Transcription
COMMUNITY ALCOHOL WITHDRAWALPRESCRIBING GUIDELINESMARCH 2020This policy supersedes all previous policies for medically assisted community alcohol withdrawal
Policy titleCommunity alcohol withdrawal prescribing guidelinesPolicyreferencePolicy categoryPHA28Relevant toTrust-wide – any services conducting medically assisted community alcoholwithdrawalMar 2020Date publishedClinicalImplementationdateDate lastreviewedNext reviewdatePolicy leadMar 2020Contact detailsEmail:Telephone: 0203 317 6029bhaskar.punukollu@candi.nhs.ukVincent Kirchner, Medical DirectorAccountabledirectorAug 2019Mar 2023Bhaskar Punukollu, Consultant in Addiction PsychiatryApproved by(Group):Substance misuse consultants meetingApproved by(Committee):Drugs and Therapeutics CommitteeDocumenthistoryMembership ofthe policydevelopment/review teamConsultationDateVersionSummary of amendments20.11.091Original document22.07.152Original revised with minor amendmentsAug 20183No changesMar 20204Removal of vitamin B compound strong .Dr Bhaskar PunukolluSubstance misuse consultants groupMembers of drugs and therapeutics committeeDO NOT AMEND THIS DOCUMENTFurther copies of this document can be found on the Foundation Trust intranet.Community Alcohol Withdrawal Prescribing Guidelines: PHA28: Mar 2020
ContentsPage1Introduction12Aims and objectives13Scope of the policy24Assessing suitability for community alcohol withdrawal25Information to be obtained prior to commencement of withdrawal36Procedure for medically assisted withdrawal4-57Medication interventions following successful withdrawal6-78Dissemination and implementation arrangements79Training requirements710Monitoring and audit arrangements811Review of the policy812References813Associated documents:Appendix 1: Contract and consent form for medically assistedcommunity alcohol withdrawal9Appendix 2: Information sheet for clients on withdrawal process10-11Appendix 3: Severity of Alcohol Dependence Questionnaire (SADQ)12-13Appendix 4: Clinical Institute Withdrawal Assessment (CIWA-AR)14-15Appendix 5: Preparing for medically assisted community alcoholwithdrawal (client information sheet)Appendix 6: Pre-withdrawal checklist (key worker to complete)Appendix 7: Template letter to GP to request blood results and physicalexamination findingsCommunity Alcohol Withdrawal Prescribing Guidelines: PHA28: Mar 20201617-1819
1.Introduction1.1 Medically assisted community alcohol withdrawal is a process in which anindividual’s physical and mental health are monitored whilst being providedmedications and psychosocial support to relieve physical and psychologicalwithdrawal symptoms, on cessation of the use of alcohol.1.2 When undertaking assisted withdrawal, the patient is required to stop alcoholintake abruptly, and its effects are replaced by medication that has crosstolerance. Then medication can be reduced at a rate that prevents withdrawalsymptoms but without promoting over-sedation, and ultimately stoppedaltogether. The process involves providing a large enough initial dose to preventsevere withdrawal symptoms including seizures, delirium tremens, severeanxiety or autonomic instability, but to withdraw the medication before physicaldependence on its effects begins.1.3 The process should be conducted in a safe and structured manner so as toreduce the likelihood of potential adverse events. The structured approach willinclude careful assessment and discussion at the multi-disciplinary teammeeting of a client’s suitability for a medically assisted alcohol detoxification.This discussion should take into account several factors including the client’smotivation to engage in a detoxification, current physical and mental health,social support, consideration of any absolute contraindications e.g. past historyof seizures or delirium tremens, and the client’s future treatment plans/goals.There should be an after-care plan in place so that the client continues to besupported to remain alcohol-free in the period following detoxification andsupported to develop skills needed to maintain long-term sobriety.2.Aims and objectives2.1 This policy will set out the procedure for carrying out a medically assistedcommunity alcohol withdrawal safely. The policy draws on recent NICEguidance (CG115) on ‘Alcohol use disorders: diagnosis, assessment andmanagement of harmful drinking and alcohol dependence’.2.2 This document aims to achieve the following objectives:2.2.1 Make clear the inclusion and exclusion criteria for medically assistedcommunity alcohol withdrawal.2.2.2 Explain the roles and responsibilities of staff conducting medicallyassisted community alcohol withdrawal.2.2.3 Set out a number of possible medically supervised detoxification regimenswhich can be used for the withdrawal process.2.2.4 Describe the different types of medications that can be used followingmedically assisted alcohol withdrawal and explain how to prescribe these.1 Community Alcohol Withdrawal Prescribing Guidelines: PHA28: Mar 2020
2.2.5 Provide a number of useful appendices including client informationsheets, GP letter and well validated rating scales to measure severity ofalcohol dependence and withdrawal symptoms.3.Scope of the policyThis policy is intended for staff working in Camden and Islington NHS FoundationTrust specialist substance misuse services and other trust sites where communityalcohol detoxification may be undertaken. The policy does not apply to themanagement of in-patients admitted on mental health wards, however alcoholdetoxification may be undertaken in inpatient mental health wards using thedetoxification schedules listed in this policy and in consultation with specialist alcoholnurses at trust substance misuse services.4.Assessing suitability for community alcohol withdrawal4.1 For service users who typically drink over 15 units of alcohol per day, and/orwho score 20 or more on the AUDIT, consider either:a) Assessment for and delivery of a community-based assisted withdrawal; orb) Assessment and management in specialist inpatient alcohol services if thereare safety concerns about a community-based assisted withdrawal.4.2 In the week prior to medically assisted alcohol withdrawal, use formalassessment tools to assess the nature and severity of alcohol misuse, includingthe:Alcohol use disorders Identification Tool (AUDIT) for identification and as aroutine outcome measureSeverity of Alcohol Dependence Questionnaire (SADQ) (Appendix 4)Leeds Dependence Questionnaire (LDQ) to assess severity of dependence.4.3 When assessing the severity of alcohol dependence and determining the needfor assisted withdrawal, adjust the criteria for women, older people, children andyoung people, and people with established liver disease who may haveproblems with the metabolism of alcohol.4.4 For service users having assisted withdrawal, particularly those who with severe(SADQ score over 30 or drinking over 50 units of alcohol per week) alcoholdependence use a formal measure of withdrawal symptoms such as the ClinicalInstitute Withdrawal Assessment Revised (CIWA-Ar) (see Appendix 4).Inclusion/Exclusion criteria: OutpatientAlcohol WithdrawalLEVEL OF DEPENDENCEMild to moderate dependence withoutsignificant co morbidity.- Mild/moderate dependence complexneeds / Severe dependenceDrinking over 30 units/ dayversus Inpatient Medically AssistedINTERVENTIONOutpatient-based assisted withdrawal- Monitor client every other day.Outpatient- based assisted withdrawalMonitor client daily.Inpatient or Residential Assisted2 Community Alcohol Withdrawal Prescribing Guidelines: PHA28: Mar 2020
SADQ score 30A history of epilepsy, seizures ordelirium tremens15-20 units/ day along with significantpsychiatric or physical co morbidities,a significant learning disability orcognitive impairment.Concurrent benzodiazepine withdrawal.5.Withdrawal Programme.Lower threshold in vulnerable groupse.g. homeless and older people.Information to be obtained prior to commencement of medically assistedwithdrawal5.1 The key worker should meet the service user on two separate occasions todiscuss the detoxification process and possible aftercare plans.Theassessment may include a relative or spouse, who will be involved in providingsupport during the medically assisted withdrawal process. The followinginformation should be presented by the key worker at the multidisciplinary teammeeting before detoxification commences: Eligibility criteria agreed by team, procedure explained to client by keyworker and consent form signed by client. Date for commencement and availability of staff (requires planning takingaccount of annual/ other leave). Information from GP: List of medications, physical problems, allergies, bloodtest results (less than 6 months old), including liver function test (LFTs)results (ALT, AST, ALP, GGT, Total Bilirubin, Albumin, PT/INR) Blood test results including LFTs must be seen by the doctor at least oneweek prior to commencement of medically assisted withdrawal. Drink Diaries for a minimum of two weeks. Baseline observations (pulse, BP, breath alcohol concentration (BAC). Risk assessment and SADQ completed. Aftercare plan agreed with client.5.2 The service user must sign a contract agreeing to attend the clinic at a specifiedfrequency, and to remain abstinent from alcohol and undergo breath alcoholtesting and physical observations during the withdrawal process. The clientmust sign a consent form (appendix 1) and a post-withdrawal care plan that hasbeen agreed with the key worker and discussed with the multi-disciplinary teambeforehand.5.3 If a service user plans to attend a day programme or residential rehabilitationcentre, a visit to the centre should be made before the medically assistedwithdrawal commences. The programme will need to provide approval and anagreement made for the client to attend before starting the medically assistedalcohol withdrawal. Attendance at Alcoholics Anonymous (AA) alone will not beadequate as a post-withdrawal care plan. If the post-withdrawal care planincludes placement in a residential rehabilitation centre or day programmerequiring funding from social services or the primary care trust, a communitycare assessment (CCA) should be completed with a social worker beforestarting the withdrawal process.3 Community Alcohol Withdrawal Prescribing Guidelines: PHA28: Mar 2020
5.4 If the post-withdrawal plan includes disulfiram or acamprosate prescribing (thisshould be discussed and agreed at the multi-disciplinary team meetingbeforehand), an appointment should be arranged to see a psychiatrist to explainthe medications available including their potential side effects and a decisionmade in agreement with the service user as to which (if any) to prescribefollowing medically assisted withdrawal.6.Procedure for medically assisted alcohol withdrawal6.1 Clients will see a doctor or a nurse prescriber on the Monday morning oncommencement of community alcohol withdrawal. A key worker will review theclient at an agreed frequency thereafter for the remainder of the withdrawalperiod. In the event of the client’s allocated key worker being on leave, it will betheir responsibility to arrange for another team member to see the client at anagreed frequency during the withdrawal process. As the alcohol service isclosed on public holidays, take home medication will be prescribed for dayswhen the service is shut. However for clients with severe dependence (SADQscore over 30 or drinking in excess of 50 units per week), medically assistedwithdrawal should not take place on a week including a public holiday, so thatthe client will have the opportunity to come in to the service on a daily basis.6.2 BAC readings during medically assisted alcohol withdrawalBreath alcohol concentrationZero on commencement and on eachsubsequent appointment during medicallyassisted withdrawal.Between zero and 0.5 on commencementof medically assisted withdrawal withobjective evidence of withdrawalsymptoms.Above zero on any day after the first day ofmedically assisted withdrawal.Treatment planStart/ continue medically assistedwithdrawal.Continue medically assistedwithdrawal.Stop medically assistedwithdrawal.6.3 Individuals will be given FP10 prescriptions for their medications.Themedication prescribed should be documented on the client’s electronic patientrecord as well as on the FP10 prescription record sheet. Treatment contract andSADQ scores should also be documented on the electronic patient records.6.4 Chlordiazepoxide will be used for medically assisted community alcoholwithdrawal. The starting and subsequent day’s dosing regimen will be decidedon the basis of clinical assessment of the client. The starting and subsequentday’s dosing will be determined by a number of factors including the client’sSADQ score done prior to detoxification, clinical presentation (including BP,pulse, respiratory rate, breath alcohol concentration (BAC) and physical andmental state) and CIWA (clinical institute withdrawal assessment) scores.6.5 Oral thiamine should be prescribed for the prevention of Wernicke-Korsakoffsyndrome where any of the following apply:4 Community Alcohol Withdrawal Prescribing Guidelines: PHA28: Mar 2020
Malnourished or at risk of malnourishedDecompensated liver diseaseAcute withdrawalBefore and during a planned medically assisted alcohol withdrawalThe recommended dose is 200mg to 300mg daily in divided doses.Thiamine should be continued for as long as malnutrition is present and / orduring periods of alcohol consumption.Following successful alcohol withdrawal. Thiamine should be continued for 6weeks. If after this time the patient remains abstinent and has regainedadequate nutritional, thiamine should be discontinued. Thiamine should berestarted if the patient starts drinking again.Continuing need of thiamine should be reviewed at appropriate intervals whichmay depend on individual circumstances.6.6 When managing alcohol withdrawal in the community, avoid giving people whomisuse alcohol large quantities of medication to take home to prevent overdoseor diversion. Prescribe for installment dispensing, with no more than 2 days’medication supplied at any time. For people with liver impairment, an inpatientdetoxification using benzodiazepines with a shorter half-life (e.g oxazepam)would be deemed most appropriate. When managing withdrawal from coexisting benzodiazepine and alcohol dependence increase the dose ofbenzodiazepine medication used for withdrawal. Calculate the initial daily dosebased on the requirements for alcohol withdrawal plus the equivalent regularlyused daily dose of benzodiazepine. This is best managed with one rather thanmultiple benzodiazepines.6.6 Be aware that chlordiazepoxide doses may need to be reduced for children andyoung people, older people, and people with liver impairment.6.7 Chlordiazepoxide reducing dose regimes based on SADQ scores on day 1Daily AlcoholConsumptionSeverity ofdependenceDay 1Day 2Day 3Day 4Day 515-25 units30-40 unitsMild/Moderate:SADQScore 3015mg25mgqdsqds10mqd 20mgsqds10mg15mgtdsqds5mg10mqdstds5mg bd 10mgtdsSevere: SADQScore 30-4030mgqds25mgqds20mgqds15mgqds10mqds50-60 unitsVery Severe:SADQ score40-6040mg qds 50mg qds35mg qds 45mg qds30mg qds 40mg qds25mg qds 35mg qds20mg qds 30mg qds5 Community Alcohol Withdrawal Prescribing Guidelines: PHA28: Mar 2020
Day 6Day 7Day 8Day 9Day 10Day 115mgnocte5mg tds 10mgtds5mg bd 5mg tds5mg5mg bdnocte5mgnocte15mg qds 25mg qds10mqds10mg tds20mg qds15mg qds5mg tds10mqds5mg bd5mgnocte10mg tds5mg tdsDay 12Day 135mg bd5mg nocte6.8 Medication(s) for medically assisted community alcohol withdrawal will beprovided using FP10 prescriptions. The prescription pad will be kept on site in alocked cupboard. The key will be kept in a locked safe on site. No medicationfor detoxifications will be kept on site.6.9 In the unlikely event that a client presents in acute severe withdrawals orexperiences seizures or other physical emergencies necessitating immediatemedical attention, an ambulance should be called by dialling 999.7.Medication interventions following successful withdrawal7.1 After a successful withdrawal for people with moderate and severe alcoholdependence, consider offering acamprosate or oral naltrexone in combinationwith an individual psychological intervention (e.g. cognitive behavioural therapy)focused specifically on alcohol misuse.7.2 After a successful withdrawal for people with moderate and severe alcoholdependence consider offering disulfiram in combination with a psychologicalintervention to service users who: have a goal of abstinence but for whom acamprosate and oral naltrexoneare not suitable, or prefer disulfiram and understand the relative risks of taking the drug.7.3 Before starting treatment with acamprosate, oral naltrexone or disulfiram,conduct a comprehensive medical assessment (baseline urea and electrolytesand liver function tests including gamma glutamyl transferase [GGT]). Inparticular, consider any contraindications or cautions, and discuss these with theservice user. For further information refer to the summary of productcharacteristics (SPC) site of the Medicines and Health Regulatory Authority(MHRA) - http://www.mhra.gov.uk/spc-pil/7.4 AcamprosateIf using acamprosate, start treatment as soon as possible after assistedwithdrawal. Usually prescribe at a dose of 1998 mg (666 mg three times a day)unless the service user weighs less than 60 kg, and then a maximum of 1332mg should be prescribed per day. Acamprosate should:6 Community Alcohol Withdrawal Prescribing Guidelines: PHA28: Mar 2020
usually be prescribed for up to 6 months, or longer for those benefiting fromthe drug who want to continue with it be stopped if drinking persists 4–6 weeks after starting the drug.Service users taking acamprosate should stay under supervision, at leastmonthly, for 6 months, and at reduced but regular intervals if the drug iscontinued after 6 months. Do not use blood tests routinely, but consider them tomonitor for recovery of liver function and as a motivational aid for service usersto show improvement.7.5 NaltrexoneIf using oral naltrexone start treatment after assisted withdrawal. Startprescribing at a dose of 25 mg per day and aim for a maintenance dose of 50mg per day. Draw the service user’s attention to the information card that isissued with oral naltrexone about its impact on opioid-based analgesics. Oralnaltrexone should: usually be prescribed for up to 6 months, or longer for those benefiting fromthe drug who want to continue with it Be stopped if drinking persists 4–6 weeks after starting the drug.Service users taking oral naltrexone should stay under supervision, at leastmonthly, for 6 months, and at reduced but regular intervals if the drug iscontinued after 6 months. Do not use blood tests routinely, but consider them forolder people, for people with obesity, for monitoring recovery of liver functionand as a motivational aid for service users to show improvement. If the serviceuser feels unwell advise them to stop the oral naltrexone immediately.7.6 Disulfiram7.6.1 If using disulfiram, start treatment at least 24 hours after the last alcoholic drinkconsumed. Usually prescribe at a dose of 200 mg per day. For service userswho continue to drink, if a dose of 200 mg (taken regularly for at least 1 week)does not cause a sufficiently unpleasant reaction to deter drinking, considerincreasing the dose in consultation with the service user.7.6.2 Before starting treatment with disulfiram, test liver function, urea andelectrolytes to assess for liver or renal impairment. Check the SPC forwarnings and contraindications in pregnancy and in the following conditions: ahistory of severe mental illness, stroke, heart disease or hypertension.7.6.3 Make sure that service users taking disulfiram: stay under supervision, at least every 2 weeks for the first 2 months, thenmonthly for the following 4 months if possible, have a family member or carer, who is properly informed aboutthe use of disulfiram, oversee the administration of the drug are medically monitored at least every 6 months after the initial 6 months oftreatment and monitoring.7.6.4 Warn service users taking disulfiram, and their families and carers, about: the interaction between disulfiram and alcohol (which may also be found infood, perfume, aerosol sprays and so on), the symptoms of which may include7 Community Alcohol Withdrawal Prescribing Guidelines: PHA28: Mar 2020
flushing, nausea, palpitations and, more seriously, arrhythmias, hypotensionand collapse the rapid and unpredictable onset of the rare complication of hepatotoxicity;advise service users that if they feel unwell or develop a fever or jaundice thatthey should stop taking disulfiram and seek urgent medical attention.The above medication prescribing should be handed over to GPs in line with locallyagreed pathways. The medications can be continued by GPs on repeat prescriptionafter specialist prescribing ceases and for as long as is deemed necessary for thepatient to remain on them. The specialist doctor should write to the GP and advise aperiod of time for which the medication(s) should be continued (usually for between6-12 months, and disulfiram should be stopped if the client starts consuming alcoholat any point in time). Further detailed information about these drugs can be found ttp://www.medicines.org.uk/emc/8.Dissemination and implementation arrangementsThis policy will be circulated to all team members working in Camden SpecialistAlcohol Treatment Service. The policy will also be circulated to other Camdensubstance misuse services and staff. Dr Bhaskar Punukollu can be contacted forclarification or support in relation to any aspect of this policy by email onBhaskar.punukollu@candi.nhs.uk.9.Training requirementsImplementation of this policy will be complemented by a training event for staffworking in Camden Specialist Alcohol Service and the partner service CRI, in linewith the trust’s mandatory training policy and the learning and development guide.For training requirements please refer to the Trust’s Mandatory Training Policy andLearning and Development Guide.10. Monitoring and audit arrangementsRegular audits will be conducted periodically to ensure that community alcoholwithdrawals are being conducted in line with the policy. The audit will aim to ensurethat appropriate assessment (including blood tests, liaison with GP and contract/consent forms being signed) has been conducted prior to commencement ofdetoxification and that the detoxification process itself follows the guidelines in termsof medication prescribing both during and following successful completion ofwithdrawal. The results will be reported to the trust audit committee. Learning fromthe audit will be shared with staff at the service at local continuing professionaldevelopment meetings.8 Community Alcohol Withdrawal Prescribing Guidelines: PHA28: Mar 2020
11. Review of the policy3 years12. References Element to bemonitoredCG 115: Alcohol dependence and harmful use: NICE Guidance 28thFeb 2011.1.2, 4, 6.4, 6.5 and 7 were excerpts from the NICE GuidelineCG115.RMOC position statement: Vitamin B supplementation in alcoholism.NHSE Nov 2019.LeadHow Trust willmonitorcomplianceFrequencySee list of NHSLAminimumrequirements ifrelevantChlordiazepoxideprescribing is beingdone in line with therecommendedprocedures outlinedin this policy(dosages based onSADQ and CIWAscores)Nursingandmedicalteam atCSATSCarry out an auditofchlordiazepoxideprescribing.AnnuallyEnsure that liverfunction test resultsare obtained prior tocommencement ofmedically assistedwithdrawalNursingandmedicalteam atalcoholservices.Carry out an auditof blood ittee orgroup willthemonitoringreport go to?Drugs andTherapeuticsGroupDrugs andTherapeuticsGroupActing onrecommendations and Lead(s)Change in practiceand lessons to besharedWhich committeeor group will act onrecommendations?How will changes beimplemented andlessons learnt/shared?Drugs andTherapeuticsGroup /Pharmacists.Ensure that allPrescribersfollow trustpolicy –ImmediateReview of policy;implementationpractices andprocedures.Re- auditGive feedback toprescribers.13. Associated documentsThere are no associated trust documents that this policy directly relates to.AppendicesAppendix 1 CONTRACT AND CONSENT FORM FOR MEDICALLY ASSISTEDCOMMUNITY ALCOHOL WITHDRAWALThe following stipulations have been designed to help you in the next couple ofweeks, so that you have the best chance of giving up alcohol, as it is your wish. The programme requires that you be abstinent from alcohol and non-prescribeddrugs. Thus, while on the programme you must not consume or possess anyalcohol or drugs other than those prescribed by the doctor. During this time you9 Community Alcohol Withdrawal Prescribing Guidelines: PHA28: Mar 2020
will be asked to be breathalysed and you may be requested to supply a urinesample for drug screening. If either of these proves positive, you will not be ableto continue with the programme. You may be able to join the programme again ata later date, but you should discuss first with your keyworker whether this is stillthe most appropriate option for you. In order to get the maximum benefit from the programme, you will need to give ityour full priority. If you are working, it is strongly suggested that you arrange totake time off for an extended period, to give yourself space for the detox andrecovery. You will be expected to stay the full duration of the sessions, for the wholeprogramme, and to take all medication as prescribed by the doctor and detoxnurse. Should you miss a session for whatever reason, you will not be able tocontinue with the programme. Aggressive, violent, abusive, racist or sexist language or behaviour can not betolerated. If you demonstrate any of these you will be asked to leave theprogramme.Please sign below to confirm that the community alcohol detoxification programmehas been explained to you, that you wish to go ahead with it and that you are happywith the conditions set above.Name Date Address Worker .10 Community Alcohol Withdrawal Prescribing Guidelines: PHA28: Mar 2020
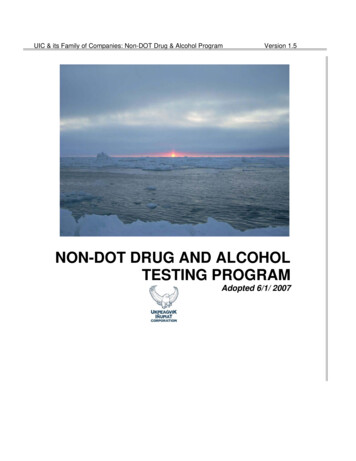
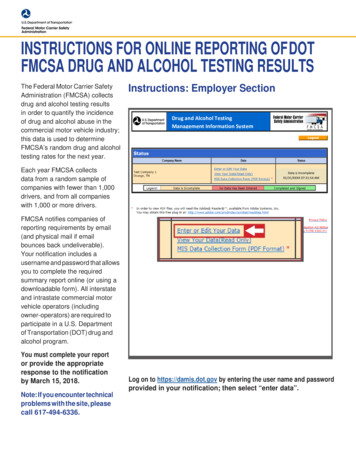
CSATS Guidelines for Medically Assisted Community Alcohol WithdrawalAppendix 2 INFORMATION SHEETAlcohol detoxification takes place at CamdenSpecialist Alcohol Treatment Service(CSATS) on the following morningsMonday9.30-11amConsultant (doctor) clinicTuesday, WednesdayFrom 9.30am with either key worker or doctorFridayFrom 9.30am with key worker Points to RememberCAMDEN & ISLINGON NHS TRUSTYour SafetyDuring detoxification you may experienceforgetfulness, irritability and poorcoordination: be careful, therefore, whencooking, boiling water and doing othertasks that require care. It would be helpfulfor you to arrange to have a responsibleperson around during this time, to help youwith these practicalities.Medically assistedcommunity alcoholwithdrawal programmeYour EnvironmentTry to arrange it so that your surroundingsare as peaceful as possible. For this, itmay be best to let those around you knowthat you will probably be feeling fragile fora few days. Also, it is advisable that youdon’t keep alcohol in your home. In theearly stages of recovery you will bevulnerable, so avoid situations wherealcohol is consumed or openly available.The programme is run by[Doctor name][Nurse name]Your TimeMost people find that if they keep busy, ithelps them not to dwell on negativefeelings. Give the coming week someconsideration: don’t leave things tochance.Your DietTry to eat something even when you arenot hungry. Eating little and often will helpminimise craving. Drink plenty of fluids.11 Community Alcohol Withdrawal Prescribing Guidelines: PHA28: Mar 2020*Specialist Alcohol Treatment ServiceTel: 0207 530 5900You have made the very important decision tostop using alcohol and this programme hasbeen put together to give you the bestpossible chance to achieve this goal.This leaflet will give you essential informationabout alcohol detoxification and inform you ofwhat you can expect from us and what weexpect from you. Please read it carefully anddon’t be afraid to ask questions
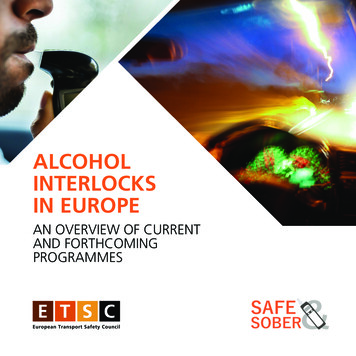
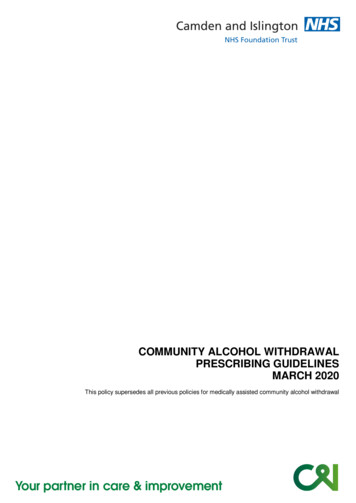
CSATS Guidelines for Medically Assisted Community Alcohol WithdrawalWithdrawal SymptomsWhat you can expect from usWithdrawing from alcohol is oftenaccompanied by some unpleasantexperiences, such as shaking, anxiety, feelingjumpy and nervous, feeling irritable, sweating,nausea, racing thoughts and insomnia.When you start on this programme, youwill be assessed by a doctor, who willprescribe the medication. A nurse will thenmonitor withdrawal closely, helping you toplan the week and to cope with thesesymptoms.These are withdrawal symptoms and withmedication the worst aspects can be relieved.However, alcohol intoxication places a heavyburden on the body and consequently youshould expect to experience some discomfort.On this programme, you will be prescribed amedication called chlordiazepoxide. This isusually quite safe, but can make peopledrowsy. Thus, during detoxification it isrecommended that you refrain from driving,operating machinery or undertaking anytasks that require being alert. In addition,the medication is not safe when takentogether with alcohol and thus if you resumedrinking you must stop taking it at once.For some people withdrawal symptoms aremore severe, including for example: Confusion Disorientation Blacking out Hallucinations FitsIf you do experience any severe symptomsyou will need to seek immediate assistance atthe nearest Accident & EmergencyDepartment.What we expect from youThe following stipulations have beendesigned to help you in the next couple ofweeks, so that you have the best chanceof giving up alcohol, as it is your wish. The programme requires that you beabstinent from alcohol and nonprescribed drugs. Thus, wh
1 Community Alcohol Withdrawal Prescribing Guidelines: PHA28: Mar 2020 1. Introduction 1.1 Medically assisted community alcohol withdrawal is a process in which an individual's physical and mental health are monitored whilst being provided medications and psychosocial support to relieve physical and psychological