Transcription
Ulcerative Colitiswww.badgut.org and incidence yet reported in the world, withapproximately 104,000 diagnosed individuals.Symptoms/ComplicationsRectal bleeding, in varying amounts, occurs inmost patients, where blood is obvious within and onthe surface of the stool. The second most frequentsymptom is diarrhea, accompanied by crampingabdominal pain. Symptom intensity can range frommild to severe. Low red blood cell count (anemia)can result if diarrhea and blood loss are severe.Constipation can also develop, as the body strugglesto maintain normal bowel function.Since ulcerative colitis is a systemic disease, somepatients will have extra-intestinal manifestationsincluding fever, inflammation of the eyes or joints, ulcersof the mouth, or tender, inflamed nodules on the shins.After having ulcerative colitis for about 10-15years, patients are at a slightly increased risk forcolorectal cancer, so screening for this diseaseshould be at an earlier and more vigilant schedule inthis group than for that of the general population.DiagnosisA physician carefully reviews the patient’smedical history. Blood tests are useful in assessinginflammation activity level, whether blood losshas resulted in anemia, and the overall health andnutritional state of the patient. Stool sample analysiscan sometimes be helpful.It takes time to obtain a diagnosis so it is a goodidea to keep a journal or diary about symptoms,Photo pablocalvog - Fotolia.comUlcerative colitis is a chronic inflammatory boweldisease (IBD) consisting of fine ulcerations inthe inner mucosal lining of the large intestine.Inflammation starts at the lower end of the colon, justabove the anus, and extends upward in a continuousmanner, to variable distances. When only a smallportion of the lower intestine is involved, this isa milder form of the disease known as ulcerativeproctitis. If this applies to you, ask for our UlcerativeProctitis pamphlet.Ulcerative colitis is unrelated to ulcers foundelsewhere in the gastrointestinal tract, such asstomach or duodenal ulcers, but it has manysimilarities to Crohn’s disease, another IBD. Themain differences between Crohn’s disease andulcerative colitis are that, in Crohn’s disease, theinflammation extends into the bowel muscle wall andcan affect any part of the digestive tract, whereas inulcerative colitis, disease is limited to the surfacelining of the colon. For more details, ask about ourInflammatory Bowel Disease booklet.The cause of ulcerative colitis is undeterminedbut there is considerable research evidence to suggestthat interactions between environmental factors,intestinal bacteria, immune dysregulation, andgenetic predisposition are responsible. There is anincreased risk for those who have a family memberwith the condition. Although there is a range oftreatments to help ease symptoms and induceremission, there is no cure.A diagnosis of ulcerative colitis can occur at anypoint throughout life, with a high occurrence inyoung children and then again around 40-50 yearsof age. Currently, Canada has the highest prevalenceUlcerative Colitis GI Society 1
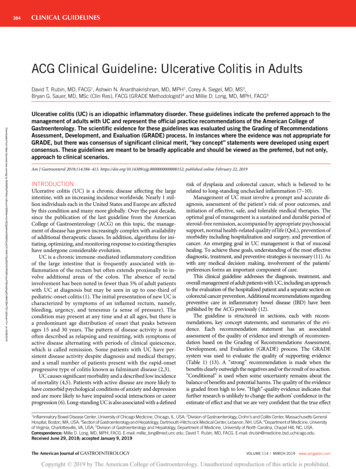
when they appear, and how you feel. As you discussthese symptoms with your physician, he or she willbe in a better position to form a diagnosis for you.Your physician will determine which of severalprocedures is best to assess your intestinal symptoms.X-rays allow the physician to view the contours of thebowel. The procedure requires the patient to undergoa barium enema. This provides contrast that helpsthe intestine show up on X-ray. Scopes may help todetermine the nature and extent of the disease. Inthese procedures, the physician inserts an instrumentinto the body via the anus (sigmoidoscope/colonoscope) to allow for visualization of the colon.The scopes are made of a hollow, flexible tubewith a tiny light and video camera. An advantageof these procedures over a barium X-ray or virtualcolonoscopy (CT scan) is that a physician may biopsysuspicious-looking tissue at any time during theexamination for subsequent laboratory analysis.Once all of this testing is complete, and otherpossible conditions are ruled out, your physician maymake a diagnosis of ulcerative colitis.Colontargeted to reduce the underlying inflammation. Thegoal is to heal the lining of the colon and to stay inremission.Dietary and Lifestyle ModificationsAs most nutrients are absorbed higher up inthe digestive tract, persons with ulcerative colitisgenerally do not have nutrient deficiencies; however,other factors may influence the patient’s nutritionalstate. Disease symptoms may cause food avoidance,leading to food choices that might not provide abalanced diet. If bleeding is excessive, problems suchas anemia may occur, and modifications to the dietwill be necessary to compensate for this.Better overall nutrition provides the body withthe means to heal itself. Depending on the extentand location of inflammation, patients may have tofollow a special diet, including supplementation. It isimportant to follow Canada’s Food Guide, but thisis not always easy for individuals with ulcerativecolitis. We encourage each patient to consult aregistered dietitian, who can help set up an effective,personalized nutrition plan by addressing diseasespecific deficiencies and the patient’s sensitivedigestive tract. Some foods may irritate the boweland increase symptoms even though they do notaffect the disease course.In more severe cases, it might be necessary toallow the bowel time to rest and heal. Specializeddiets, easy to digest meal substitutes (elementalformulations), and fasting with intravenous feeding(total parenteral nutrition) can achieve incrementaldegrees of bowel rest.RectumSymptomatic Medication TherapyAnusArea Affected by Ulcerative ColitisInflammation starts at the anus and extendsup into the colon. It may involve only a shortsegment or as much as the entire colon.ManagementThe treatment of ulcerative colitis is multifaceted; it includes managing the symptoms andconsequences of the disease along with therapies2GI Society Ulcerative Colitis The symptoms are the most distressingcomponents of ulcerative colitis, and direct treatmentof these symptoms, particularly pain and diarrhea,will improve quality of life for the patient. A numberof treatments exist to address diarrhea and pain.Dietary adjustment may be beneficial and antidiarrheal medications have a major role to play. Forpainful symptoms not controlled by other drugs,analgesics can be helpful, with acetaminophen(Tylenol ) being the preferred choice.There are two types of anti-diarrheal medicationswww.badgut.org
directed at preventing cramps and controllingdefecation. One group alters the muscle activity ofthe intestine, slowing down content transit. Theseinclude: nonnarcotic loperamide (Imodium );narcotic agents diphenoxylate (Lomotil ), codeine,opium tincture and paregoric (camphor/opium);and anti-spasmodic agents hyoscyamine sulfate(Levsin ), dicyclomine (Bentylol ), propantheline(Pro-Banthine ), and hyoscine butylbromide(Buscopan ).The other group adjusts stool looseness andfrequency by soaking up (binding to) water,regulating stool consistency so it is of a formand consistency that is easy to pass. These workin different ways; some, such as Metamucil or Prodiem , come from plant fibres, whereascholestyramine resin (Questran ) is a bile saltbinder. Interestingly, plant fibres are also useful forconstipation, due to their stool regulating effects.If extra-intestinal signs of ulcerative colitis occur,such as arthritis or inflamed eyes, the physician willaddress these conditions individually, as the patientmay require referrals to other specialists. If anxietyand stress are major factors, a program of stressmanagement may be valuable. Ask for our pamphleton Stress Management.Individuals with ulcerative colitis may be anemicfrom chronic blood loss. Adding dietary supplementscould help improve this condition, with heme ironpolypeptide (Proferrin ) being the preferred choice,due to its quick-acting and low side effect profiles.The most widely prescribed antibiotics areciprofloxacin (Cipro ) and metronidazole (Flagyl ,Florazole ER ). Broad-spectrum antibiotics areimportant in treating secondary manifestations ofthe disease, such as peri-anal abscess and fistulae.Anti-inflammatory Medication TherapyThis comes in many forms, using various bodysystems to effect relief. A physician may prescribeany of the following medications alone or incombination. It could take some time to find the rightmix for any specific patient, as each case of ulcerativecolitis is unique. Depending on the location of yourdisease, the combination of drug delivery method(oral and rectal) could help to ensure that all areas ofthe disease are covered.www.badgut.org 5-Aminosalicylic Acid (5-ASA)5-ASA medication is safe and well tolerated forlong-term use in mild cases of ulcerative colitis.These medications, taken orally, include mesalamine(Asacol , Asacol 800 , Mesasal , Mezavant ,Pentasa , Salofalk ) and olsalazine sodium(Dipentum ). Quicker results might occur whenmedication is used in a topical form, taken rectally.Salofalk is available in 500mg and 1g suppositories.Salofalk 1g and Pentasa 1g suppositories areonce-a-day therapies. In a more difficult case, youmay receive 5-ASA enema therapy (Salofalk 4g& 2g/60mL and Pentasa 1g, 2g, or 4g/100mL)for a short course, followed by suppositories, asthe inflammation improves. Some patients maybenefit from a combination of orally and rectallyadministered 5-ASA therapies in cases that do notrespond to rectal therapy alone.Patients use rectal medications nightly at firstand, as the disease improves, treatments become lessfrequent. Sometimes your doctor will stop treatmentand start it again if there is a flare up, and sometimesmaintenance therapy two to three times a week maybe required long-term. Typically, a patient starts onone type of preparation and if there is inadequateresponse, then switches to another type.5-ASA helps to settle acute inflammation and,when taken on a long-term basis (maintenance),it tends to keep the inflammation inactive. It isimportant to keep up your medicine regimen evenif your symptoms disappear and you feel well again.Maintenance therapy can be at the full initial dosageor at a reduced dosage and interval, depending on thedisease response.CorticosteroidsTo reduce inflammation for the short-termin moderate to severe cases of ulcerative colitis,corticosteroids can help. These are prednisone andbudesonide (Entocort ) taken orally, althoughprednisone tends to have greater side effects. Thesemedications can be helpful to induce remission butshould not be used long-term, or for maintenance.For topical relief in the colon, budesonide(Entocort ) and hydrocortisone (Betnesol ,Cortenema , Cortifoam , Proctofoam ) areavailable for patients to administer rectally (enemas,foams, and suppositories). However, if the patientUlcerative Colitis GI Society 3
has significant diarrhea, then the rectal medicationsmay be difficult to hold. Cortifoam is a foampreparation of a smaller volume so the patient mayretain the treatment in the rectum longer, therebyincreasing the amount of time it has to work.Physicians can prescribe hydrocortisone (SoluCortef ) and methylprednisolone (Solu-Medrol )for administration intravenously in-hospital.Immunosuppressive AgentsThese drugs are used to treat ulcerativecolitis, to reduce dependence on steroids, and forthose who have steroid-resistant disease. Theyinclude azathioprine (Imuran ), cyclosporine,mercaptopurine/6-MP(Purinethol ),andmethotrexate sodium (Rheumatrex ). It could takeup to six months or more of therapy to see results.BiologicsBiologic medications are important treatmentoptions for those who have moderate to severeulcerative colitis. Biologics are specially developedantibodies, which selectively block moleculesthat are involved in the inflammatory process.Gastroenterologists routinely prescribe biologics,which include infliximab (Remicade ), golimumab(Simponi ), and adalimumab (Humira ) to controlthe symptoms(induce clinical remission) ofinflammatory bowel diseases.Remicade has indications to induce andmaintain clinical remission and mucosal healing, andfor reducing or eliminating corticosteroid use, since2006. Simponi has indications for use to induceand maintain clinical remission and mucosal healinguse, since 2013. Humira has indications for use toinduce and maintain clinical remission, since 2013.Both Humira and Simponi are selfadministered under the skin (subcutaneously),Humira about every 2 weeks, and Simponi about every 4 weeks. A health care professionaladministers Remicade by intravenous (IV)infusion about every 8 weeks, usually in a Janssenprovided BioAdvance clinic.SurgerySince ulcerative colitis only involves the largebowel, removing this organ will remove the diseasebut it is not a cure; removing the colon can leadto other symptoms and complications. Althoughthere are many variations to possible surgicalprocedures, typically, after removing all or part ofthe colon (colectomy), a surgeon brings the end of theremaining intestine through a new surgical openingin the abdominal wall (ostomy) to which the patientcan attach a removable appliance to collect stool.An ostomy may be either temporary or permanent,depending upon the particular situation.In recent years, new techniques have arisenwhereby surgeons can preserve the anal muscleand create an internal pouch, or reservoir, fromthe remaining intestine. Emptying pouch contentsvia the anus more closely resembles the normalanatomical route. However, with the loss of colonfunction, bowel movements have very high watercontent and move very frequently. This means thateven after surgery, patients could face troublesomegastrointestinal symptoms. One complication thatcan occur is pouchitis, which is inflammation withinthe surgically-created pouch.An emerging surgical therapy is intestinaltransplantation, but there are barriers yet toovercome, such as tissue rejection and inflammationin the newly transplanted organ.OutlookUlcerative colitis is a chronic, systemicinflammatory disease manifesting in the colon.Intensity of this condition varies greatly from personto person and during a lifetime. Some patients mayhave an initial episode and then go into remissionfor a long period, some may have occasional flareups, and some others may have ongoing disease.Although there is no cure, ulcerative colitis patientsrequire ongoing medical care, and must adhere to aproper nutrition and medication regimen, even whenthings appear to be going well. Your physician willwork with you to create an appropriate treatment planfor you and to monitor your disease regularly, evenduring periods of remission. For more informationon ulcerative colitis, visit www.badgut.org.In patients with ongoing active disease that failsto respond to all forms of medical management,surgery may be necessary.4GI Society Ulcerative Colitis www.badgut.org
Notes:About UsAs the Canadian leader in providing trusted, evidence-basedinformation on all areas of the gastrointestinal (GI) tract, theGastrointestinal Society is committed to improving the livesof people with GI and liver conditions, supporting research,advocating for appropriate patient access to healthcare, andpromoting gastrointestinal and liver health.The Inside Tract newsletter provides the latest newson GI research, disease and disorder treatments (e.g.,medications, nutrition), and a whole lot more. If you haveany kind of digestive problem, then you’ll want this timely,informative publication.Please subscribe today!The GI Society, in partnership with the Canadian Societyof Intestinal Research, produced this pamphlet under theguidance of affiliated healthcare professionals. This documentis not intended to replace the knowledge, diagnosis, or careof your physician. Gastrointestinal Society 2014Subscription/Donation FormPurchase InformationI enclose a donation of (Eligible for a tax receipt)I enclose a 20 annual subscription fee ( 30 outside Canada)Total Name (Mr./Mrs./Ms./Dr./OtherPlease circle one)Company Name (Optional)Street AddressCity, Province, Postal CodeDaytime PhonePatientEmailFriend/Family MemberProfessionalDiagnosis/Area of Interest (This optional information helps usto determine which topics might be of interest to you and is keptstrictly confidential. We never sell our lists.)Would you like more information? Please list your topics.Payment:VisaMastercardCheque Enclosed*Credit Card NumberExpiry Date*Make cheque payable to the GI Society.Gastrointestinal Society231-3665 KingswayVancouver, BC V5R 5W2Phone: 604-873-4876Toll-free: 1-866-600-4875Fax: 604-875-4429Email: info@badgut.orgWebsite: www.badgut.orgCharitable Registration Number: 817065352RR0001www.badgut.org Ulcerative Colitis GI Society 5
Ulcerative colitis is unrelated to ulcers found elsewhere in the gastrointestinal tract, such as stomach or duodenal ulcers, but it has many similarities to Crohn's disease, another IBD. The main differences between Crohn's disease and ulcerative colitis are that, in Crohn's disease, the inflammation extends into the bowel muscle wall and