Transcription
UNION BENEFITS TRUSTHOW TO ENROLL IN YOUR DENTAL,VISION AND BASIC LIFE BENEFITSFOR MEMBERS WITH AT LEAST ONEYEAR OF SERVICEbenef its
r:Dear UBT Membeployversary of state emnianaryeeonurhed you have almost reac).Congratulations! YoBenefits Trust (UBTonniUethofrbement and as a mem:ployees,s Trust’s mission issented public emreep-ronniUtoeesThe Union Benefitn of their respectivbenefits and servictioyialitecuapr-qapghrhieithereTo delivto enhancl quality of life andalerovreithhricchto ene benefits for whithtouabnarletounions.lp you beginas designed to heweidguisth,chAs sule.you are now eligibThese benefits are:talge with Delta Den Dental CoveraPwith EyeMed or VS Vision Coveragelatiao.gov or by usingrance with PrudenhisuInyOmfeLiatcesilinBaon coverageonline atdental and visions representative orfitnebecyenofYou may enroll inagailable from yourcur within 31 daysavoctrmusfomttenenllmllmroropaper enthe nextInfo Tab. Enrtunity to enroll isunder the Forms &pog,oport.xtusnetretsthefie,benthat your coverageu miss this deadlinreyosuIf.entelpdaheyillarwrsleas possibyour annivedate. Eachd. Enrolling as soonment anniversaryriooypepltenemurllmyororuenteopenemium costs for yost of the month afprfirelyththllyonmuaeusthy,klt UBT paysbegins quice time of service, buthatsstcovehaplan willd in thetomatically enrollemembers.aueilyarmufaYolee.ibigncelradanlife insutions can becost for the basicpossible. DesignaasonsoasryUBT also pays theiaficctionsld declare a fbasictstrust.ora paper. Visit benefiationmade online or viore detailed informmrFos.fitnsnetiobeopuron bothmary of yoe atnded to be a sumBT customer servicUtacntcoorgorThis booklet is intetstrust.Pleaseplease visit benefibenefitstrust.org.e@icrvseeromon these benefits,strmationepartment; all info0-228-5088 and cuDs80ceorur55soRe228an50614your Humme.dress current withmailed to your hobeillwtskitenllmkeep your home adenroniversary and openincluding your anserving you.We look forward toeChristopher A. Mabfits TrustChair, Union BeneAFSCME Local 11President, OCSEA,Trustees & Staff,tUnion Benefits Trus2
CONTENTSIntroduction. 4Dental and Vision Plans. 5Eligibility . 5Enrollment. 7Your Coverage. 8Cobra. 8MyUBT. 8Dental Plan.9Plan Comparison Chart.10Benefit Information.12Payment Chart.12Claims.13Exclusions and Limitations.14Vision Plans.15Compare the Plans.16Benefits Summary.16Early Coverage.17Cosmetic Options.17Low Vision Benefits.17Additional Discounts.17Laser Surgery .18Exclusions and Limitations.19Coordinating Benefits.20COBRA.21Basic Life/Accidental Death.22Eligibility & Enrollment.22Basic Life Insurance Benefits.22Basic Annual Earnings.22Accelerated Death Benefits.22Accidental Death Benefits.23Life Exclusions & Benefits.24Beneficiaries & Claims .25When Your Benefits End.26Portability and Conversion.26Plan Administration.27Contacts.Back Cover3
INTRODUCTIONAbout the TRUSTUnion Benefits Trust exists toprovide high-quality benefits andservices to Union-representedpublic employees who work forthe State of Ohio. Since 1993, UBThas offered benefits to Unionrepresented State employees, andcurrently serves approximately35,000 employees represented byOCSEA/AFSCME Local 11,District 1199/SEIU, OSTA, FOP/OLC,SCOPE/OEA and CWA.About this bookletThis booklet describes three UBTbenefits:Dental PlanThis booklet describes the UBTDental Plan effective July 1, 2010.This plan booklet replaces theprior booklet and is incorporatedwith the Administrative Servicesagreement with Delta Dentalto form the complete contract. Itcontains highlights of the benefitsoffered by UBT. If a discrepancyexists between the informationin this booklet and the DentalPlan Document, the Dental PlanDocument prevails over this planbooklet.Vision PlansThis booklet also describes theUBT Vision Plans effective July1, 2014. It contains highlights ofthe benefits offered by UBT. If adiscrepancy exists between theinformation in this booklet and theVision Service Plan Document andaddendum or the Vision BenefitPlan Agreement between UnionBenefits Trust and EyeMed VisionCare, these documents prevail overthis plan booklet.Basic Life/AD&DThis booklet describes the UBTBasic Life insurance benefits effective July 1, 2014. If a discrepancyexists between the informationin this booklet and the Basic LifeInsurance booklet-certificate andthe Group Insurance Contract fromPrudential, the Group InsuranceContract prevails.4Answering yourquestionsThis booklet outlines eligibilityrequirements, benefits payable andbenefit limitations. It has beenspecially designed to make it easierfor you to find information you needto understand your benefits. Weencourage you to use this summaryas your first source of informationwhen you have questions. If youcannot find an answer to yourquestion, please contact UBT,Delta Dental, EyeMed, VSP orPrudential, using the informationon the back cover of this booklet.For eligibility questions, contact UBTat 800-228-5088.If a discrepancy exists between plandescriptions in this booklet and theSummary Plan Description, the PlanDescription documents takeprecedence.FORMS All forms are available atbenefitstrust.org underthe Forms & Info Tab or you may call our customerservice line 800-228-5088or 614-508-2255 or email customerservice@benefitstrust.org andrequest to have a formmailed to your home.
DENTAL & Vision ELIGIBILITYEmployeesMembers of participating Unionsare eligible for dental and visionbenefits after one year ofcontinuous State service.Coverage for unmarried dependentchildren will end at age 19, unlessyou supply appropriate documentation of the following conditions:Your HR Representative can provide more details about the typesof required documentation neededfor dependent coverage.To be eligible, you must first bea full or part-time permanentemployee and a member of: Children from age 19 until theend of the month in whichthey reach age 23 may becovered if they are primarilydependent on you for maintenance and support and areattending an accredited school.A divorced spouse is not eligibleas a dependent and no person isconsidered a dependent whilein the armed forces. Any personliving outside the United States orCanada is not considered acovered dependent. Children of any age who areprimarily dependent on youand incapable of self-supportdue to developmentaldisabilities or physical handicapwill be eligible as long as youmaintain your eligibility.Remember that if you aremarried and your spouse hascoverage through his or heremployer, coordinated benefitsmay apply. See the section onCoordinating Benefits on page 20. OCSEA/AFSCMEUnits 3-9, 13, 14, 45, 50, 55 District 1199/SEIUUnits 11, 12 OSTAUnits 1, 15 FOP/OLCUnits 2, 46, 48 SCOPE/OEAUnit 10 or CWAUnit 40.Established term employees areeligible unless excluded by anagency-specific agreement.There is no premium cost toyou for dental and visioncoverage for yourself and/oryour eligible dependents.DependentsIf you, the member, are eligible forUBT benefits, you may cover yourcurrent legal spouse andunmarried dependent children,including those born to you,residential stepchildren, fosterchildren, legally adopted childrenand children for whom you havelegal guardianship. Dependent children must be dependent on youfor support and maintenance.To obtain eligibility, documentation is required and will need to beprovided: when you first enroll when the child is first eligible for dependents over 19.Coverage will not be provided fordependents until the eligibility documents are received and approved.Details for required documentationfor dependents is available atbenefitstrust.org.Two Stateemployeesin the familyWhen you and your spouse areboth State employees, one maycarry family coverage and the othersingle coverage, provided that thespouse is not listed as a dependentunder family coverage. A child whois eligible for coverage as a Stateemployee is not eligible as thedependent of a parent who is alsoa State employee.Dental and vision benefitsare not affected by the2010 Health Care ReformAct (ACA).As a result, dependents age19 (or 23 if a student) cannotcontinue on your dental andvision coverage even thoughthey may be coveredunder your health plan.5
DENTAL & VISION ENROLLMENT and ChangesEFFECTIVE DATESENROLLINGMembers who are actively at workcan enroll in dental and vision coverage after one year of continuousState service. Coverage starts onthe first day of the month following one continuous year of Stateservice if you enroll within 31 daysof becoming eligible.It is not necessary to enroll inmedical health care to enroll in theUBT Dental or a Vision Plan.For example, if your hire date isJuly 15, 2013, you must enrollwithin 31 days of July 15, 2014 forcoverage to begin on August 1,2014. If you do not enroll within31 days of becoming eligible, youmust wait until a Trust-sponsoredopen enrollment.If you already have one year ofservice, you can enroll or makechanges during open enrollment.Once enrolled, you may makechanges at each subsequentTrust-sponsored open enrollment.Coverage elected during openenrollment will be effective on theJuly 1st following, as long as allappropriate forms are received bythe enrollment deadline.Coverage for enrolled dependentsis effective on your effective date.Dependents you acquire after youenroll become eligible forcoverage as shown on the FamilyStatus Changes chart to the right,provided they are eligible andyou enroll them for benefits bythe appropriate deadline with theappropriate documentation.Cost of CoverageThere is no premium for dentalor vision coverage. UBT pays yourdental and vision premiums.You must enroll in the plan(s) toreceive coverage, it is not automatic.Once enrolled, you do not needto enroll again unless you wish tomake a change; however, it isimportant to review your coverageand dependents annually.See page 7 for online enrollmentinstructions or you may complete apaper form and submit it toyour HR. Forms are available atbenefitstrust.org under theForms & Info Tab. Online and paperenrollments must be completedwithin 31 days of your anniversarydate.If you do not enroll within 31 daysof your anniversary date, you mustwait until the next annual openenrollment period to obtain dentaland/or vision coverage.When YOURcoverage BEGINSTypically, your dental and visioncoverage will be effective the firstday of your 13th month of continuous state service.FAMILYSTATUS ChangesYou may change your coverage level(single or family) during the annualopen enrollment or during the yearif you have a family or employmentrelated status change that affectsyour coverage. Changes must bemade within 31 days of the event oryou will have to wait until the nextTrust sponsored open enrollment toadjust your coverage level. Reviewthe chart below, and see your HRRepresentative for more information.Family status changesChangeCoverage ChangeAllowedDate Change EffectiveMarriageAdd dependent spouse(add spouse’s children)First of month followingmarriageBirth or adoptionAdd dependent childDate of birth or placementin homeDivorce (you providedcoverage)Drop spouseLast day of month in whichdivorce occurredDeath of dependent (youprovided coverage)Drop dependentLast day of the month inwhich death occurredEnroll in coverage, addLoss of coverage throughdependentspouse’s employer due tolayoff, termination, death ordivorceDate varies by type ofchange; see your HRRepresentativeReturn to work througharbitration order orgrievance settlement oradministrative orderRe-enrollDate varies by settlementagreement; see your HRRepresentativeDependent return toschoolReinstate dependentcoverage1st month following termstart date6
Enrollment instructionsEnroll in dental and vision coverage online at: myOhio.gov or byusing a paper enrollment formavailable online atbenefitstrust.org, under theForms & Info Tab, from your agencybenefits representative or bycalling UBT at 800-228-5088 or614-508-2255.A. ONLINE You may enroll on-line atmyOhio.gov beginning thesecond business day followingyour one-year anniversary date. Enter your State of OhioUser ID and password,click “SIGN IN;” On toolbar clickHEALTH & BENEFITS Tab Select BENEFITS SUMMARYfrom drop down menuThe Benefits Summary pagewill open; Click on “Enroll in Benefits” Click the “SELECT” button onthe benefit enrollment pageSubmit your selections throughmyOhio.gov within 31 days ofyour anniversary date. Make sureyour online elections are correctlysubmitted and that you receive aconfirmation message. Print andkeep a copy for your records.OnlineAccess hoursNon-Payday WeekMon. - Thurs.Available 24 hours/dayFriday.All day until 7 pmSat. and Sun.UnavailablePayday WeekMon. - Fri. .Available 24 hours/daySaturday.All day except 4-6 pmSunday.UnavailableB. paperObtain a paper dental andvision enrollment form online at benefitstrust.org, from your agency’s humanresource office, or call UBT at 800-228-5088 tohave one mailed to your home.Give the completed, signed anddated form to your agency’shuman resource office within 31days of your anniversary date.ENROLLING DEPENDENTSIf you are enrolling yourdependent(s) in your dental andvision coverage, you are requiredto provide the required eligibilitydocumentation for your dependents. A listing of the requireddocuments can be found at:das.ohio.gov/eligibilityrequirement. Coverage will not be provided for dependents until theeligibility documents are receivedand approved by your agency’s human resource office. If the requireddocumentation is on file with youragency’s human resource office asa result of enrolling in a medical7plan, you may not need to resubmit.Be sure you have a valid mailingaddress on file at myOhio.gov.Information regarding your benefits is mailed to that address fromDAS and UBT. It is your responsibility to ensure that your currentaddress is on file. You may list a P.O.Box as a mailing address but not asa home address.BenefitReference Cardsfor dental andvisionA card is not required to receiveservices at your dental or visionprovider’s office for yourconvenience.You have an option to printreference cards for you and yourfamily’s dental and vision benefitvisits. Simply1. link from UBT’s websitebenefitstrust.org toDelta Dental & VSP.2. register and create a password fora secure login.3. print a card with your name andgroup number (which can beused for all familymembers).4. for Eyemed, print reference cardat benefitstrust.org under theVISION tab.
Your DENTAL & VISION coverageWhen you are onleaveIn some cases your dental andvision coverage may continue whenyou are not actively at work for thelength of your authorized Stateleave. See your HR Representativefor details.WHEN YourCoverage ENDSGenerally, coverage is extendedthrough the end of the monthfollowing the month state serviceterminates. For example, typically,if you leave State employment inJuly, and UBT receives a contributionin July, UBT will pay your last dentalor vision premium for August. Yourcoverage would end August 31.However in certain circumstances,you may be able to continue yourdental and vision benefits throughCOBRA. See page 21 for more information.When yourdependent(s)coverage endsYour dependent benefits will endon the last day of the month inwhich your dependent no longermeets the definition of an eligibledependent or the date your benefits end. See page 5 for dependenteligibility.CoBRAYou are responsible for notifyingUBT when your dependent(s)is no longer eligible to receivedental and vision coverage underyour benefits. At no time is youroverage dependent automaticallyenrolled in COBRA for dental andvision, even if they have enrolledin COBRA for the state’s medicalplan. See page 21 for more information.Contact UBT at 800-228-5088 or614-508-2255 or email tocustomerservice@benefitstrust.org.8Access your member-specificbenefits at benefitstrust.org.Click MyUBT to register andcreate a password for a securelogin. Check you plan coveragesfor dental, vision, lifeand legal Check what dependentsyou have covered Find out how muchlife insurance youhave for you and yourdependentsTo access network providersyou do not need to create apersonal account. Link to all plannetworks via the PLANS tab.Find forms and booklets via theFORMS & INFO tab.View Frequently AskedQuestions via the FAQ tab.
DENTAL BENEFITSUBT Dental PlanYour UBT Trustees have selectedDelta Dental of Ohio as your dentalcarrier effective July 1, 2010.The UBT Dental Plan coversdiagnostic and preventativeservices at 100% and no annualdeductible is required forClass 1 or 4 services. You mustmeet the annual deductible of 25 per person, for Class 2 and 3services, before benefits are paid.Benefits will be paid up to themaximum annual benefit amountof 1500 per person per plan year.Out-of-pocket costs may varydepending on the provider youchoose. You will be covered byone plan, but your savings aredetermined by the dentist youchoose.One plan, three levels of coverage elta Dental PPO providersDoffer the highest level of savings and cannot balance-billyou for additional payment forthe services you received. Thatmeans no additional out ofpocket expenses. elta Dental PremierDproviders are in the secondarynetwork. While you receive amore modest savings compared to the PPO dentist, youwill have many more dentiststo choose from than the PPO.You cannot be balance-billedfor the difference between thedental charge and the allowedamount. on-participating providersNwill balance-bill you for anyamount that exceeds DeltaDental’s allowed amount.They may ask you to pay thefull amount up front and mayhave you submit your claiminformation to receivereimbursement.PLAN ADMINISTRATIONThe UBT Dental Plan is administered by Delta Dental of Ohio, aThird Party Administrator (TPA) withtwo dental provider networks: theDelta Dental PPO and Delta DentalPremier. With two networks available the UBT Dental Plan offersaccess to more in-network providers and thus greater savings to itsmembers.The UBT DENTAL Plan also has anout of network benefit. So you cansee any dentist you choose and theplan will pay, however benefits arebetter in one of Delta Dental’s twonetworks.For a summary of benefits and thepercentages of dentists’ fees theplan pays in the PPO, Premier or outof network, see the chart on pages10 and 11. See Page 12 for plan payment examples by network.You must meet a deductible of 25 per person each plan yearbefore benefits are payable forrestorative services, oral surgery,endodontic, periodontic andprosthodontic services (Class 2and 3 services combined).Finding a ParticipatingDentistTo find the names of participating dentists near you, callDelta Dental’s customer servicedepartment toll-free at 877334-5008. The DASI (Delta’sAutomated Service Inquiry)system is available 24 hours aday, seven days a week, and canprovide you with the names ofparticipating dentists. You canalso check the Delta Dentallink under the PLANS tab, or godirectly to deltadentaloh.com.Pre-treatmentestimateA pre-treatment estimate isrecommended for services over 300. It outlines what the plan willpay, giving you an idea as to theportion of the cost that will beyour responsibility. See page 13 forclaims information.Network feeA discounted fee negotiated byDelta Dental for services fromnetwork providers.9
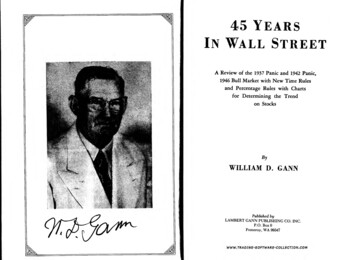
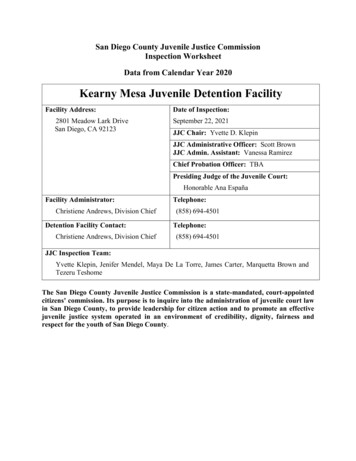
UBT DENTAL PLANThis chart presents a summary of benefits and reflects the amount that the plan pays for your treatment orservices. Please read the sections that follow for details on plan benefits and limitations. Benefit Classes 2 and3 are subject to the annual plan deductible of 25 per person. Benefit Classes 1 and 4 have no deductible.PPODentistAnnual Maximum 1500 per person per benefit yearCLASS 1 SERVICESDiagnostic and Preventive ServicesOral Exams twice per plan yearCleanings (prophylaxes) twice per plan yearFull mouth x-rays once in any three year periodBitewing X-rays twice per plan yearTopical fluoride treatment for age 18 and under or age 55or older, twice per plan yearSpace maintainers, age 18 and under, once per lifetimeEmergency palliative treatment (temporary pain relief)Sealants for unblemished permanent molars for age 18and under, once per tooth, per three year periodBrush t*Plan Pays Plan 00%65%65%*100%100%65%65%65%*65%*CLASS 2 SERVICES (annual 25 deductible applies)Restorative ServicesFilingsRoutine extractionsRelining and rebasing of existing removable dentures,once in any three year periodRepair or re-cementing of crowns, inlays, onlays,dentures or bridgeworkOral SurgeryComplex extractions or removal of tooth or rootGeneral anesthesia when medically necessary inconnection with a covered dental serviceAntibiotic injectionsEndodonticRoot canal, pulp capping, pulpotomy or therapy fordiseases of the soft tissuePeriodonticsTreatment of diseases of the gums and tissuePeriodontal maintenance cleanings following some formof periodontal treatment10
PPODentistAnnual Maximum 1500 per person per entist*Plan Pays Plan Pays*CLASS 3 SERVICES (annual 25 deductible applies)Prosthodontics (crowns, implants, bridges,dentures)Installation of fixed bridgeworkInstallation of implants and implant relatedservices, once per tooth in any five year periodInstallation of a partial removable or fullremovable dentureCrowns, inlays, and onlays up to one suchrestoration to the same tooth surface, oncein any five year periodReplacement of an existing removable denture orfixed bridgework. Must be due to the loss of oneor more natural teeth after the existing denturewas installed or if the existing denture or bridgework is at least five years old and unserviceableReplacement of an existing immediate temporaryfull denture by a new permanent full denture.Must be necessary because the existing denturecannot be made permanent and the permanentdenture is installed with 12 months after theexisting denture was installed.Addition of teeth to an existing partial removabledenture. Must be needed to replace one or morenatural teeth removed after the existing denturewas 60%50%50%*60%50%50%*60%50%50%*CLASS 4 SERVICESOrthodontia (children only)Lifetime Orthodontic Maximum 1500Services for the treatment of irregularities of theteeth and their correction, including appliancetherapy, so as to bring about proper occlusion.Dependent children are eligible until the end ofthe month in which the child reaches age 19 or23 if a student.50%up to 1,500**50% up to 1,500**50%* up to 1,500**The Annual Maximum Payment per person, per benefit year is 1,500 for all services except Orthodontics.The Annual 25 Deductible is for class 2 and class 3 services combined.**The separate lifetime maximum payment for orthodontic services is 1,500 per person.Orthodontic payment is based on the treatment plan submitted by the dentist including but not limited to the date of thebanding or placement of the appliance, and the number of months of treatment. Payment begins once the bands or theappliance is placed and will continue on a monthly basis as long as you are eligible under the dental plan until the end oftreatment or your 1,500 maximum has been met.*The percentages in the “Nonparticipating Dentist’ column will be paid based on Delta Dental’s Allowed Amount fornon-participating dentists for that service, not necessarily the amount the dentist bills. This could leave a balance due,which you are responsible for. See the example on page 12.11
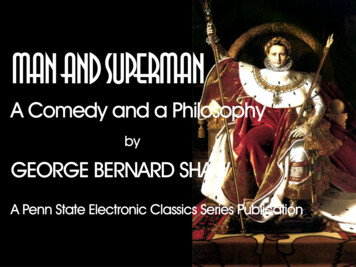
dental benefit informationConditions forproviding benefitsCertain plan benefits, as explainedin the next section, are payableaccording to important conditionsdescribed below.Alternate benefitDental benefits will be based onthe materials and method oftreatment which cost the least andwhich, in the opinion of the claimsadministrator, generally meetaccepted dental standards.Dental has the right to a refundfrom you. The refund amount willequal the difference between whatwas actually paid and what shouldhave been paid. Instances whererefunds may occur: when you failto pay all or some of the expensesyou’re required to, or another partypays all or some of the expenses onyour behalf. Annual deductible appliesto Class 2 and 3 servicescombined Full mouth x-rays have a 3 yearfrequency Class 3 appliances have a fiveyear frequency limit Orthodontia has a separateonce in a lifetime benefit; thelifetime maximum payment is 1,500Plan limitsGenerally, plan benefits arelimited by the frequency orbenefit amount per plan year.A full description is available online,or you can get a copy from the UBT.Overpayments Plan year July 1 to June 30If the plan pays more than it shouldfor expenses incurred by you oryour covered dependents, Delta Plan year benefit 1,500 perpersonExample of UBT Dental Plan paymentPPO DentistPremier DentistNon-participating DentistFile claim andreceive paymentThe PPO DentistWhat is thepayment basedon?The billed fee or the amountin your dentist’s local PPO FeeSchedule1, whichever is less.The billed fee or theMaximum Approved Fee2,whichever is less.The billed fee or the Nonparticipating Dentist Fee3,whichever is less.Payment exampleof a Class 2dental benefit(assuming anyapplicabledeductiblehas been met)Billed Charges: 100.00Billed Charges: 100.00Billed Charges 100.00PPO Fee Scheduleamount: 76.00MaximumApproved Fee: 92.00Non-Par DentistFee amount: 88.00Delta Dental pays100% of the PPOfee schedule: 76.00Delta Dental pays65% of the MaximumApproved Fee: 59.80Delta Dental pays 65% of theNon-Participating DentistFee amount: 57.20Member pays: 0.00Member pays:Member pays:The PPO dentist cannot chargeyou the 24 difference betweenthe PPO Fee Schedule amountand his/her fee.The Premier Dentist 32.20The Premier dentist cannotcharge you the 8 differencebetween the MaximumApproved Fee and his/her fee.You 42.80Because the dentist does notparticipate, you are responsiblefor the difference between Delta’spayment and his/her fee.A PPO Dentist is one that has agreed to the PPO Fee Schedule, which is lower than Maximum Approved Fee used for adentist who participates in Delta Dental Premier.1Maximum Approved Fee is the maximum amount approved for a specific procedure determined by Delta Dental in thePremier program.23Non-participating Dentist Fee is the maximum fee allowed when the dentist does not participate.12
CLAIMSSeeking a pretreatment estimate(Pre-determination)You can find out what your planpays before your d
District 1199/SEIU, OSTA, FOP/OLC, SCOPE/OEA and CWA. ABOUT THIS BOOkLET This booklet describes three UBT benefits: Dental Plan This booklet describes the UBT Benefits Trust and EyeMed Vision Dental Plan effective July 1, 2010. This plan booklet replaces the prior booklet and is incorporated with the Administrative Services