Transcription
Neuropsychological EvaluationGeoffrey Tremont, Ph.D., ABPP-CNRhode Island Hospital & Alpert MedicalSchool of Brown University
Outline of Talk Neuropsychology DefinitionTraining in NeuropsychologyPurpose of a Neuropsychological EvaluationApproaches and MethodsNormative DataDeficit MeasurementComponents of an EvaluationCognitive Domains
Outline Continued Neuropsychological ReportNormal Cognitive AgingMild Cognitive ImpairmentDementiaDepression-Related Cognitive Dysfunction
Neuropsychology Definition Study of brain-behavior relationships– Cognition– Mood– Functional ability Observation and formal assessment toidentify CNS integrity
Training In Neuropsychology Clinical Psychology PhD (PsyD, EdD)Neurology, neuroanatomy, neuroscienceSpecialized training internship & fellowshipLicensed as clinical psychologistBoard Certification not standard like medicine– American Board of Clinical Neuropsychology(ABCN)– American Board of Professional Psychology(APN)
Purpose of NeuropsychologicalEvaluation Pattern of overall cognitive and behavioralfunctioning (strengths and weaknesses) Differential diagnosis (e.g., dementia v.depression) Cognitive change following neurologicdisorder, head injury, or surgery Disability determination, competency, orother litigation Baseline for later comparison
Purpose of NeuropsychologicalEvaluation cont. Track progression of degenerativediseases Recommendations about placement,medications, other testing/diagnosticprocedures, behavioral interventions,cognitive rehabilitation, and safetyconcerns
Approaches and Methods Fixed battery approachFlexible approach/Hypothesis TestingProcess approachMost use a combined core battery withflexibility 100’s of tests and batteries
Normative Data To identify areas of impairment need ahealthy reference group Need to consider demographics factors thatcan affect performance – age, education,gender, race Compare performance to normative data Premorbid ability estimation– Regression based (Barona equation)– Ability based (Wechsler Test of Adult Reading)
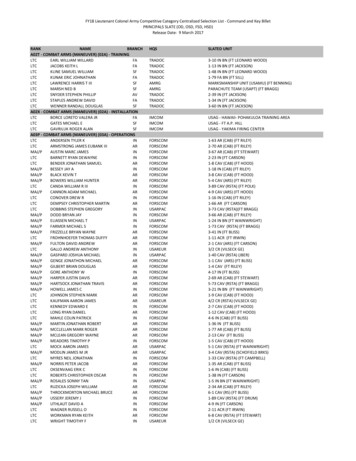
Deficit Measurement Different standard scores used (IQ, Tscores, z-scores, scaled scores, percentiles) Impairment defined by– 1-2 SD below mean (Mild)– 2-3 SD below mean (Moderate)– 3 SD below mean (Severe) Interpret in context of premorbid ability
Normal Distribution
Components of Examination Medical record review Clinical interview – medical, social,psychological, educational history Collateral interview – especially important indementia Behavioral observations/Mental status Motivational/Effort Testing
Motivation and Effort Detection of exaggeration and malingeringis important when there is potentialsecondary gain Performance validity testing – Test ofMemory Malingering, Word MemoryTesting Symptom validity - Minnesota MultiphasicPersonality Inventory – 2 (Validity Scales,Fake Bad Scale) – medical & psychmalingering/exaggeration
Cognitive Domains Intellectual/Academic/Global CognitionAttentionProcessing SpeedExecutive FunctioningLanguage & Related FunctionsVisuospatialLearning and MemoryMood and BehaviorSensory/Perceptual/Motor
Intellectual/AchievementGlobal Cognition IQ tests provide a measure of overallcognitive strengths and weaknesses Academic achievement testing useful forlearning disorders Global cognitive measures can be used forscreening or tracking progression of disease MMSE (1-2-point decline per year indementia) – generally insensitive toexecutive dysfunction Mattis Dementia Rating Scale (14-pointdecline per year in dementia)
Attention CapacitySustainedSelectiveExamples: Digit SpanDisorders: Delirium, ADHDTypically preserved in dementia
Processing Speed Psychomotor Information Processing Examples: Trail Making Test A, PacedAuditory Serial Addition Test Disorders: Multiple Sclerosis, Parkinson’sdementia, cerebrovascular disease
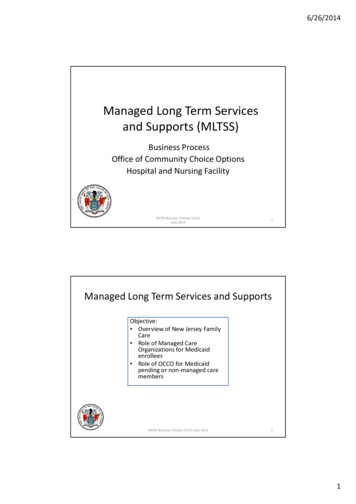
Executive Functioning Problem solving & bstractionInitiation/Perseveration/Personality ChangeExamples: Similarities, Stroop Test, Trail MakingTest B, Wisconsin Card Sorting Test, VerbalFluency Disorders: Frontotemporal Dementia, Traumaticbrain injury
Stroop Color-Word TestRedBlueBlueGreenGreenRed
Language & Related Functions ticExamples: Boston Naming TestDisorders: stroke, primary progressiveaphasia (Frontotemporal dementia)
Visuospatial Skills PerceptionConstructionMental rotationExamples: Clock Drawing Test, Judgmentof Line Orientation, Rey-OsterriethComplex Figure Disorders: right hemisphere stroke
Mild Cognitive Impairment
Alzheimer’s Disease
Lewy Body Dementia
Frontotemporal Dementia
Sensory/perceptual/motor Right-left orientationNeglectGrip strength/manual dexterityExamples: cancellation taskDisorders: stroke, brain tumor
Learning & Memory Learning/encodingFree recall/retrievalRetentionRecognition - DiscriminabilityExamples: Logical Memory, Hopkins VerbalLearning Test, Brief Visuospatial MemoryTest Disorders: Alzheimer’s disease, AlcoholInduced Amnestic Disorder (Korsakoff’sdisorder)
Memory Processes Encoding Process by which information is initiallyrecorded in a form usable to memory Storage Maintenance of material saved in thememory system Retrieval Material in memory storage is located,brought into awareness
Memory ConceptsShort-Term MemoryHolds information for 15 to 25 seconds (7 2items)RehearsalRepetition of information that has entered shortterm memoryChunkingUsed to expand ability to remember things inshort term; organize material into meaningfulgroups
Other Aspects of MemoryDeclarative MemoryFactual informationProcedural MemorySkills and habitsSemantic MemoryGeneral knowledge and facts about theworldEpisodic MemoryBiographical details of our individual lives
Forgetting & InterferenceDecayLoss of information through its nonusewhen new material is learned, a memory trace(engram) occursProactive interferenceInformation learned earlier interferes with recallof newer materialRetroactive interferenceDifficulty in recall of information because of laterexposure to different material
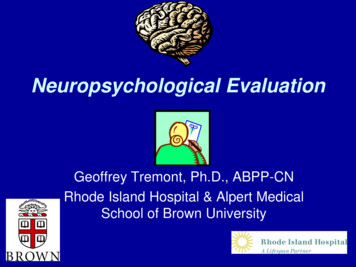
Anatomy of the Memory SystemSquire L , and Zola S PNAS 1996;93:13515-13522
Mood and Behavior AffectPersonalityMoodBehaviorExamples: Beck Depression Inventory,Minnesota Multiphasic PersonalityInventory, Frontal Systems Behavior Scale Disorders: Frontotemporal dementia, Lewybody dementia
Neuropsychological Report Serves as permanent record of patient’sperformance Differences among neuropsychologists– Length of report– History– Test scores– Diagnostic impressions– Recommendations
NEUROPSYCHOLOGY INAGING
Normal Aging Cognitive aging hypotheses– Right hemisphere– Frontal hypothesis– Fluid vs. Crystallized Intelligence Most changes are not dramatic Processing speed Stress, depression, medical illness, andmedications can contribute
Pathology/Physiology in Normal Aging Decrease in brain weight/volume Selective loss of neurons Declines in oxidative metabolism/accrualof oxidative stress Changes in adrenal/hormonal levels Changes in cerebrovascular supply Presence of AD pathology
Mild Cognitive Impairment Condition between normal aging and dementia Associated with an increased risk of developingdementia (10-15% per year) Healthly elderly (1-2% per year) 80% MCI may eventually develop dementia Decline in cognitive skills greater than 1.5 SDsbelow normative mean No impairment in ADLs - need good informant toestablish functional ability
Role of Neuropsychology in MildCognitive Impairment Establish level of impairment – Is it severeenough to meet the 1.5 SD threshold? Are there other problems (depression,medical illness) that explain problems? Identifying subtypes- amnestic, amnesticplus, single domain Monitor change at yearly intervals Evaluate the validity of informant report
Role of Neuropsychology inDementia Helpful in identifying pattern– Memory other functions – AD– Visuospatial other functions – Lewy Body– Frontal/Executive/Behavior other functions –FTD– Executive/slowing - subcortical (e.g.,Parkinson’s) Establish severity and track progression Determine response to treatment
Depression-Related CognitiveDysfunction Also referred to as pseudodementia ordementia syndrome of depression (may notbe appropriate terms) Depression is common in adults over 65(20%) Cognitive deficits associated withdepression are variable – almost never meetcriteria for dementia Deficits in visuospatial skills, executivefunctioning, & psychomotor speed
Depression-Related CognitiveDysfunction Depressed older adults with significantcognitive deficits may reflect a pre-dementiagroup – may not be responsive toantidepressants Late-life-onset depression may be differentthan early-life-onset – could reflect brainchange –prodromal dementia Deficits should improve with effectiveantidepressant treatment and/orpsychotherapy
Depression-Related CognitiveDysfunction Depression early in life increases risk forlate-life dementia MCI depression more likely to convert todementia than MCI alone AD depression (30-40%) greatercognitive impairment and faster declinethan AD alone
Cognition & ADL Performance Cognition is weakly to moderately associated withfunctional status (explains about 20% of variance) Medication management, finances, and telephone usehave highest correlations with cognition Similar correlations between cognition and ADLs andIADLs Executive functioning has strongest relationship withfunctional status (3x memory) Screening tests (MMSE, Mattis DRS) have strongerrelationships with functioning than most formalneuropsychological measures Behavior change also shows a strong relationship withfunctional status
When to Refer Older Adults forNeuropsychological Evaluation Dementia versus depression Perform below expectations on screeningtest Reports from patient and family member ofrepetitious speech or behavior Change in ADL performance
Conclusions Neuropsychological evaluation providesdetailed study of brain-behaviorrelationships Important component of work-up for MCIand dementia Careful consideration of premorbid abilities Pattern analysis can be helpful indifferentiating MCI/dementia type
Questions?
recorded in a form usable to memory . memory system Retrieval Material in memory storage is located, brought into awareness Memory Processes . Short-Term Memory Holds information for 15 to 25 seconds (7 2 items) Rehearsal . Late-life-onset depression may be different than early-life-onset - could reflect brain .