Transcription
University of Michigan Health SystemMedSport Staffing & Scheduling AnalysisFinal ReportClient:Julie Agbabian, Interim Operations Management, MedSportCoordinator:Richard Coffey, Director, Programs and Operations AnalysisFrom:IOE 481 Project Team, Programs and Operations AnalysisBradley BelskyMike GrezlikAnne PiontekReid TatorisDate: April 19, 2004
Table of ContentsExecutive Summary 1Problem .1Findings .1Recommendations .2Introduction and Background . .3Key Issues . 3Scope . 3Approach and Methodology .3Preparatory Work .4Data Collection .4Current Situation 4Results 5Clinician Analysis 5Outpatient Office Assistant Analysis .6Scheduling Analysis .6Current State and Sensitivity Analysis 7Recommendations .8Appendix A: Data Collection Forms .9Appendix B: Linear Cominations .11Appendix C: Raw Data . 12
Executive SummaryProblemMedSport, the University of Michigan’s sports medicine therapy clinics, recently relocated to alarger facility and, at the same time, experienced a decrease in patient volume. Thesecircumstances may require changes in staffing of MedSport’s clinicians. These cliniciansinclude physical therapists (PT’s), athletic trainers (ATC’s), and personal trainer assistants(aides). The purpose of this project was to determine an optimal staffing level for MedSportclinicians, and to implement a model to schedule MedSport clinicians that will account for futurevariations in demand.MethodologyOur team flowcharted the patient process and developed a data collection strategy after fourmeetings with MedSport’s Interim Operations Manager, Julie Agbabian. Our team created datacollection forms and distributed them to the members of Team 4 and the OPOA with written datacollection instructions. A sample data collection form is attached in Appendix A.Team 4 collected patient data for two weeks, from February 10 through 23. An additional weekof data collection was performed from March 8 through 12. A total of 88 patient samples werecollected over both data collection periods. Our team was present at the MedSport facility toobserve Team 4 for two of the five days of this collection period, and recorded the data fromtwelve of the patients ourselves. This observation ensured there was no bias in the data collectedby Team 4.To verify that the data collected by Team 4 was representative of all MedSport teams, patientdata was collected from another MedSport Team (Team 1). This data was collected on March 26and was observed by the student team to validate the recorded data.FindingsData from 88 patients were collected between February 10 and March 12, 2004, by MedSportTeam 4. MedSport has five teams consisting of PT’s and ATC’s. Of these five teams, it wasdetermined that Team 4 would be the most responsive to data collection and therefore werechosen as the data collection team. During this period, the mean time spent by PT’s or ATC’sfor revisit patients was 34.4 minutes with a standard deviation of 18.7 minutes. The mean timespent by PT’s on new patients was 57 minutes with a standard deviation of 7.6 minutes. Finally,the mean time spent by PT’s on Medicare patients was 40 minutes with a standard deviation of8.7 minutes. Also, the clinicians spent an average of 3.7 minutes of additional time ondocumentation after the patient left the MedSport facility during this period.Through the use of linear combinations, the expected total time and variance spent with patientsby PT’s and ATCs was determined, forming the basis for our model. Based on MedSport’spatient database, it was determined that their current patient volume was 100 visits per day, re1
visit to new patient ratio was 7.5:1, and Medicare patients made up 5% of total patients. Basedon this data, the model we constructed shows that there should be 238 PT hours and 217 ATChours per week. To maintain the current staffing ratio, MedSport should have 145 patients perday.RecommendationsCurrently, MedSport has 342 PT hours and 314 AT hours per week in comparison to the 238Physical Therapist hours and 217 Athletic Trainer hours per week suggested by the model. Thisstaffing schedule indicates that MedSport is overstaffed by 104 PT hours and 97 AT hours perweek (assuming there are zero sick and vacation hours during the week). Given this, we suggestthat MedSport either reduce the total number of Physical Therapist and Athletic Trainer hoursthrough the expansion of the high school outreach program or increase their patient volume to145 patients per day if MedSport wishes to continue at their current staffing level.2
Introduction and BackgroundMedSport is the home of the University of Michigan sports medicine clinic. They are a physicaltherapy clinic whose objective is to provide complete orthopedic care to athletes of all interests,levels and ages.Currently, MedSport employs 28.5 Full-Time Equivalences (FTE’s), 9.6 of which are PT’s.MedSport has five teams at the Domino’s Farms facility. Each team consists of one to two PT’sand one to three ATC’s. MedSport also employs aides as support staff to provide extraassistance to teams. Only a PT can see new patients or those with Medicare insurance. ATC’scan perform all other tasks of a PT under direct supervision by a PT. On average, MedSport seesabout 100 patients per day, ten to eleven of which are new patients. Patients seen by PT’s arebilled in 15-minute increments (billed by units).Recently, MedSport expanded from a 10,000-square-foot facility to a 45,000-square-foot facilityat Domino’s Farms on Plymouth Road at the north side of Ann Arbor. At the same time, theclinic experienced a decrease in patients, largely due to new insurance company restrictions. Forexample, beginning in January 2003, M-Care requires patients to pay a 15 co-pay for each visit.This additional cost to patients is partly responsible for the decrease in patient volume.Decreased patient volume has led to financial concerns for MedSport, which have forced them toevaluate their patient-to-employee ratios and their employee scheduling process.These circumstances require changes in the utilization of MedSport’s physical therapists (PT’s),athletic trainers (ATC’s), and personal trainer assistants (aides). MedSport has identified a needto evaluate their scheduling practices for their employees due to the transition to a new facilityand the decrease in operating margin. Thus, the Interim Operations Manager is concerned thatMedSport may be overstaffed. Therefore, the purpose of this project was to determine anoptimal staffing level for MedSport clinicians and to implement a scheduling model that willaccount for future variations in demand. The purpose of the report is to discuss the findings ofthe student team and review the methodology used to obtain their results.Key IssuesThe following key issues drove the need for this project. A decrease in the number of patients A decrease in operating margin MedSport’s perception that the facility may be overstaffedScopeProject Included: MedSport facility at Domino’s Farms only3
Physical Therapist (PT), Athletic Trainer (ATC) , aide, and Out Patient Office Assistant(OPOA) functionsProject Excluded: MedSport facilities at the Ice Cube, Brighton, and Livonia locations Medical Doctor (MD) functions Golf Fit clinicApproach and MethodologyPreparatory WorkFollowing four meetings with Julie Agbabian, the Interim Operations Manager at MedSport, ourteam flowcharted the patient process and developed a data collection strategy. The client choseto focus data collection on Team 4 (comprised of three physical therapists and two athletictrainers), and the Out Patient Office Assistants (OPOA) for MedSport’s staffing and schedulingproject. Ms. Agbabian perceived Team 4 to be most representative of the teams at MedSport.Also Ms. Agbabian briefly discussed their role in the patient data collection process. Our teamcreated data collection forms and distributed them to the members of Team 4 and the OPOA withwritten data collection instructions. .Data CollectionData was entered by each member of Team 4 to log the amount of time PT’s and ATC’s spentwith each type of patient. A sample data collection form is attached in Appendix A. Team 4 andthe OPOA collected patient data for two weeks, between February 10 and 23. Team 4 recordeddata from 51 patients and the OPOA recorded data from 91 patients during that time. Anadditional data collection period was held for one week, between March 8 and 12, where Team 4patient data was again collected. This period yielded data from 37 patients. Our team waspresent at the MedSport facility to observe Team 4 for two of the five days of this collectionperiod, and recorded the data from twelve of the patients ourselves. The purpose of thisobservation was to verify there was no bias in the data self-collected by Team 4.To verify that the data collected by Team 4 was representative of all MedSport teams, patientdata was collected from another MedSport Team. The team chosen to verify this data wasMedSport Team 1. This data was collected on March 26 and was observed by the student teamto validate the recorded data.4
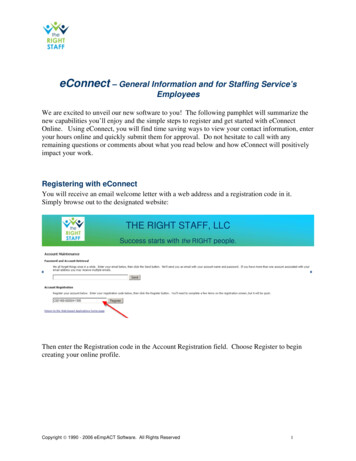
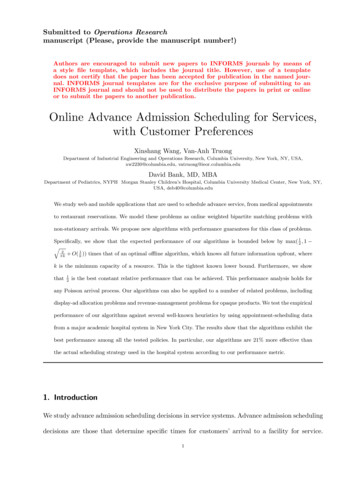
ResultsClinician AnalysisData was collected from February 10 through 23 and from March 8 through 12 by MedSportTeam 4. Over this period, 88 samples were collected, of which 74 were re-visits. Theproportion or re-visits to total visits is consistent with patient data provided from the client’spatient database. Figure 1 displays the total time spent with each re-visit patient by PhysicalTherapists and Athletic Trainers. Time spent with the patient by aides is being ignored as theyonly spent time with four patients.Figure 1: Total time spent (min) per re-visit patient by Physical Therapists and Athletic TrainersThis data displayed in Figure 1 is approximately normal as determined by the Anderson-Darlingnormality test (A-Squared is .800) and will be analyzed using the normal distribution. Pointestimates for the mean and standard deviation are 34.4 minutes and 18.7 minutes respectively.The point estimates were validated by both samples from Team 1 as well as samples taken by thestudent team. Neither of these additional samples have statistically significant deviation from themain data set.Of the 74 patients, Athletic Trainers saw 51 while 32 were seen by Physical Therapists (somewere seen by both). Table 1 shows the time spent per patient by clinician type.5
Table 1: Time spent with patient by clinician typeSample Size Average PTStandardSeen by(min)Time (min) Deviation (min)PT Only2337.823.0AT Only42PT and AT910.76.5Average ATTime (min)33.121.1StandardDeviation (min)17.513.0The time spent per patient is distributed approximately normally in all three cases for time spentby both Physical Therapists as well as Athletic Trainers (verified by Anderson-Darling). Theanalytical tools for the normal distribution are well-developed, making the analysis muchsimpler.The remaining patients were either Medicare patients or new patients. These differ from re-visitsin that only Physical Therapists can work with the patient. Table 2 shows the amount of timespent with each patient by the Physical Therapist.Table 2: Average time spent PT’s by patient typeStandardPatientAverage TimeDeviationTypeSpent (min)(min)New Visit57.07.6Medicare40.08.7Although the sample size for each is small relative to re-visits, the standard deviation is small.Thus, confidence in the average time spent is high. Additionally, time spent per patient isdistributed approximately normally (verified by Anderson-Darling).Both PT’s and ATC’s spend additional time on documentation after the patient leaves MedSport.The average time spent on documentation is 3.7 minutes. Analysis was done by patient type, anddifferences were found to not be statistically significant from the overall mean.Outpatient Office Assistant AnalysisFrom the 88 patients sampled, 44 met with an outpatient office assistant (OPOA) after their visit.The total time spent with all 88 patients by the OPOA’s over the data collection period was 28minutes. Given this, the number of patients seen by an OPOA in a given day has a negligibleeffect on their workload.Scheduling AnalysisThe average time spent per patient can be determined through the use of linear combinations.The mathematical theory for linear combination is presented in Appendix B. Using this, theexpected total time and variance spent with patients by Physical Therapists and Athletic Trainerscan be determined.6
From factory physics, variability will degrade the performance of the system 1 . Therefore,MedSport must include a buffer over what is required from the expected total time. The datacollected suggests that MedSport has a low coefficient of variation (defined as the ratio of thevariance of a system to the expected time squared). Looking at simulations with low coefficientsof variation and other parameters similar to MedSport, a buffer of 15% above the expected totaltime will make up for degradation of the system due to variability.Additionally, break time and meetings must be included to determine the optimal number ofPhysical Therapist and Athletic Trainer FTE’s. The total time (which includes two 15-minutebreaks and one half hour lunch) must be increased by an additional 15% to determine the totalnumber of FTE’s needed on-site. This additional buffer yields a total of a 30% buffer tocompensate for variability in the system.Current State and Sensitivity AnalysisUsing MedSport’s current patient volume of 100 patients per day, re-visit to new patient ratio
19.04.2004 · MedSport facilities at the Ice Cube, Brighton, and Livonia locations Medical Doctor (MD) functions Golf Fit clinic Approach and Methodology Preparatory Work Following four meetings with Julie Agbabian, the Interim Operations Manager at MedSport, our team flowcharted the patient process and developed a data collection strategy. The client chose to focus data collection on Team 4 .