Transcription
Inter-observer Agreement of FDG PET/CT visualHerder Score for the assessment of solitarypulmonary nodules (SPN)K Ordidge, N Gandy, M Arshad, N Soneji, K Wallitt, S Khan, T BarwickDepartment of Nuclear Medicine, Charing Cross Hospital, Imperial College HealthcareNHS Trust, London, UK
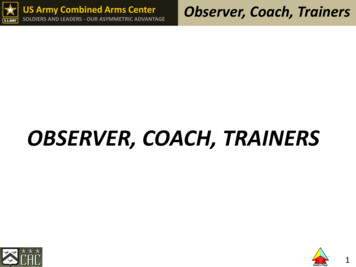
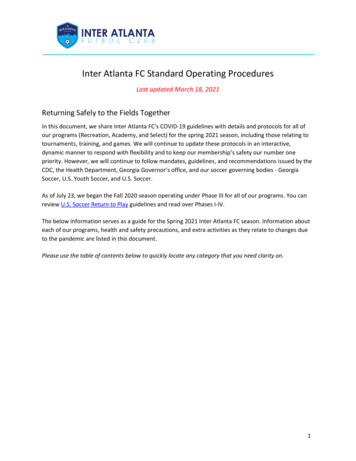
Background: Herder Visual Score for Solitary PulmonaryNodulesIntense ModerateFaintAbsentBritish Thoracic Society (BTS) guidelines recommend FDG PET CT for pulmonary nodule followup in high risk individuals or if the Brock score is 10% [1]Herder score was originally proposed by Herder et al. in 2005 in a retrospective study of 106patients with indeterminate solitary pulmonary nodules evaluated by FDG PET CT [2]Uptake in the nodule is assessed visually, in comparison to the surrounding lung tissue andmediastinal blood poolReferences:1. Callister MEJ, Baldwin DR, Akram AR, et al. British Thoracic Society guidelines for the investigation and management of pulmonary nodules. Thorax 2015;70: ii1–ii54.2. Herder GJ, van Tinteren H, Golding RP, et al. Clinical prediction model to characterize pulmonary nodules: validation and added value of 18F-fluorodeoxyglucose positron emission tomography. Chest 2005;128:2490–6
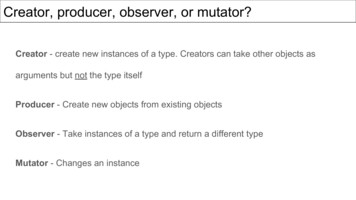
BTS Pulmonary Nodule Risk Prediction Calculator Herder score from the FDG PET CT is used to calculate the probability ofmalignancy, also taking into account other patient demographics- age,smoking history etc.Herder model probability is used to guide patient management
BTS Pulmonary Nodule Risk Prediction Calculator Differences in image interpretation using the visual scale will affect the Herder modelrisk prediction calculationThis could potentially lead to changes in patient managementReference:Callister MEJ, Baldwin DR, Akram AR, et al. British Thoracic Society guidelines for the investigation and management of pulmonary nodules. Thorax 2015;70: ii1–ii54.
Aim- Assessing Inter-observer Agreement Herder score has been reported as having high diagnostic validityVisual scale and needs to be reproducible between observersNo studies to date looking at inter-observer agreement in using the HerderscoreHigh inter-observer agreement has been reported using the Deauvillecriteria in lymphoma [1,2,3]References:1.2.3.Barrington SF, Qian W, Somer EJ et al. Concordance between four European centres of PET reporting criteria designed for use in multicentre trials in Hodgkinlymphoma. Eur J Nucl Med Mol Imaging (2010) 37:1824-1833Biggi A, Gallamini A, Chauvie S et al. International Validation Study for Interim PET in ABVD-Treated, Advanced-Stage Hodgkin Lymphoma: Interpretation Criteria andConcordance Rate Among Reviewers. J Nucl Med. 2013 May; 54(5):683-690Burggraaff CN, Comelisse AC, Hoekstra OS, et al. Interobserver Agreement of Interim and End-of-Treatment 18F-FDG PET/CT in Diffuse Large B-Cell Lymphoma:Impact on Clinical Practice and Trials. J Nucl Med. 2018 Dec;59(12):1831-1836
Methods Single centre retrospective study with local ethical approvalImperial FDG PET CT database was searched under IC10 code IC34 JF(lung, characterisation)Identified 100 consecutive patients having FDG PET CT for the evaluationof a solitary pulmonary noduleExclusion criteria: documented malignancy in the past 5 yearsAnonymised images were reviewed separately by 3 consultant NuclearMedicine Radiologists using a dedicated Hermes workstationHerder score was recorded, along with a confidence score graded 1-3Inter-observer agreement was assessed using Interclass CorrelationCoefficient modelling
Results- inter-observer agreement Complete reviewer agreement in 81% of casesInterclass correlation with Cronbach’s Alpha was excellent at 0.963 (95%CI 0.932-0.982) for the first 29 cases reviewedThe agreement between pairs of reviewers was good (Kappa scores forreviewer 1v2 0.722, 1v3 0.807, 2v3 0.625)For the remainder of the cases Cronbach’s Alpha was 0.977 (95% CI0.966-0.985)Kappa scores for reviewers 1v2 0.782, 1v3 0.901, 2v3 0.801This suggests that with increasing case numbers, the inter-observeragreement improvedOverall, for the total cases assessed, Cronbach’s Alpha was 0.973
Results- 19 discrepant cases 8 patients Herder risk calculations meant unchanged management planClinically significant difference in risk resulting in different managementplans in 11 patients- these patients were followed up 6 cases absent/faint discrepancy7 cases faint/moderate6 cases moderate/intense
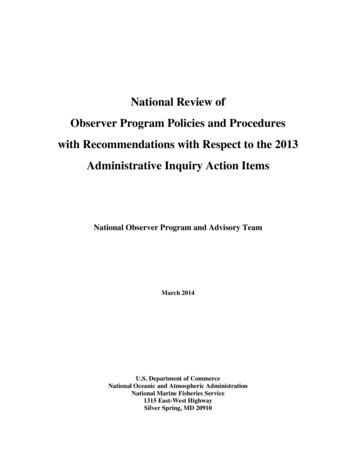
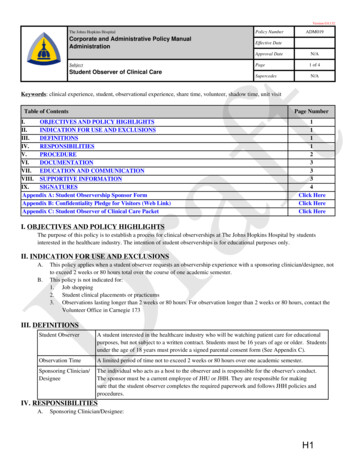
Discrepant case example- faint vs moderate
Follow up Patient too frail for lung biopsyIn practice this case was followedup with interval CT studies at 3/12and 12/12Stable volumetryIn most of the discrepancy cases,there was additional patienthistory that decided themanagement plan in the MDTsetting
Conclusion Inter- observer agreement is excellent, with 81% complete agreement andCronbach’s Alpha of 0.973Inter-observer agreement improved with increasing number of casesreviewedDifferences in visual interpretation can lead to clinically significantdifference in the calculated risk, changing the suggested managementIn practice, the clinical history is used to guide management, particularly incases where there is a previous history of cancerEquivocal cases were most likely to be followed up with interval CT at 3/12and 12/12
Further work Could inter-observer agreement improve further using a semi-quantitativemethod to assess lesion SUVmax and mediastinal blood pool SUVmax?Multiple studies using FDG PET & FDG PET CT suggest that semiquantitative methods do not increase accuracy of diagnosis [1,2], even forlesions with low SUVmax [3]ultraHD, Q.Clear- potential that things which were absent become faint onnewer reconstruction methods- affect on inter-observer agreement?References:1. Nomori et al. Visual and semiquantitative analyses for f-18 fluorodeoxyglucose in PET scanning in pulmonary nodules 1cm to 3cm in size. Ann Thorac Surg.2005 Mar;79(3):984-82. Garcia-Velloso et al. Assessment of indeterminate pulmonary nodules detected at lung cancer screening: Diagnostic accuracy of FDG PET/CT. Lung Cancer.2016 Jul;97:81-63. Hashimoto et al. Accuracy of PET for Diagnosis of Solid Pulmonary Lesions with 18F-FDG Uptake Below the Standardised Uptake Value of 2.5. J Nucl Med.2006; 47:426-431
Thank youSupervisor: Dr Tara BarwickConsultant reviewers: Dr Neil Soneji, Dr Sam Khan, Dr Kathryn WallittColleagues from Nuclear Medicine Department at Charing Cross Hospital
Kappa scores for reviewers 1v2 0.782, 1v3 0.901, 2v3 0.801 This suggests that with increasing case numbers, the inter-observer agreement improved . Discrepant case example- faint vs moderate. Follow up Patient too frail for lung biopsy In practice this case was followed up with interval CT studies at 3/12 and 12/12
![Clinical significance of incidental [18 F]FDG uptake in the .](/img/32/s12876-016-0545-x.jpg)