Transcription
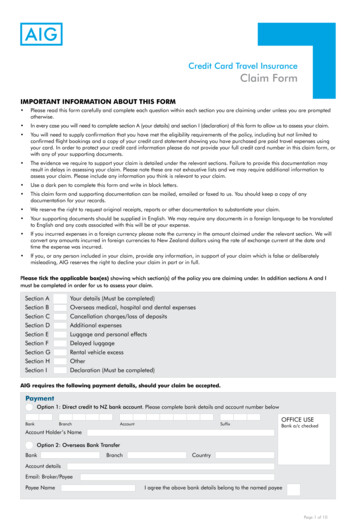
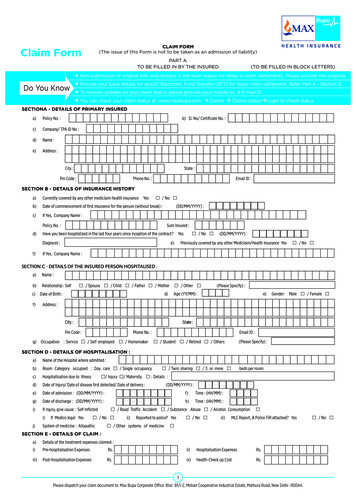
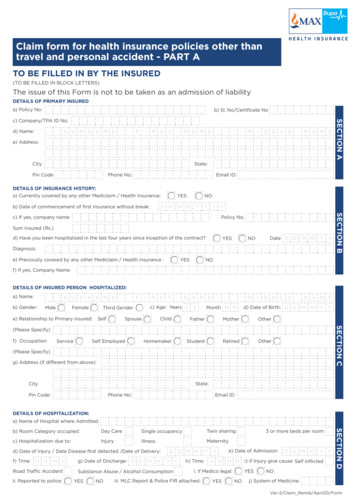
Claim form for health insurance policies other thantravel and personal accident - PART ATO BE FILLED IN BY THE INSURED(TO BE FILLED IN BLOCK LETTERS)The issue of this Form is not to be taken as an admission of liabilityDETAILS OF PRIMARY INSUREDa) Policy No:b) Sl. No/Certificate Nod) Name:SU R N A M EFIRSTMN A M EID D LEN A M Ee) Address:SECTION Ac) Company/TPA ID No:State:CityPin CodePhone No:Email ID:DETAILS OF INSURANCE HISTORY:a) Currently covered by any other Mediclaim / Health Insurance:YESD Db) Date of commencement of first Insurance without break:NOM MY Y Y YSum Insured (Rs.)d) Have you been hospitalized in the last four years since inception of the contract?YESDate D DNOM MY YDiagnosis:e) Previously covered by any other Mediclaim / Health insurance :YESSECTION BPolicy No.c) If yes, company name:NOf) If yes, Company NameDETAILS OF INSURED PERSON HOSPITALIZED:a) Name:Sb) Gender:MaleU R N A M EFIe) Relationship to Primary insured:SpouseSelfSTMN A M Ec) Age: Years Y YThird GenderFemaleRMonth M MID D LEd) Date of Birth: D DFatherMotherOtherHomemakerStudentRetiredOtherM MY YSECTION CChildN A M E(Please Specify)f) Occupation:ServiceSelf Employed(Please Specify)g) Address (if different from above):State:CityPin Code:Phone No:Email ID:DETAILS OF HOSPITALIZATION:a) Name of Hospital where Admitted:Day CareSingle occupancyTwin sharingc) Hospitalization due to:InjuryIllnessMaternityd) Date of Injury / Date Disease first detected /Date of Delivery:f) Time:H HM MRoad Traffic Accidentii. Reported to police:g) Date of Discharge: D DM MD DY YSubstance Abuse / Alcohol ConsumptionYESNOM Mh) Time:Y YH He) Date of Admission:M MYESNOD DM MY Yi) If Injury give cause: Self inflictedYESi. If Medico legal:iii. MLC Report & Police FIR attached:3 or more beds per roomNOSECTION Db) Room Category occupied:j) System of Medicine:Ver-2/Claim Reimb/April20/Form
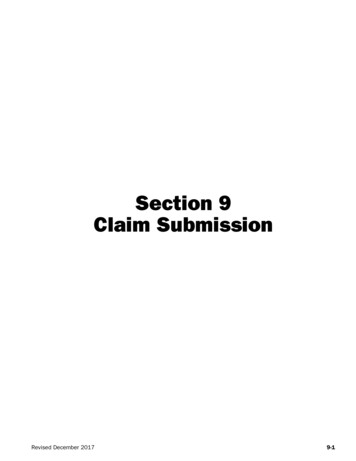
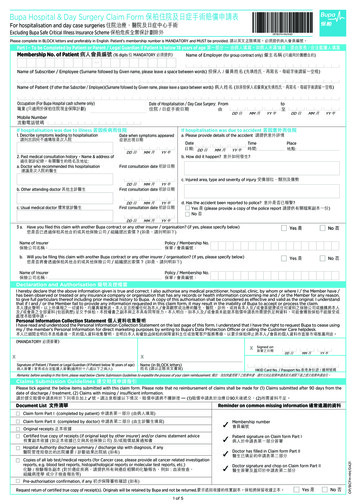
DETAILS OF CLAIM:a) Details of the treatment expenses claimedi. Pre-hospitalization Expenses:Rs.ii. Hospitalization Expenses: Rs.iii. Post-hospitalization Expenses:Rs.iv. Health-Check up Cost:Rs.v. Ambulance Charges:Rs.vi. Others (code):Rs.TotalRs.Daysvii. Pre-hospitalization period:YESDaysNO (If yes, provide details in annexure)SECTION Eb) Claim for Domiciliary Hospitalization:viii. Post-hospitalization period:c) Details of Lump sum / cash benefit claimed:i. Hospital Daily Cash:Rs.ii. Surgical Cash:Rs.iii. Critical Illness Benefit:Rs.iv. Convalescence:Rs.vi. OthersRs.TotalRs.v. Pre/Post hospitalization Lump sum benefit: Rs.Claim Documents Submitted- Check List:Claim Form Duly signedHospital Discharge SummaryInvestigation Reports (Including CT/MRI / USG / HPE)Copy of the Claim intimation if anyPharmacy BillHospital Main BillOperation Theatre NotesDoctor's PrescriptionsHospital Break-up BillECGOthersHospital Bill Payment ReceiptDoctor's request for investigationDETAILS OF BILLS ENCLOSED:Sl. No.DateBill No.Issued byAmount (Rs)TowardsD D M M Y YHospital Main BillD D M M Y YPre-hospitalization Bills:Nos3D D M M Y YPost-hospitalization Bills:Nos4D D M M Y YPharmacy Bills5D D M M Y Y6D D M M Y Y7D D M M Y Y8D D M M Y Y9D D M M Y Y10D D M M Y Yb) Account Number:a) PANc) Bank Name and Branch:e) IFSC Code:d) Cheque/ DD Payable details:DateD DM MY YPlaceSignature of the InsuredSECTION HDECLARATION BY THE INSURED:I hereby declare that the information furnished in this claim form is true & correct to the best of my knowledge and belief. If I have made anyfalse or untrue statement, suppression or concealment of any material fact with respect to questions asked in relation to this claim, my rightto claim reimbursement shall be forfeited. I also consent & authorize TPA / insurance company, to seek necessary medical information /documents from any hospital / Medical Practitioner who has attended on the person against whom this claim is made. I hereby declare thatI have included all the bills / receipts for the purpose of this claim & that I will not be making any supplementary claim except the pre/posthospitalization claim, if any.SECTION GDETAILS OF PRIMARY INSURED'S BANK ACCOUNT:SECTION F12
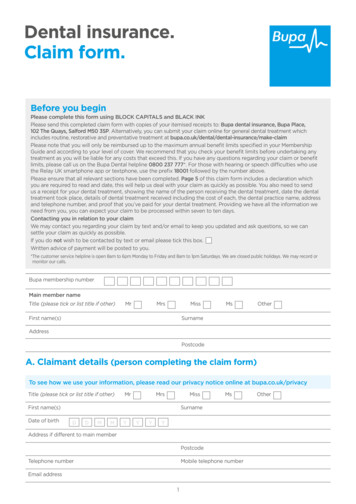
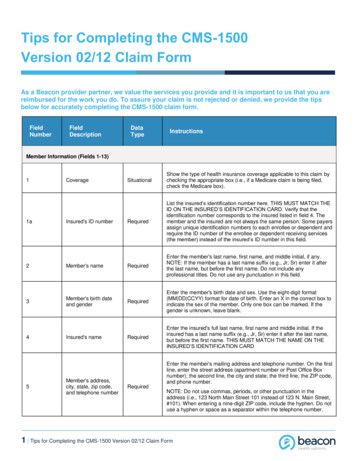
GUIDANCE FOR FILLING CLAIM FORM - PART A(To be filled in by the insured)DESCRIPTIONDATA ELEMENTFORMATSECTION A - DETAILS OF PRIMARY INSUREDa)Policy No.Enter the policy numberAs allotted by the insurance companyb)SI. No/ Certificate No.Enter the social insurance number or thecertificate number of social health insuranceschemeAs allotted by the organizationc)Company TPA ID No.Enter the TPA ID NoLicense number as allotted by IRDAIand printed in TPA documents.d)NameEnter the full name of the policyholderSurname, First name, Middle namee)AddressEnter the full postal addressInclude Street, City and Pin CodeSECTION B - DETAILS OF INSURANCE HISTORYa)Currently covered by any otherMediclaim / Health Insurance?Indicate whether currently covered by anotherMediclaim / Health InsuranceTick Yes or Nob)Date of Commencement of firstInsurance without breakEnter the date of commencement of firstinsuranceUse dd-mm-yy formatc)Company NameEnter the full name of the insurance companyName of the organization in fullPolicy No.Enter the policy numberAs allotted by the insurance companySum InsuredEnter the total sum insured as per the policyIn rupeesHave you been Hospitalized inthe last four years sinceinception of the contract?Indicate whether hospitalized in the last fouryearsTick Yes or NoDateEnter the date of hospitalizationUse mm-yy formatDiagnosisEnter the diagnosis detailsOpen Texte)Previously Covered by any otherMediclaim/ Health Insurance?Indicate whether previously covered byanother Mediclaim / Health InsuranceTick Yes or Nof)Company NameEnter the full name of the insurance companyName of the organization in fulld)SECTION C - DETAILS OF INSURED PERSON HOSPITALIZEDa)NameEnter the full name of the patientSurname, First name, Middle nameb)GenderIndicate Gender of the patientTick Male, Female or Third Genderc)AgeEnter age of the patientNumber of years and monthsd)Date of BirthEnter Date of Birth of patientUse dd-mm-yy formate)Relationship to primary InsuredIndicate relationship of patient withpolicyholderTick the right option. If others, please specify.f)OccupationIndicate occupation of patientTick the right option. If others, please specify.g)AddressEnter the full postal addressInclude Street, City and Pin Codeh)Phone NoEnter the phone number of patientInclude STD code with telephone numberi)E-mail IDEnter e-mail address of patientComplete e-mail address
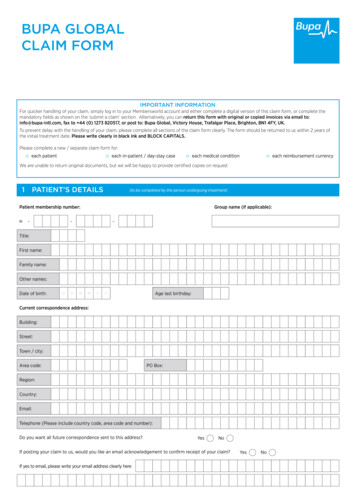
SECTION D - DETAILS OF HOSPITALIZATIONa) Name of Hospital where admittedEnter the name of hospitalName of hospital in fullb) Room category occupiedIndicate the room category occupiedTick the right optionc) Hospitalization due toIndicate reason of hospitalizationTick the right optiond) Date of Injury/Date Disease firstdetected/ Date of DeliveryEnter the relevant dateUse dd-mm-yy formate) Date of admissionEnter date of admissionUse dd-mm-yy formatf) TimeEnter time of admissionUse hh:mm formatg) Date of dischargeEnter date of dischargeUse dd-mm-yy formath) TimeEnter time of dischargeUse hh:mm formatIndicate cause of injuryTick the right optionIf Medico legalIndicate whether injury is medico legalTick Yes or NoReported to PoliceIndicate whether police report was filedTick Yes or NoMLC Report & Police FIR attachedIndicate whether MLC report and Police FIRattachedTick Yes or NoEnter the system of medicine followed intreating the patientOpen Texti) If Injury give causej)System of MedicineSECTION E - DETAILS OF CLAIMa)Details of Treatment ExpensesEnter the amount claimed as treatmentexpensesIn rupees (Do not enter paise values)b)Claim for DomiciliaryHospitalizationIndicate whether claim is for domiciliaryhospitalizationTick Yes or Noc)Details of Lump sum/ cashbenefit claimedEnter the amount claimed as lump sum/cash benefitIn rupees (Do not enter paise values)d)Claim Documents SubmittedCheck ListIndicate which supporting documents aresubmittedTick the right optionSECTION F - DETAILS OF BILLS ENCLOSEDIndicate which bills are enclosed with the amounts in rupeesSECTION G - DETAILS OF PRIMARY INSURED'S BANK ACCOUNTa)PANEnter the permanent account numberAs allotted by the Income Tax departmentb)Account NumberEnter the bank account numberAs allotted by the bankc)Bank Name and BranchEnter the bank name along with the branchName of the Bank in fulld)Cheque/ DD payable detailsEnter the name of the beneficiary the cheque/DD should be made out toName of the individual/ organization in fulle)IFSC CodeEnter the IFSC code of the bank branchIFSC code of the bank branch in fullSECTION H - DECLARATION BY THE INSUREDRead declaration carefully and mention date (in dd:mm:yy format), place (open text) and sign.Disclaimer: Max Bupa Health Insurance Company Limited, Registered Office: B-1/I-2, Mohan Cooperative Industrial Estate, MathuraRoad, New Delhi – 110044. Website: www.maxbupa. com, Fax: 011-30902010, Customer Helpline No.: 1860 500 8888. CIN:U66000DL2008PLC182918, IRDAI Registration No. 145. ‘Max’, Max logo, ‘Bupa’ and Heartbeat logo are registered trademarks of theirrespective owners and are being used by Max Bupa Health Insurance Company Limited under license. Insurance is the subject matter ofsolicitation. Please read sales brochure carefully before concluding a sale.
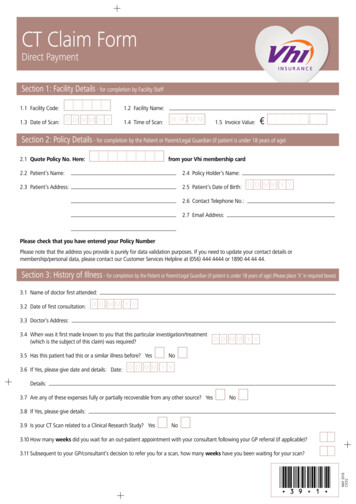
CLAIM FORM - PART BTO BE FILLED IN BY THE HOSPITAL(TO BE FILLED IN BLOCK LETTERS)The issue of this Form is not to be taken as an admission of liabilityPlease include the original preauthorization request form in lieu of PART ADETAILS OF HOSPITALb) Hospital ID:c) Type of Hospital:d) Name of the treating doctor:U R N A M ESFIRSTNetwork(If non networkfill section E)Non NetworkN A M EMID D LEN A M Ef) Registration No. with State Code:e) Qualification:SECTION Aa) Name of the hospital:g) Phone No.DETAILS OF THE PATIENT ADMITTEDa) Name of the Patient:SU R N A M EFIRSb) IP Registration Number:N A M Ec) Gender:f) Date of Admission:D DM Mi) Time:H HM MY Y Y Yg) Time: H HMaleD DM MY Y Y YDischarge to homeID D LEN A M EThird GenderFemaleM MY Y Y Y2 1 M 0M 1Y Y8 Y 3Yh) Date of Discharge: D DM Mj) Type of Admission: Emergencyk) If Maternity i. Date of Delivery: D Dl) Status at time of discharge:e) Date of birth:Months M MMDay CarePlannedMaternityii. Gravida Status:Discharge to another hospitalSECTION BY Yd) Age: YearsTDeceasedm)Total claimed amountDETAILS OF AILMENT DIAGNOSED (PRIMARY)a)ICD 10 CodesDescriptionICD 10 PCSb)i. Procedure 1:ii. AdditionalDiagnosis:ii. Procedure 2:iii. Co-morbidities:iii. Procedure 3:iv. Co-morbidities:iv. Details ofProcedure:c) Pre-authorization obtained:YESDescriptionSECTION Ci. PrimaryDiagnosis:d) Pre-authorization Number:NOe) If authorization by network hospital not obtained, give reason:f) Hospitalization due to Injury:YESNOI. If Yes, give cause Self-inflictedRoad Traffic AccidentSubstance abuse / alcohol consumptionii. If Injury due to Substance abuse / alcohol consumption, Test Conducted to establish this:iii. If Medico legal:YESNOvi. If not reported to police give reason:iv. Reported to Police:YESNOYESv. FIR no.NO(If Yes, attach reports)
CLAIM DOCUMENTS SUBMITTED - CHECK LISTInvestigation reportsOriginal Pre-authorization requestCT/MR/USG/HPE investigation reportsCopy of the Pre-authorization approval letterDoctor's reference slip for investigationCopy of photo ID card of patient verified by hospitalECGHospital Discharge summaryPharmacy billsOperation Theatre notesMLC report & Police FIRHospital main billOriginal death summary from hospital whereapplicableHospital break-up billAny other, please specifyADDITIONAL DETAILS IN CASE OF NON NETWORK HOSPITALSECTION DClaim Form duly signed(ONLY FILL IN CASE OF NON-NETWORK HOSPITAL)a) Address of the Hospital:Pin Code:d) Hospital PAN:b) Phone No:c) Registration No. with State Code:f) Facilities available in the hospital:e) Number of Inpatient bedsi. OT :YESNOii. ICU :YESSECTION EState:CityNOiii. Others :Date:Place:D D M M Y Y Y YSignature and Seal of the Hospital Authority:SECTION F(PLEASE READ VERY CAREFULLY)DECLARATION BY THE HOSPITALWe hereby declare that the information furnished in this Claim Form is true & correct to the best of our knowledge and belief. If we havemade any false or untrue statement, suppression or concealment of any material fact, our right to claim under this claim shall be forfeited.
GUIDANCE FOR FILLING CLAIM FORM - PART B(To be filled in by the hospital)DESCRIPTIONDATA ELEMENTFORMATSECTION A - DETAILS OF HOSPITALa)Name of HospitalEnter the name of hospitalName of hospital in fullb)Hospital IDEnter ID number of hospitalAs allocated by the TPAc)Type of HospitalIndicate whether In network or non networkhospitalTick the right optiond)Name of treating doctorEnter the name of the treating doctorName of doctor in fulle)QualificationEnter the qualifications of the treating doctorAbbreviations of educational qualificationsf)Registration No. with State CodeEnter the registration number of the doctoralong with the state codeAs allocated by the Medical Council of Indiag)Phone No.Enter the phone number of doctorInclude STD code with telephone numberSECTION B - DETAILS OF THE PATIENT ADMITTEDa)Name of PatientEnter the name of hospitalName of hospital in fullb)IP Registration NumberEnter insurance provider registration numberAs allotted by the insurance providerc)GenderIndicate Gender of the patientTick Male, Female or Third Genderd)AgeEnter age of the patientNumber of years and monthse)Date of BirthEnter date of admissionUse dd-mm-yy formatf)Date of AdmissionEnter date of admissionUse dd-mm-yy formatg)TimeEnter time of admissionUse hh:mm formath)Date of DischargeEnter date of dischargeUse dd-mm-yy formatI)TimeEnter time of dischargeUse hh:mm formatj)Type of AdmissionIndicate type of admission of patientTick the right optionk)If MaternityDate of DeliveryEnter Date of Delivery if maternityUse dd-mm-yy formatGravida StatusEnter Gravida status if maternityUse standard formatl)Status at time of dischargeIndicate status of patient at time of dischargeTick
I hereby declare that the information furnished in this claim form is true & correct to the best of my knowledge and belief. If I have made any false or untrue statement, suppression or concealment of any material fact with respect to questions asked in relation to this claim, my right to claim reimbursement shall be forfeited. I also consent & authorize TPA / insurance company, to seek .