Transcription
Underwritten by Metropolitan Life Insurance Company (MetLife)NexGenADULT FORMER DEPENDENT LIFEWelcome toMilitary BenefitAssociation (MBA)We are a nonprofit organization of militarypersonnel, civilian employees of the UnitedStates Government, veterans, their spouses,and dependent/former dependent children.We sponsor for our Members an attractivepackage of insurance and other benefits.Established in 1956, MBA is one of theoldest and largest associations of its kind.ELIGIBILITYYou are eligible if you were at one time a dependentchild of an MBA member or former MBA memberand you are at least age 21 but under age 62.COVERAGE FEATURESAmounts AvailableAs an eligible applicant, you may apply for group term lifeinsurance in amounts up to 250,000, in units of 50,000.Continuous Coverage to Age 7024 hours a day, anywhere in the world, during times of warand peace. Coverage ends at age 70.Emergency Death Benefit1An advance payment of up to 10,000 may be paid to thedesignated beneficiary on the death of the Insured uponrequest and verification.Accelerated Benefits Option2For access to funds during a difficult timeYou can receive up to 80% of your Term Life insuranceproceeds to a maximum of 200,000 in the event thatyou become terminally ill and are diagnosed with lessthan 12 months to live. This can go a long way towardhelping your family meet medical and other relatedexpenses at this difficult time.Effective Date of InsuranceCoverage becomes effective on the first day of the monthfollowing both (a) approval of your application for insuranceand (b) receipt by MBA of the required premium. Please notethat the effective date of coverage will be delayed if illnessprevents you from completing a day of regular employmentor if you are confined to a hospital, at home under the care ofa physician for any medical reason, or if you have applied toreceive or are receiving disability income from any source forany medical reason.Conversion PrivilegeMembers have a conversion privilege upon the occurrence ofcertain events, including upon termination of group coverage,at age 70, to an individual policy of life insurance with MetLife,as explained in the certificate of coverage.ExclusionNo benefit will be paid if the Member's death occurs fromsuicide, or if health is misrepresented, in the first two yearsof coverage. Instead, the premium will be refunded.Cancellation Protection, TerminationLife insurance coverage cannot be terminated by the insurerprior to age 70, as long as MBA membership continues, themaster group policy stays in force, premiums continue to bepaid and the above exclusions do not apply.MBA-AFD-A (01/19)
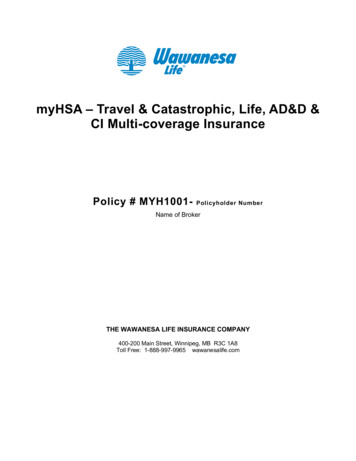
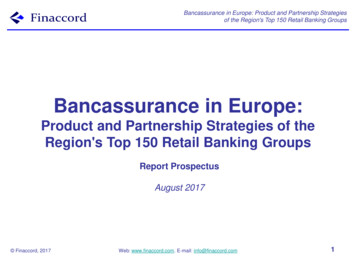
ADULT FORMER DEPENDENT LIFEMONTHLY PREMIUM/COVERAGE (MALES)AGENonTobaccoTobaccoPremium Rates 50,000 100,000 150,000 200,000 250,000Thru 29 6.88 10.83 15.00 19.17 23.3330-34 7.50 12.08 16.88 21.67 26.4635-39 8.75 13.75 19.38 25.00 30.6340-44 11.46 19.17 27.50 35.83 44.1745-49 16.67 30.42 44.38 58.33 72.2950-54 20.83 36.25 53.13 70.00 86.8855-59 25.00 48.75 71.88 95.00 118.1360-64 39.17 75.83 112.50 149.17 185.8365-69 62.50 122.08 181.88 241.67 301.46AGE 50,000 100,000 150,000 200,000 250,000Thru 29 13.76 21.66 30.00 38.34 46.6630-34 15.00 24.16 33.76 43.34 52.9235-39 17.50 27.50 38.76 50.00 61.2640-44 22.92 38.34 55.00 71.66 88.3445-49 33.34 60.84 88.76 116.66 144.5850-54 41.66 72.50 106.26 140.00 173.7655-59 50.00 97.50 143.76 190.00 236.2660-64 78.34 151.66 225.00 298.34 371.6665-69 125.00 244.16 363.76 483.34 602.92Rates are based on your current age on your effective date of coverage. Rates will change when you move into a higher age band ormay change at anytime if the entire Group's rates are changed. An increase in your allotment or premium payment will be necessaryif one of these events occurs. If you fail to pay the increase in premium, your coverage will be continued, but at a reduced amount.
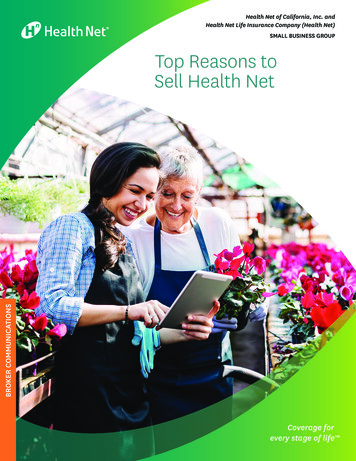
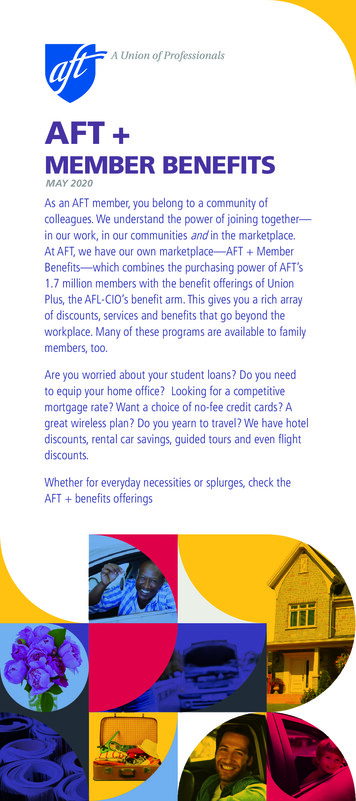
ADULT FORMER DEPENDENT LIFEMONTHLY PREMIUM/COVERAGE (FEMALES)AGENonTobaccoTobaccoPremium Rates 50,000 100,000 150,000 200,000 250,000Thru 29 5.21 8.33 11.25 14.17 17.0830-34 6.04 10.00 13.75 17.50 21.2535-39 7.50 11.25 15.63 20.00 24.3840-44 10.21 17.92 25.63 33.33 41.0445-49 12.29 20.83 30.00 39.17 48.3350-54 14.17 25.00 36.25 47.50 58.7555-59 20.83 37.92 55.63 73.33 91.0460-64 35.00 66.67 98.75 130.83 162.9265-69 51.04 98.75 146.88 195.00 243.13AGE 50,000 100,000 150,000 200,000 250,000Thru 29 10.42 16.66 22.50 28.34 34.1630-34 12.08 20.00 27.50 35.00 42.5035-39 15.00 22.50 31.26 40.00 48.7640-44 20.42 35.84 51.26 66.66 82.0845-49 24.58 41.66 60.00 78.34 96.6650-54 28.34 50.00 72.50 95.00 117.5055-59 41.66 75.84 111.26 146.66 182.0860-64 70.00 133.34 197.50 261.66 325.8465-69 102.08 197.50 293.76 390.00 486.26Rates are based on your current age on your effective date of coverage. Rates will change when you move into a higher age band ormay change at anytime if the entire Group's rates are changed. An increase in your allotment or premium payment will be necessaryif one of these events occurs. If you fail to pay the increase in premium, your coverage will be continued, but at a reduced amount.
HOW TO APPLYComplete the Enrollment ApplicationForm — Requests for membership and insurancemust be approved by MBA and MetLife. Be sure tocomplete the Enrollment Application Form, front andback. Additional evidence of insurability and/or amedical examination may be required. The maximumcoverage available on the NexGen Adult FormerDependent application through MBA with MetLifeis 250,000.Return the Enrollment ApplicationForm — You must meet eligibility for membershiprequirements on the effective date of insurancecoverage. Therefore, enrollment application formsmust be approved and payment of the first month’spremium must be received while you are still eligible.Enrollment application forms should be received atleast three months before termination of eligibility.Enclose Your Method of Payment — To paymonthly premiums by Electronic Funds Transfer (EFT)from your bank or credit union, please complete andenclose the EFT Authorization form and include avoided check with the enrollment application form.To pay premium by credit card, please complete andenclose the Credit Card Authorization Form.To pay your premium by check or money order,please enclose a check or money order payable toMBA for three months of premium with the enrollmentapplication form. You will be billed quarterly or semiannually for future premiums.Coverage will either be approved by MetLife based upon its underwriting rules and your answers or you will be asked to submit additional medicalinformation in order for MetLife to complete its review of your application for coverage. Coverage is not available in all states and certain statelimitations may apply to some provisions. All applications are subject to review and approval by Metropolitan Life Insurance Company basedupon its underwriting rules.Like most group insurance policies, MetLife's policies contain certain exclusions, exceptions, waiting periods, reductions, limitations and terms forkeeping them in force. Association Group Term Life Insurance is issued by Metropolitan Life Insurance Company (MetLife), New York, NY, policyform # 149107-1-G.1Benefit is payable after 2 years and cannot exceed 50% of coverage.The Accelerated Benefits Option is subject to state regulation and is intended to qualify for favorable tax treatment, in which case the benefits will beexcludable from income and not subject to federal taxation. This information was written as a supplement to the marketing of life insurance products.Tax laws relating to accelerated benefits are complex and limitations may apply. You are advised to consult with and rely on an independent tax advisorabout your own particular circumstances. Receipt of accelerated benefits may affect your eligibility, or that of your spouse or your family, for publicassistance programs such as medical assistance (Medicaid), Temporary Assistance to Needy Families (TANF), Supplementary Social Security Income(SSI) and drug assistance programs. You are advised to consult with social service agencies concerning the effect that receipt of accelerated benefitsmay have on public assistance eligibility for you, your spouse or your family.2For further assistance or information call us toll free 1-800-336-0100, 8 am to 4 pm, Monday through Friday, Eastern Time
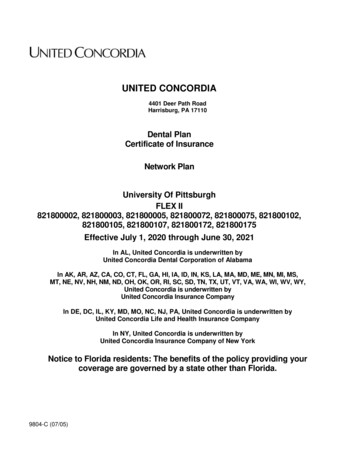
Life InsuranceCompany,Metropolitan LifeMetropolitanInsurance CompanyNY, NY10166 NY, NY 10166Metropolitan Life Insurance Company NY, NY 10166AUXILIARY MEMBER (NEXGEN ADULT FORMER DEPENDENT) ENROLLMENT CHANGE FORMAUXILIARY MEMBER (NEXGEN ADULT FORMER DEPENDENT) ENROLLMENT CHANGE FORMSECTION 1 – Your Enrollment Information (To be Completed by the Auxiliary Member)SECTION 1 – Your Enrollment Information (To be Completed by the Auxiliary Member)NexGen Adult Former DependentNexGen Adult Former DependentAuxiliary Member’s Name (First, Middle, Last)Auxiliary Member’s Name (First, Middle, Last)MaleFemaleMaleFemaleCurrent Mailing Address (Street, City, State, Zip Code)Current Mailing Address (Street, City, State, Zip Code)Home/Cell Phone #Home/Cell Phone #MarriedMarriedSingleSingleAuxiliary Member’s SSN #AuxiliarySSN #– ork Phone #Work Phone #Date of Birth (MM/DD/YYYY)Date of Birth (MM/DD/YYYY)Personal Email AddressPersonal Email AddressSECTION 2 – Member (Sponsor) InformationSECTION 2 – Member (Sponsor) InformationMember (sponsor’s) Name (First, Middle, Last)Member (sponsor’s) Name (First, Middle, Last)Member (sponsor’s) SSN #Member (sponsor’s) SSN #––––SECTION 3 – Coverage SelectionSECTION 3 – Coverage SelectionSelect one:New MemberCurrent Member Requesting Additional CoverageCurrent Member Requesting Change in CoverageSelect one:New MemberCurrent Member Requesting Additional CoverageCurrent Member Requesting Change in CoverageI have read my enrollment materials and request the following coverage as indicated below. I understand that contributions are required for theI have readmy enrollmentbenefitsI selectbelow. materials and request the following coverage as indicated below. I understand that contributions are required for thebenefits I select below.I understand health information is not required if I enroll within 90 days after my eligibility under NexGen Child coverage ends and:I understandinformationis notI amrequiredwithincoverage90 daysupaftermy eligibility under NexGen Child coverage ends and:if previouslyhealthenrolledfor 10,000,eligibleif Itoenrollincreaseto 50,000. if previously enrolled for 20,000 10,000,orI ameligibleI amto increaseto 50,000. 25,000;eligible tocoverageincreaseupcoverageup to 100,000. if previously enrolled for 20,000 or 25,000; I am eligible to increase coverage up to 100,000.Auxiliary Member Life Insurance 1Auxiliary Member Life Insurance 1 50,000 100,000 150,000 200,000 250,000 50,000 100,000 150,000 200,000 250,000Is this insurance coverage intended to replace any existing life insurance or annuity contracts currently held by you (except for current MBAIs thisLifeinsurancecoverageintended toGroupreplaceLifeanyInsuranceexisting lifeinsuranceor annuitycontractscurrentlyheld by (FEGLI)you LI)or FederalEmployees’GroupLife Insurance)? urance(FEGLI))?1 Life Insurance may include an Accelerated Benefits Option under which a terminally ill insured can accelerate a portion of his or her life insurance amount.1 Life Insurance may include an Accelerated Benefits Option under which a terminally ill insured can accelerate a portion of his or her life insurance amount.An interest and expense charge may be deducted from the accelerated payment. Receipt of accelerated benefits may affect eligibility for public assistance.An interestchargemayarebe deductedacceleratedReceiptof accelerated benefits may affect eligibility for public assistance.Thisbenefitandmayexpensebe taxableand youadvised tofromseektheassistancefrompayment.a personaltax advisor.This benefit may be taxable and you are advised to seek assistance from a personal tax advisor.FOR INTERNAL USE ONLY – Group Customer Information to be completed by the RecordkeeperFOR INTERNAL USE ONLY – Group Customer Information to be completed by the RecordkeeperName of Group Customer/AssociationName ofBenefitGroup Customer/AssociationMilitaryAssociation (MBA)Military Benefit Association (MBA)Date of Membership (MM/DD/YYYY)Date of Membership (MM/DD/YYYY)Member ID #Member ID #Group Customer #Group Customer #01491070149107Experience #Experience #Report #Report #Sub CodeSub CodeCoverage Effective Date (MM/DD/YYYY)Coverage Effective Date (MM/DD/YYYY)GEF02-1GEF02-1ADMADMform number above applies to residents of all states except as follows: Form number GEF09-1 applies to residents of Montana;(TheGEF02-1(The form number above applies to residents of all states except as follows: Form number GEF09-1 applies to residents of Montana;GEF02-1ADMapplies to residents of Connecticut, North Dakota and Utah)ADM applies to residents of Connecticut, North Dakota SUBMISSIONand Utah)INSTRUCTIONSSUBMISSION INSTRUCTIONSAfter completion, sign and date the form on the last page where indicated. Make a copy for your records and return the original toAftercompletion,signASSOCIATION,and date the formon Avionthe lastpage whereindicated.Makea copyVAfor20153-1110your recordstheoriginal toMILITARYBENEFIT14605Parkway,P.O. Box221110,Chantilly,orandfax returnto (703)968-6423.MILITARY BENEFIT ASSOCIATION, 14605 Avion Parkway, P.O. Box 221110, Chantilly, VA 20153-1110 or fax to (703) 968-6423.Page 1 of 4MBA –ENROLL-Auxiliary Member (12/18)Page 1 of 4MBA –ENROLL-Auxiliary(12/18)Initial SSN#Member(Last 4)Initial SSN# (Last 4)
SECTION 44 -- PaymentPayment InformationInformationSECTIONAA completedcompleted EFTEFT authorizationauthorization (monthly(monthly only)only) formform fromfrom mymy checkingchecking ationforautomaticpayment.A completed credit/debit card authorization for automatic payment.MilitaryMilitary AllotmentAllotment AuthorizationAuthorization (complete(complete thethe RequestRequest forfor AllotmentAllotment sectionsection ofof thethe AdditionalAdditional FormsForms andand InformationInformation k/Money Order for the first three (3) months. DO NOT SEND CASH. Coverage will be effective on the firstfirst ofof thethe followingfollowing month,month, afterafter tions.approval and receipt of required contributions.For immediateimmediate coveragecoverage (effective(effective afterafter MetLifeMetLife approvalapproval andand receiptreceipt ofof requiredrequired contributions)contributions) encloseenclose aa check/moneycheck/money orderorder forfor thethe firstfirst threethree (3)(3)Formonths.months. DODO NOTNOT SENDSEND CASHCASHSECTION 55–– TobaccoTobacco UseUseSECTIONAuxiliaryAuxiliary MemberMemberYesNoYesNoHaveHave youyou usedused tobaccotobacco inin anyany formform inin thethe pastpast 1212 months?months?GEF02-1GEF02-1ADMADM(The(The formform numbernumber aboveabove appliesapplies toto residentsresidents ofof allall statesstates exceptexcept asas follows:follows: FormForm numbernumber GEF09-1GEF09-1 appliesapplies toto residentsresidents ofof Montana;Montana;GEF02-1GEF02-1ADMADM appliesapplies toto residentsresidents ofof Connecticut,Connecticut, NorthNorth DakotaDakota andand Utah)Utah)SECTION 66–– HealthHealth InformationInformationSECTIONPlease completecomplete allall questionsquestions below.below. OmittedOmitted informationinformation willwill causecause delays.delays. InIn thisthis section,section, “you”“you” andand “your”“your” refersrefers toto thethe personperson forfor whomwhomPleaseinsurance isis beingbeing requested.requested.insuranceAuxiliaryAuxiliary MemberMember HeightHeightfeetfeetinchesinches WeightWeightpoundspounds1.1. PersonalPersonal Physician’sPhysician’s Name:Name:DateoflastvisitReasonDate of last visit (MM/DD/YYYY):(MM/DD/YYYY):Reason forfor ons?YesNoIfyes,listthemedications2. Are you currently taking any prescribed medications?YesNo If yes, list the e:Prescribing Physician’s nalmedications.Check here if you are attaching another sheet for any additional medications.ZipZip CodeCodeZipZip CodeCodeTelephone:Telephone: ((Telephone:Telephone: (())--))--AuxiliaryAuxiliaryMemberMemberForFor questionsquestions 33 throughthrough 6,6, forfor “yes”“yes” answers,answers, pleaseplease provideprovide fullfull detailsdetails inin thethe sectionssections below.below.3. HaveHave youyou hadhad anyany applicationapplication forfor life,life, accidentalaccidental deathdeath andand dismembermentdismemberment oror disabilitydisability ated;modified; ororissued otherother thanthan asas appliedapplied for?for?4. InIn thethe pastpast 55 years,years, havehave youyou beenbeen convictedconvicted ofof drivingdriving whilewhile intoxicatedintoxicated oror underunder thethe influenceinfluence ofof alcoholalcohol and/orand/or anyany drug?drug?4.IfIf “yes”,“yes”, specifyspecify ”date(s)”date(s) ofof conviction(s)conviction(s) (month/day/year)(month/day/year)5. ForFor residentsresidents ofof allall statesstates exceptexcept CT,CT, pleaseplease answeranswer thethe followingfollowing question:question: HaveHave youyou everever beenbeen diagnoseddiagnosed oror treatedtreated byby aa5.physicianphysician oror otherother healthhealth carecare providerprovider forfor AcquiredAcquired ImmunodeficiencyImmunodeficiency SyndromeSyndrome (AIDS),(AIDS), AIDSAIDS RelatedRelated ComplexComplex (ARC)(ARC) oror thethe HumanHumanImmunodeficiency VirusVirus (HIV)(HIV) infection?infection?ImmunodeficiencyFor CTCT residents,residents, pleaseplease answeranswer thethe followingfollowing question:question: ToTo thethe bestbest ofof youryour knowledgeknowledge andand belief,belief, havehave youyou everever beenbeen diagnoseddiagnosedFororor treatedtreated byby aa physicianphysician oror otherother healthhealth carecare providerprovider forfor AcquiredAcquired ImmunodeficiencyImmunodeficiency SyndromeSyndrome (AIDS),(AIDS), AIDSAIDS RelatedRelated ComplexComplex (ARC)(ARC)oror thethe HumanHuman ImmunodeficiencyImmunodeficiency VirusVirus (HIV)(HIV) infection?infection?6.6. HaveHave youyou everever beenbeen diagnosed,diagnosed, treatedtreated oror givengiven medicalmedical adviceadvice byby aa physicianphysician oror otherother healthhealth carecare providerprovider for:for: cardiaccardiac ororcardiovascular disorder;disorder; strokestroke oror circulatorycirculatory disorder;disorder; highhigh bloodblood pressure;pressure; cancer;cancer; bloodblood disorder;disorder; diabetes;diabetes; lunglung disease;disease; liverliver ororcardiovascularintestinalintestinal disorder;disorder; mentalmental illness,illness, anxiety,anxiety, depression,depression, attemptedattempted suicidesuicide oror nervousnervous sYesNoNoGEF09-1GEF09-1HEAHEA(The(The formform numbernumber aboveabove appliesapplies toto residentsresidents ofof allall statesstates exceptexcept asas follows:follows: FormForm numbernumber GEF09-1GEF09-1 appliesapplies toto residentsresidents ofof Montana;Montana;GEF09-1GEF09-1HEA appliesapplies toto residentsresidents ofof Connecticut,Connecticut, NorthNorth DakotaDakota andand Utah)Utah)HEAPage 22 ofof 44PageMBA –ENROLL-Auxiliary–ENROLL-Auxiliary MemberMember (12/18)(12/18)MBAInitialInitial SSN#SSN# (Last(Last 4)4)
For questions 7 and 8, for “yes” answers, please provide full details in the sections below.Forand 8,for you“yes”answers,pleaseasprovidedetailsthe sectionsbelow.7. Inquestionsthe past 5 7years,havebeenHospitalizeddefinedfullbelow(not ionfor inpatientcare asin adefinedhospital;receiptcare in awell-babyhospice facility,intermediate care facility, or long termYesNo7. HospitalizedIn the past 5 years,you beenHospitalizedbelow(notofincludingdelivery)?care facility; or receipt of the following treatment wherever performed: chemotherapy, radiation therapy, or dialysis.Hospitalized means admission for inpatient care in a hospital; receipt of care in a hospice facility, intermediate care facility, or long term8. careIn thefacility;past 5oryears,haveyoufollowingbeen diagnosed,or givenmedicaladvice by a physicianother healthcare provider for any otherreceiptof radiationortherapy,or dialysis.medical condition or had a surgical procedure (other than oral surgery)?YesNo8. In the past 5 years, have you been diagnosed, treated or given medical advice by a physician or other health care provider for any otherPleaseprovidefull detailsfor or had belowa surgicalprocedurethantooralsurgery)?3 through 8.YesNoIf you need more space to provide full details, attach a separate sheet with the information and sign and date it. Delays in processing your application swertoquestions3through8.occur if complete details are not provided. MetLife may contact you for additional or missing information.If you need more space to provide full details, attach a separate sheet with the information and sign and date it. Delays in processing your application mayoccur if complete details are not provided. MetLife may contact you for additional Pleaseor missinginformation.list anymedication prescribed that is not already identified inQuestion Number(s)Condition/DiagnosisSection 7 Question 2Please list any medication prescribed that is not already identified inQuestion Number(s)Condition/DiagnosisSection 7 Question 2Date of Diagnosis (MM/YYYY)Date of Last Treatment (MM/YYYY)Type of TreatmentDate of Diagnosis (MM/YYYY)Date of Last Treatment (MM/YYYY)Type of TreatmentTreating Health ProfessionalPhysician’sName:Treating HealthProfessionalDateof last Name:visit:Physician’sReason for visit:AddressDateof last visit:StreetAddressGEF09-1StreetReason for visit:CityStateZip CodeCityStateZip CodeTelephone: ()-Telephone: ()-HEA-SUPPGEF09-1(The form number above applies to residents of all states except as follows: Form number GEF09-1 applies to residents of Montana;HEA-SUPPGEF09-1(Theform numberappliesoftoConnecticut,residents of allstatesexceptfollows: Form number GEF09-1 applies to residents of Montana;HEA-SUPPappliesaboveto residentsNorthDakotaandasUtah)GEF09-1HEA-SUPP applies to residents of Connecticut, North Dakota and Utah)SECTION 7 – Fraud WarningsBeforesigning 7this–enrollmentform, please read the warning for the state where you reside and for the state where the insurance policy under which you areSECTIONFraud Warningsapplying for coverage was issued. Alabama, Arkansas, District of Columbia, Louisiana, Massachusetts, New Mexico, Ohio, Rhode Island and WestBefore signingthis enrollmentform, pleasereada thefor the claimstate forwhereyou resideandorforbenefitthe statewhere thepresentsinsurancefalsepolicyunder whichVirginia:Any personwho knowinglypresentsfalsewarningor fraudulentpaymentof a lossor knowinglyinformationin anyou areapplying forforcoveragewasis sachusetts,RhodeprovideIsland andapplicationinsuranceguilty of Alabama,a crime andmay be subjectfinesand confinementin prison.Colorado:NewIt is Mexico,unlawful Ohio,to knowinglyfalse,WestVirginia: Anyperson whofactsknowinglypresentstoaanfalseor fraudulentclaimforforthepaymentloss or benefitor knowinglypresentsthefalseinformationin an mayincompleteor misleadingor informationinsurancecompanypurposeofofa defraudingor attemptingto defraudcompany.Penaltiesapplicationfor insuranceis guiltyof ofa crimeand maybe subjectto finesconfinementin prison.Colorado:It is unlawfulto fines,denialinsuranceand civildamages.Anyandinsurancecompanyor agentof an insurancecompanywho knowinglyincompleteor misleadingfacts orfactsinformationto an insurancecompanythe purposedefraudingor attemptingto defraudtothecompany.Penalties mayfalse,incomplete,or misleadingor informationto a policyholderor forclaimantfor theofpurposeof defraudingor attemptingdefraudthe policyholderorinclude imprisonment,denial oforinsuranceand civildamages.insuranceor agentan insurancecompanywho knowinglyclaimantwith regard tofines,a settlementaward payablefrominsuranceAnyproceedsshallcompanybe reportedto theofColoradoDivisionof Insurancewithin theprovidesfalse, incomplete,or misleadingfactsFlorida:or informationto a whopolicyholderor andclaimantfor thetopurposeof defraudingor attemptingto defraudthe policyholderorDepartmentof RegulatoryAgencies.A personknowinglywith intentinjure, defraudor deceiveany insurancecompanyfiles aclaimant withregardortoana applicationsettlement containingor award payablefrom insuranceproceedsinformationshall be reportedColoradoDivisionof Insurancewithinstatementof claimfalse, incompleteor misleadingis guiltytoofthea felonyof thethird degree.KansasandtheOregon:Departmentof RegulatoryA personwho knowinglyand with intentto injure, maydefraudor deceiveany insurancefilessubjectaAnyperson whoknowinglyAgencies.presents aFlorida:materiallyfalse statementin an applicationfor insurancebe guiltyof a criminaloffense companyand may betostatementof claimor law.an iltyof a felonyof the thirddegree.KansasOregon:penalties understateKentucky:containingAny personwhoknowinglyorandwith intentto defraudisanyinsurancecompanyor otherpersonfiles falsepresentsa materiallyfalse statementin an applicationfor insurancemaybe guilty anyof a factcriminaloffenseand commitsmay be subjecttocontaininginformationor conceals,for the purposeof misleading,informationconcerningmaterialtheretoa fraudulentpenaltiesstate islaw.Kentucky:person whoand withto defraudany insurancecompanyor otherfiles informationan applicationinsuranceunderact, whicha crime.Maine,AnyTennesseeandknowinglyWashington:It isintenta crimeto knowinglyprovide false,incompleteor personmisleadingto ancontaining companyany materiallyinformationor conceals,for the purposeof misleading,informationconcerninganyfact materialtheretobenefits.commitsMaryland:a fraudulentinsurancefor thefalsepurposesof defraudingthe company.Penaltiesmay includeimprisonment,fines ora denialof insuranceinsurancewhichis a crime.Maine,presentsTennesseeandIt iscrime to ofknowinglyinformationAnypersonact,whoknowinglyor willfullya falseor Washington:fraudulent claimforapaymenta loss orprovidebenefit false,or whoincompleteknowinglyorormisleadingwillfully presentsfalse to aninsurance companyfor the purposesof defraudingthea company.Penaltiesmay includefinesa denialof Jersey:insuranceAnybenefits.informationin an applicationfor insuranceis guilty ofcrime and maybe subjectto finesimprisonment,and confinementin orprison.NewpersonMaryland:who files anAny personcontainingwho knowinglyor willfullypresentsinformationa false or fraudulentfor paymenta loss or benefitor whowillfully presentsfalseapplicationany falseor misleadingis subject claimto criminaland civilofpenalties.New York(onlyknowinglyapplies toorAccidentand ndfor withinsuranceof aanycrimeand maybe subjectto finesand filesconfinementin prison.New Jersey:Any personwho files anAnyperson inwhointent isto guiltydefraudinsurancecompanyor otherpersonan applicationfor insuranceor statementof ,or misleadinginformationsubjectto criminaland civilinformationpenalties. concerningNew York (onlyappliesto AccidentHealtha Benefits):containing anymateriallyor concealsforisthepurposeof misleading,any factmaterialthereto,andcommitsfraudulentAny personact,whoknowinglyand withto defraudany toinsurancecompanyother personfiles an applicationor statementof claiminsurancewhichis a crime,and intentshall alsobe subjecta civil penaltynot orto exceedfive thousanddollars andfortheinsurancestated valueof the claimfor eachcontainingany Oklahoma:materially falseinformation,concealsforknowingly,the rialmakesthereto,fraudulentsuch violation.WARNING:Anyorpersonwhoandofwithintent toinformationinjure, defraudor deceiveanycommitsclaim fora theinsurance ofact,is a crime,shall alsosubjectto a civilorpenaltynot toinformationexceed fiveisthousandthe statedof the claimfor eachproceedsanwhichinsurancepolicy andcontaininganybefalse,incompletemisleadingguilty of adollarsfelony.andPuertoRico: valueAny personwho knowinglysuchviolation.Oklahoma:WARNING:who knowingly,and withforintentto injure,defraudor deceiveinsurer,any claimfor theand withthe intentionto defraudincludesAnyfalsepersoninformationin an applicationinsuranceor files,assistsor abetsanyin thefiling makesof a fraudulentclaimto obtainproceedsofofaanlossinsurancecontainingany false,incompletemisleadingis commitsguilty of aa felony.PuertoRico:guiltyAnyshallpersonwho knowinglypaymentor otherpolicybenefit,or files morethan oneclaim fororthesame lossinformationor damage,felony andif foundbe punishedfor eachand with withthe intentionincludesfalse informationin an applicationfor insuranceor files,assistsor abetsorinimprisonedthe filing offora fraudulentto obtainviolationa fine of tonodefraudless thanfive thousanddollars ( 5,000),not to exceedten thousanddollars( 10,000);a fixed termclaimof three(3)paymenta lossor other benefit
Conversion Privilege Members have a conversion privilege upon the occurrence of certain events, including upon termination of group coverage, at age 70, to an individual policy of life insurance with MetLife, as explained in the certificate of coverage. Exclusion of coverage. Instead, the premium will be refunded. Cancellation Protection .