Transcription
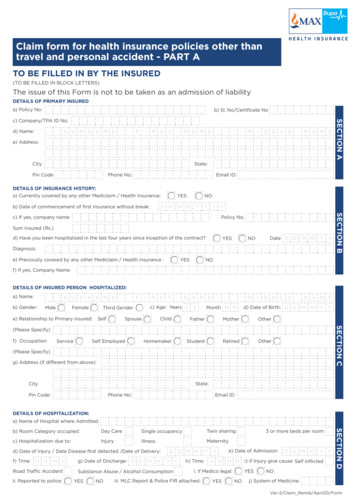
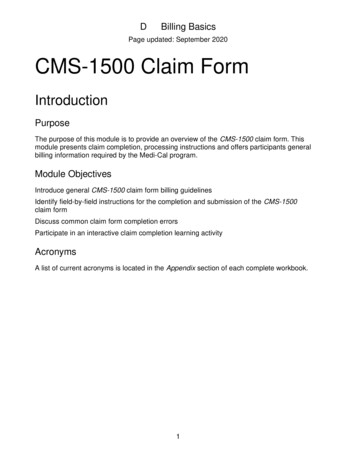
CLAIM FORM(The issue of this Form is not to be taken as an admission of liability)Claim FormPART ATO BE FILLED IN BY THE INSURED(TO BE FILLED IN BLOCK LETTERS)« Non-submission of original bills and receipts is the main reason for delay in claim settlements. Please provide the originalsDo You Know« Provide your bank details for direct/ Electronic Fund Transfer (EFT) for faster claim settlement. Refer Part A - Section G« To receive updates on your claim status, please provide your mobile no. & E-mail ID« You can check your claim status at: www.maxbupa.com à Claims à Claims status àLogin to check statusSECTIONA - DETAILS OF PRIMARY INSUREDa)Policy No. :b) Sl. No/ Certificate No. :c)Company/ TPA ID No :d)Name :e)Address :City :State :Pin Code :Phone No. :Email ID :SECTION B - DETAILS OF INSURANCE HISTORYa)Currently covered by any other mediclaim health insurance Yes / No b)Date of commencement of first Insurance for the person (without break) :c)If Yes, Company Name :Policy No. :d)YYYSum Insured :Have you been hospitalized in the last four years since inception of the contract? Yese)Diagnosis :f)D D M M Y(DD/MM/YYYY) : / No (DD/MM/YYYY) :D D M M YPreviously covered by any other Mediclaim/Health insurance YesYYY / No If Yes, Company Name :SECTION C - DETAILS OF THE INSURED PERSON HOSPITALISED :a)Name :b)Relationship : Selfc) Date of Birth :f) / Spouse / Child / Father / MotherD D M M YYYd)Y(Please Specify) : / Other Age (YY/MM) :YYM Me)Gender: Male / Female Address :City :State: :StatePin Code :Phone No. :g) Occupation : Service / Self employed / HomemakerEmail ID :(Please Specify) : / Student / Retired / OthersSECTION D - DETAILS OF HOSPITALISATION :a)Name of the Hospital where admitted :b)Room Category occupied : Day care / Single occupancyc)Hospitallisation due to Illnessd)Date of Injury/ Date of disease first detected/ Date of delivery :e)Date of admission : (DD/MM/YYYY) :D D M M Yg)Date of discharge : (DD/MM/YYYY) :D D M M Yi)If injury, give cause : Self Inflictedi)j)If Medico legal Yes / Twin sharing / 3 or more beds per room / Injury / Maternity : Details :D D M M YY Y YY Y Yf)Time : (HH/MM) :H H M MY Y Yh)Time : (HH/MM) :H H M M / Road Traffic Accident / Substance Abuse / Alcohol Consumption / No System of medicine : Allopathic(DD/MM/YYYY) :ii)Reported to police? Yes / Other systems of medicine / No iii) MLC Report, & Police FIR attached? Yes SECTION E - DETAILS OF CLAIM :a)Details of the treatment expenses claimed :i)Pre-hospitalisation ExpensesRs.ii)Hospitalisation ExpensesRs.iii)Post-hospitalisation ExpensesRs.iv)Health-Check up CostRs.1Please dispatch your claim document to: Max Bupa Corporate Office: Bloc B1/I-2, Mohan Cooperative Industrial Estate, Mathura Road, New Delhi -110044. / No
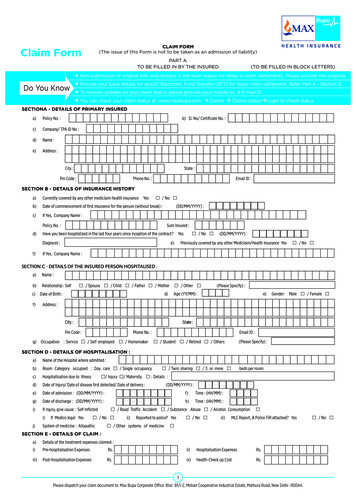
Claim Formv)Ambulance ChargesRs.TotalRs.vii) Pre-hospitalisation Periodvi)DaysOthers (code)Rs.viii) Post -hospitalisation Period / No Daysb)Claim for Domiciliary Hospitalization : Yes(if yes, please provide details in annexure)c)Details of Lumpsum / cash benefit claimed :i)Hospital Daily CashRs.ii)Surgical CashRs.iii)Critical IlIness BenefitRs.iv)ConvalescenceRs.v)Pre/Post hospitalisation lum psum benefit: Rs.vi)OthersRs.Claim Documents Submitted- CheckList: Duly filled and signed Claim Form Copy of intimation letter, if any Hospital Main Bill Hospital Break Up bill Hospital Bill Payment Receipt Hospital Discharge Summary Pharmacy Bill Operation Threater Notes ECG Doctor’s Request for Investigation Investigation Reports ( Including CT, MRI/USG/HPE) Doctor’s Prescription OthersSECTION - F DETAILS OF BILLS ENCLOSED :Sl. No.Bill No.DateIssued byTowardsDDMMYYHospital Main BillDDM MYYPre-hospitalisation Bills: NosDDM MYYPost-hospitalisation Bills: NosDDM MYYPharmacy BillsDDM MYYDDM MYYDDM MYYDDM MYYDDM MYYDDM MYYDDM MYYAmount (Rs.)SECTION - G DETAILS OF PRIMARY INSURED’S BANK ACCOUNT :a)Account Holder’s Name:b)PAN No :d)Bank Name :e)IFSC Code :f)Payment option: Cheque / DD / NEFT g)MICR No :c) Account No :Branch :Note: Please submit a cancelled cheque leaf or a copy of latest bank statement or passbook with a/c holder’s name, account no. and IFSC code mentioned on it.SECTION H - DECLARATION BY THE INSUREDI hereby declare that the information furnished in this claim form is true & correct to the best of my knowledge and belief. If I have made any false or untrue statement,suppression or concealment of any material fact with respect to questions asked in relation to this claim, my right to claim reimbursement shall be forfeited. I also consent& authorize TPA / insurance company, to seek necessary medical information / documents from any hospital / Medical Practitioner who has attended on the person againstwhom this claim is made. I hereby declare that I have included all the bills / receipts for the purpose of this claim & that I will not be making any supplementary claim exceptthe pre/post-hospitalisation claim, if any.Date :Place :D D M M YY Y YSignature of Insured :þ2Please dispatch your claim document to: Max Bupa Corporate Office: Bloc B1/I-2, Mohan Cooperative Industrial Estate, Mathura Road, New Delhi -110044.
Claim FormCHECK LIST OF ENCLOSURES FOR SUBMISSION OF CLAIMIn-patient Treatment /Day Care ProceduresDaily Cash Benefitq Duly filled and signed Claim Form.q Duly filled and signed Consent Form.q Photocopy of ID card / Photocopy of current year policy.q Duly filled and signed Claim Form.q Photocopy of ID card / Photocopy of current year policy.q Original Detailed Discharge Summary / Day care summary from thehospital.q Original consolidated hospital bill with break up of each Item, dulysigned by the insured.q Original payment Receipt of the hospital bill.q First Consultation letter and subsequent Prescriptions.Organ Donation/TransplantationIn addition to the documents of general hospitalisationq Organ Function test / blood test proving organ failure.q Treatment Certificate issued by the Transplant Surgeon of the hospitalconcerned.q Original bills, original payment receipts and Reports for investigation.q Original medicine bills and receipts with corresponding Prescriptions.q Original invoice/bills for Implants (viz. Stent /PHS Mesh / IOL etc.) withoriginal payment receipts.Ambulance Benefitq Duly filled and signed Claim Form.q Photocopy of ID card / Photocopy of current year policy.Road Traffic AccidentIn addition to the In-patient Treatment documents:q Copy of the First Information Report from Police Department / Copy ofthe Medico-Legal Certificate.In Non Medico legal casesq Original Bill with Original Payment Receipt.q Treating Doctor’s consultation prescription indicating EmergencyHospitalization.q Treating Doctor’s Certificate giving details of injuries (How, when andwhere injury sustained)Maternity ExpensesIn Accidental Death casesq Copy of Post Mortem Report & Death CertificateIn addition to the In-patient Treatment documents:q Obstetric history (Gravida, Para, Living children, Abortions) fromtreating doctor.For Death CasesIn addition to the In-patient Treatment documents:q Original Death Summary from the hospital.Critical Illness Benefitq Copy of the Death certificate from treating doctor or the hospitalauthority.q Photocopy of ID card / Photocopy of current year policy.q Copy of the Legal heir certificate, if the claim is for the death of theprinciple insured.q A medical certificate confirming the diagnosis of critical illness from adoctor not less qualified than MD/MS.q Duly filled and signed Claim Form.q Investigation reports / other related documents reflecting the criticalillness diagnosis.Pre and Post-hospitalisation expensesq Duly filled and signed Claim Form.q Photocopy of ID card / Photocopy of current year policy.q Original Medicine bills, original payment receipt with prescriptions.q Original Investigations bills, original payment receipt with prescriptionsand report.q Original Consultation bills, original payment receipt with prescription.Health Check upq Duly filled and signed Claim Form.q Photocopy of ID card / Photocopy of current year policy.q Original Investigation bills, original payment receipts with Reports.q Original Consultation bills and original payment receipts with prescription.q Copy of the Discharge Summary of the main claim.Outpatient Benefit/Dentalq Duly filled and signed Claim Form.q Photocopy of ID card / Photocopy of current year policy.q Original Medicine bills, original payment receipt.Expenses for spectacles/contact lenses, hearing aidsq Duly filled and signed Claim Form.q Photocopy of ID card / Photocopy of current year policy.q Original Investigations bills, original payment receipt with report.q Original Consultation bills, original payment receipt with prescription.q Details of any Outpatient Procedures, If anyq Dental X-ray film.q Prescription of the Treating Doctor.q Original Invoice/bills, original payment receipt of the device, appliances, lens etc.3Please dispatch your claim document to: Max Bupa Corporate Office: Bloc B1/I-2, Mohan Cooperative Industrial Estate, Mathura Road, New Delhi -110044.
GUIDANCE FOR FILLING CLAIM FORM - PART A :DATA ELEMENTDESCRIPTIONFORMATa) Policy No.Enter the policy numberAs allotted by the insurance companyb) SI. No/ Certificate No.Enter the social insurance number or the Certificate number of socialhealth insurance schemeAs allotted by the organizationc) Company TPA ID No.Enter the TPA ID NoLicense number as allotted by IRDA andprinted in TPA documentsd) NameEnter the full name of the policyholderSurname, First name, Middle namee) AddressEnter the full postal addressInclude Street, City and Pin Codea) Currently covered by any otherMediclaim / Health Insurance?Indicate whether currently covered by another Mediclaim / HealthInsuranceTick Yes or Nob) Date of Commencement of firstInsurance without breakEnter the date of commencement of first insuranceUse dd-mm-yy formatc) Company NameSECTION A - DETAILS OF PRIMARY INSUREDSECTION B - DETAILS OF INSURANCE HISTORYEnter the full name of the insurance companyName of the organization in fullPolicy No.Enter the policy numberAs allotted by the insurance companySum InsuredEnter the total sum insured as per the policyIn rupeesIndicate whether hospitalized in the last 4 yearsTick Yes or NoDateEnter the date of hospitalisationUse mm-yy formatDiagnosisEnter the diagnosis detailsOpen Texte) Previously Covered by any otherMediclaim/ Health Insurance?Indicate whether previously covered by another Mediclaim / HealthInsuranceTick Yes or Nof) Company NameEnter the full name of the insurance companyName of the organization in fulld) Have you been Hospitalized in thelast 4 yearsSECTION C - DETAILS OF INSURED PERSON HOSPITALIZEDa) NameEnter the full name of the patientSurname, First name, Middle nameb) Relationship to primary InsuredIndicate relationship of patient with policyholderTick the right option. If others, please specifyc) Date of BirthEnter Date of Birth of patientUse dd-mm-yy formatd) AgeEnter age of the patientNumber of years and monthse) AddressEnter the full postal addressInclude Street, City and Pin Codef) GenderIndicate Gender of the patientTick Male or Femaleg) OccupationIndicate occupation of patientTick the right option. If others, please specifyh) Phone NoEnter the phone number of patientInclude STD code with telephonei) E-mail IDEnter e-mail address of patientComplete e-mail addressa) Name of Hospital where admittedEnter the name of hospitalName of hospital in fullb) Room category occupiedIndicate the room category occupiedTick the right optionc) Hospitalization due toIndicate reason of hospitalisationTick the right optiond) Date of Injury/Date Disease firstdetected/ Date of DeliveryEnter the relevant dateUse dd-mm-yy formate) Date of admissionEnter date of admissionUse dd-mm-yy formatf) TimeEnter time of admissionUse hh:mm formatg) Date of dischargeEnter date of dischargeUse dd-mm-yy formath) TimeEnter time of dischargeUse hh:mm formati) If Injury give causeIndicate cause of injuryTick the right optionIf Medico legalIndicate whether injury is medico legalTick Yes or NoReported to PoliceIndicate whether police report wasfiledTick Yes or NoMLC Report & Police FIR attachedIndicate whether MLC report and Police FIR attachedTick Yes or NoEnter the system of medicine followed in treating the patientOpen TextSECTION D - DETAILS OF HOSPITALIZATIONj) System of Medicine4Please dispatch your claim document to: Max Bupa Corporate Office: Bloc B1/I-2, Mohan Cooperative Industrial Estate, Mathura Road, New Delhi -110044.
SECTION E - DETAILS OF CLAIMa) Details of Treatment ExpensesEnter the amount claimed as treatment expensesIn rupees (Do not enter paise values)b) Claim for DomiciliaryHospitalizationIndicate whether claim is for domiciliary hospitalisationTick Yes or Noc) Details of Lump sum/ cash benefitclaimedEnter the amount claimed as lump sum/ cash benefitIn rupees (Do not enter paise values)d) Claim Documents SubmittedCheck ListIndicate which supporting documents are submittedTick the right optionSECTION F - DETAILS OF BILLS ENCLOSEDIndicate which bills are enclosed with the amounts in rupeesSECTION G - DETAILS OF PRIMARY INSURED’S BANK ACCOUNTAs mentioned in the bank documentsEnter the full namea) Account Holder’s Nameb) PANEnter the permanent account numberAs allotted by the Income Taxc) Account NumberEnter the bank account numberAs allotted by the bankd) Bank Name and BranchEnter the bank name along with the branchName of the Bank in fulle) IFSC Codef) Cheque/ DD payable detailsEnter the IFSC code of the bank branchEnter the name of the beneficiary the cheque/DD should be made out toIFSC code of the bank branch in fullName of the individual/ organization in fullSECTION H - DECLARATION BY THE INSUREDRead declaration carefully and mention date (in dd:mm:yy format), place (open text) and sign.PART B(TO BE FILLED IN BY THE HOSPITAL IN CASE OF CASHLESS CLAIMS)The issue of this Form is not to be taken as an admission of liability. Please inclu
Please dispatch your claim document to: Max Bupa Corporate Office: Bloc B1/I-2, Mohan Cooperative Industrial Estate, Mathura Road, New Delhi -110044. v) Ambulance Charges Rs. vi) Others (code) Rs. Total Rs. Claim Form vii) Pre-hospitalisation Period Days viii) Post -hospitalisation Period Days b) Claim for Domiciliary Hospitalization : Yes / No (if yes, please provide details in annexure .