Net, Inc.)
Existing CCSProvider SystemsDavid Banda, DHCS
CCS Service Providers Hospitals Individual Providers Pharmacies DME Providers Other Provider Types andManufacturers- 10 -
CCS Provider Standards Hospitals NICU PICU Individual Physicians Allied Health Care Providers Special Care Centers- 11 -
CCS Special Care Centers Hospital-linked Inpatient/Outpatient andStand Alone Outpatient ‘Condition based’ Multispecialty- multidisciplinary teams Annual evaluations Certain conditions require receipt ofcare at center- 12 -
CCS Approved Facilities 338 Hospitals 129 NICUs 27 PICUs 250 Other SCC- 13 -
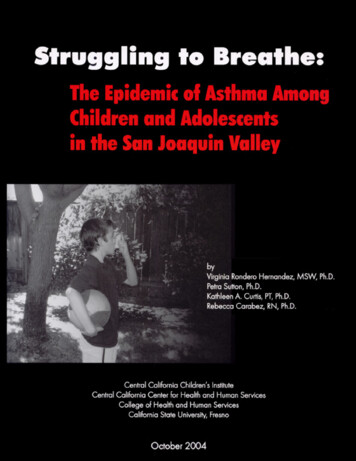
UC, CCHA, Tertiary Hospitals Map- 14 -
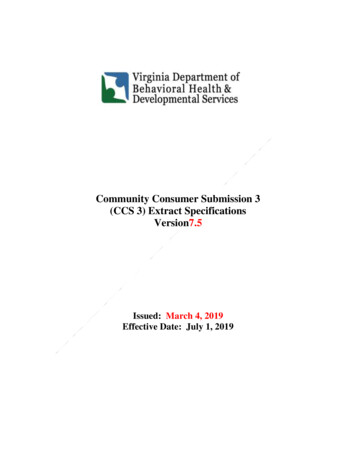
CCHA Member Hospital Map- 15 -
Hospital ApplicationType of Hospital1.Tertiary HospitalStandard Number3.3.1Referral hospital for pediatric care to children from birthup to 21 yrs. of agea) Regional NICU andb) Neonatal Surgery andc) PICU andd) Special Care Centers2. Pediatric Community Hospital3.3.2With licensed pediatric beds that provides services forchildren from birth up to 21 years of age.a)b)c)d)Community NICU orIntermediate NICU orPICU orRehabilitation3. General Community Hospital3.3.2/H.s.2.a3.3.3Without licensed pediatric beds in which care may beprovided only for adolescents 14 up to 21 years of age,length of stay shall not exceed 21 days.a)b)Community NICU orIntermediate NICU- 16 -Periodic ReviewsNo less than every three years or as deemednecessary by the CCS ProgramNo less than every three years or as deemednecessary by the CCS ProgramNo less than every three years or as deemednecessary by the CCS Program
Hospital Application, continuedType of Hospital4. Special HospitalStandard Number3.3.4The hospital has no licensed pediatric beds, but has:licensed perinatal unit/service & ICNN; licensed underspecial permit for rehab services; also providesspecialized area of: eye or ear surgery or burn center.a)b)c)Community NICU orIntermediate NICU orRehabilitation5. Limited HospitalHospital in a rural area - there are no community ortertiary inpatient hospital services available, nolicensed pediatric beds, can provide limited services tochildren & adolescents for acute short-term conditionsLOS shall not exceed 5 days.a)b)Periodic ReviewsNo less than every three years or as deemednecessary by the CCS Program3.3.4/A.1.b3.3.5No less than every three years or as deemednecessary by the CCS ProgramCCS PaneledNo specialty6. Special Care Centers(draft)3.37/C.4- 17 -No less than five-year intervals and more oftenif indicated
NICU and PICU ApplicationStandardsI .Neonatal Intensive Care Unit (NICU)1.a)b)Regional NICUTertiary HospitalNeonatal Surgery/PDA2.Community NICUa)c)Pediatric Community HospitalorGeneral Community HospitalorSpecial Hospital;3.Intermediate NICUa)Pediatric Community HospitalorGeneral Community HospitalorSpecial Hospitalb)b)c)Standard NumberPeriodic ReviewsMay be conducted on an annual basis or as deemednecessary by the CCS program.3.25.13.25.2May be conducted on an annual basis or as deemednecessary by the CCS program.No less than five-year intervals and more often ifindicated3.25.3- 18 -May be conducted on an annual basis or as deemednecessary by the CCS program.
NICU and PICU Application, continuedStandardsII. Pediatric Intensive Care Unit (PICU)1999 Standards1.Tertiary Hospital or2.Pediatric Community HospitalNeonatal Surgery/PDA(Community NICU) Tertiary Hospital Pediatric Community Hospital General Hospital Special HospitalStandard Number3.323.343.34.1/C- 19 -Periodic ReviewsNo less than every three years or as deemednecessary by the CCS program.
Recertification PeriodFacility TypeHospitalsTertiary, Pediatric, Community,General Community, SpecialCommunity, and Limited HospitalNeonatal Intensive Care Unit (NICU)Community and IntermediateRecertification PeriodConducted no less than every threeyears or as deemed necessary by theCCS Program.Conducted on an annual basis or asdeemed necessary by the CCSProgram.Pediatric Intensive Care Unit (PICU)Conducted no less than every threeyears or as deemed necessary by theCCS Program.Pediatric Intensive Care Unit (PICU)Conducted on an annual basis or asdeemed necessary by the CCSProgram.CommunitySpecial Care CentersCommentsPer Final Draft Standards for CommunityPICU, dated October 16, 2112Located within CCS approved tertiaryhospitals with CCS approved PediatricIntensive Care Units (PICU) or specialhospitals demonstrating equivalentexpertise.Not Specified- 20 -
Types of ApprovalApproval TypeDescriptionGranted when all CCS Provider Standards for thespecified facility are met.FullMaybe granted when all CCS Provider Standardsappear to be met, additional documentation isrequired by the CCS program. This type of approvalmay not exceed one year.ProvisionalFor a period not to exceed six months, may begranted when there are readily remediablediscrepancies with program standards. The specifiedfacility must present written plan for achievingcompliance with program standards, and the planmust be approved by the CCS program. If thediscrepancies are not corrected with the time framespecified by the CCS program, approval shall beterminated.ConditionalGiven based upon failure of the specified facility tomeet CCS program standards.Denial- 21 -
CCS Provider PanelingTypes of ProvidersThe following providers must be paneled by CCS in order to treat clients with a CCS-eligible medical condition: ional TherapistsOrthotistsPediatric Nurse Practitioners * Physical Therapists ProsthetistsPsychologistsRegistered Nurses *Respiratory Therapists *Social WorkersSpeech Language Pathologists*Provider type is subject to program participation limitations.Provider types not listed above do not need to be paneled by the CCS program to treat CCS clients.National Provider Identifier RequiredAll providers applying for CCS paneling must be enrolled as a Medi-Cal provider and have a valid National Provider Identifier(NPI) to become CCS-paneled.Additional information regarding enrolling an NPI with Medi-Cal can be located at http://files.medical.ca.gov/pubsdoco/npi/npi.asp.- 22 -
CCS Provider Paneling, continuedPanel ApplicationsThe application for becoming paneled by CCS has two versions: A California Children’s Services (CCS) Program Individual ProviderPaneling Application for Physicians and Podiatrists (form DHCS 4514) and a California Children’s Services (CCS) Program IndividualProvider Paneling Application for Allied Health Care Professionals (form DHCS 4515). Physicians, podiatrists, and allied healthprofessionals can apply online or with a hard copy via fax or United States Postal Service. Allied provider applications are never autopaneled. Allied providers need to provide supporting information that must be reviewed by an analyst Visit the CCS website at www.dhcs.ca.gov/services/ccs/pages/default.aspx and click on “Forms,” located under the “CountyCCS Programs” heading. Visit the Medi-Cal website at www.medi-cal.ca.gov, click on “Forms,” and scroll down to “California Children’sServices (CCS).”Applying online Visit the http://www.dhcs.ca.gov/services/ccs page on the DHCS website. Under the “Providers” heading, click on “Becoming aCCS Provider”: Enroll.aspx Click on the following hyperlink, located near the bottom of the “Becoming a CCS Provider” sp. Enter the code provided in the text box and complete the online application.If the online application system indicates additional information is required, fax the information to (916) 440-5299.Auto-Paneled – This is when the provider successfully inputs all required information into the website and the system automaticallypanels the provider. A certificate is generated and there is nothing more for the analyst to do. This scenario is not available to alliedproviders, such as Audiologists.Auto-Pended – Provider inputs their information into website and receives a pending status. A physician may be required to submitmore information before being fully paneled. Allied providers are always put into a pending status because requirements for panelingof allied providers requires analytical review of required documentation submitted to meet the specific allied practioner’srequirements. Once an application is denied due to the provider not submitting the requested information, the provider must provide anew application should they wish to paneled- 23 -
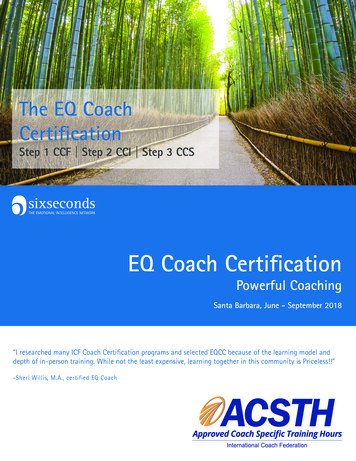
CCS Provider Paneling, continuedPhysician PanelingPhysicians may be paneled with full or provisional approval status, described as follows.Full ApprovalPhysician applicants who meet all criteria required for paneling, including certification by the American Board of MedicalSpecialties (ABMS) will be given full panel approval.Provisional ApprovalIf the physician is board eligible for the certifying examination, provisional paneling status will be given to the physicianfor three years upon completion of residency or fellowship training. Upon successful completion of the boardexamination, the physician must provide an ABMS certificate immediately by faxing the number listed below or bymailing to the Systems of Care Division Provider Paneling Unit.Paneling StatisticsIn 2014 approximately 10,000 Physicians and Allied Professionals were paneled 84% were Physicianso 8,560 paneled/yearo 778 paneled/montho 60% used the Auto-paneling featureo 7% were either automatically Pended or madeProvisional awaiting additional information 16% were Allied Professionalso 1,700 paneled/yearo 154 paneled/monthSource: CMS NetNote: means approximately- 24 -
Comments fromCo-ChairNick Anas, MDChildren’s Specialty Care Coalition
CCS Provider Access & Networks:Overall ConsiderationsHow can we develop and ensure an integrated andadequate network of primary care and specialty carephysicians? ACO strategy to aggregate primary and specialty careproviders. Economic models to include physicians and hospitals. Care models to address quality, cost, access, andpatient satisfaction. Assess current provider standards and credentialing.- 26 -
Maintain Quality of CCS NetworkCCS Redesign effort should maintain the CCSstandards for Provider training, certification, andperformance; sustain regional provider networks;primary and specialty care Providers must formintegrated Networks; there must be a “whole-child”approach to care/the development of the medicalhome concept.- 27 -
Use Data to Assess Current AccessDetermine the spectrum/severity of the Provideraccess issues, and determine the barriers toaccess. In this process, identify the specificphysician specialties or primary care Providersthat are difficult to guarantee access and todetermine which regions of the State are mostimpacted.- 28 -
Focus on Solutions Focus on solutions to improve access:recruitment and retention of physicians; use ofmid-level providers to provide care; use oftechnologies like telemedicine and electronicreferrals to enhance access. Review outcomes from pilots Use data and technology to measurenetwork/access activity and performance to dateand going forward- 29 -
Group Discussion & QuestionsJessica Padilla: jessicap@ucla.eduDavid Banda: v.david.banda@dhcs.ca.govNick Anas: - 30 -
Provider Network and Provider AccessTWG Workplan & Next Steps Key Priority Areas Obtaining Input Need for Evidence to Guide Decisions Relationship with other technical workgroups Resources & Capacity Timeline Homework & Next Steps- 31 -
care at center - 13 - CCS Approved Facilities . 27 PICUs 250 Other SCC - 14 - UC, CCHA, Tertiary Hospitals Map - 15 - CCHA Member Hospital Map - 16 - Hospital Application Type of Hospital . Standard Number Periodic Reviews ; 1. . specialized area of: eye or ear surgery or burn center. a) Community NICU or b) Intermediate NICU or :