Transcription
PDF hosted at the Radboud Repository of the Radboud UniversityNijmegenThe following full text is a publisher's version.For additional information about this publication click this link.http://hdl.handle.net/2066/96373Please be advised that this information was generated on 2021-06-07 and may be subject tochange.
Original ArticleSuccess rate of miniplate anchorage for bone anchored maxillary protractionEline E. B. De Clercka; Gwen R. J. SwennenbABSTRACTObjective: To evaluate the success rate of Bollard miniplate anchorage for bone anchoredmaxillary protraction (BAMP).Materials and Methods: Twenty-five consecutive patients (mean age, 12.0 6 1.2 years; range,8.7–14.8 years) with maxillary hypoplasia without congenital or acquired deformation wereincluded in this study. A total of 100 Bollard modified miniplates were placed by the same surgeon.Ninety-nine miniplates were inserted under general anesthesia, and one was placed under localanesthesia because of initially soft bone conditions. Loading of the miniplates with 150 g elasticswas initiated at 17.5 6 6.9 days (range, 11–38 days) after surgery. Mean follow-up was provided at20.8 6 11.1 months (range, 6.5–46.2 months).Results: The overall success rate of miniplate anchorage in terms of stability was 97%. Duringorthodontic loading, five miniplates showed signs of mobility. After interruption of loading over 2 months,two miniplates became stable again. However, a total of three miniplates needed to be removed andwere successfully replaced under local anesthesia after a mean healing period of 3 months.Conclusion: Skeletal anchorage by means of Bollard modified miniplates is effective for BAMP.Success depends on proper presurgical patient counseling, minimal invasive surgery, goodpostsurgical instructions, and orthodontic follow-up. (Angle Orthod. 2011;81:1010–1013.)KEY WORDS: Miniplate anchorage; Bone anchored maxillary protraction; Success rateanchorage in the upper jaw.16–18 The first two modifiedmethods of maxillary protraction involved Le Fort Icorticotomy or osteotomy; the two latter protocols stillinvolved the use of a face mask.Over several years, bone anchored maxillary protraction (BAMP) without corticotomy or osteotomy withthe use of class III elastics between miniplate skeletalanchorage in the upper and lower jaw was introduced.19,20 With this approach, an extraoral face maskis no longer needed and intermaxillary traction can beapplied 24 hours a day. Preliminary studies based onconventional two-dimensional (2D) cephalometricanalysis21,22 and three-dimensional (3D) virtual treatment outcome analysis23 showed already very promising results. However, the stability and success rate ofminiplate anchorage for BAMP had not been investigated yet. Hence, the aim of this prospective studywas to evaluate the success rate of Bollard miniplateanchorage for BAMP in growing children.INTRODUCTIONCorrection of maxillary hypoplasia during growth byorthopedic maxillary protraction was pioneered byDelaire in the 1970s.1,2 The main disadvantages ofDelaire face mask therapy are noncompliance due todiscomfort, dentoalveolar compensation, and clockwise rotation of the mandible.3–6 To reduce these sideeffects, modified methods of maxillary protraction weredeveloped consisting of (1) maxillary distraction by arigid external distractor7–12; (2) maxillary distractionwith a face mask after Le Fort I corticotomy in cleftpatients13–15; and (3) face mask combined with skeletalaMedical student, Katholieke Universiteit Leuven, Belgium;research assistant, Division of Maxillo-Facial Surgery, Department of Surgery, General Hospital St-Jan Bruges, Rudershove,Bruges, Belgium.bProfessor, Division of Maxillo-Facial Surgery, Department ofSurgery, General Hospital St-Jan Bruges, Bruges, Belgium.Corresponding author: Professor Gwen R. J. Swennen, MD,LDS, DMD, PhD, FEBOMFS, Division of Maxillo-Facial Surgery,Department of Surgery, General Hospital St-Jan Bruges, Ruddershove 10, 8000 Bruges, Belgium(e-mail: gwen.swennen@azsintjan.be)MATERIALS AND METHODSThis prospective study was approved by theInstitutional Review Board of the AZ St-Jan Hospital.A total of 25 consecutive patients were included. Allpatients were referred for BAMP by four differentorthodontists (L.G.: n 5 4; T.B.: n 5 1; V.G.: n 5 1;Accepted: April 2011. Submitted: January 2011.Published Online: June 23, 2011G 2011 by The EH Angle Education and Research Foundation,Inc.Angle Orthodontist, Vol 81, No 6, 20111010DOI: 10.2319/012311-47.1
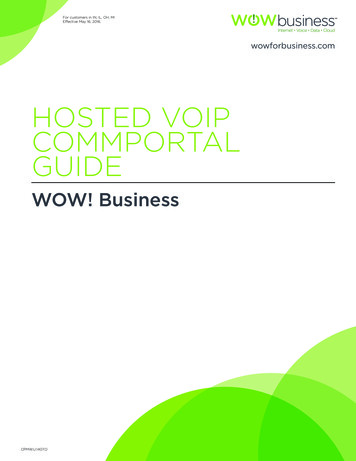
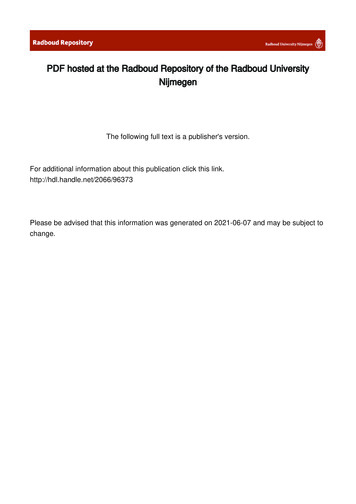
1011SUCCESS RATE OF MINIPLATE ANCHORAGE FOR BAMPFigure 1. Placement of Bollard modified miniplates for boneanchored maxillary protraction (BAMP). In this particular case, asquare wire was placed in the 0.018 3 0.025-inch tube of the lowerleft Bollard to slightly modify the vector of intermaxillary traction toavoid irritation of gingival soft tissues in the left lower jaw.and H.D.C.: n 5 19), and all presented with maxillaryhypoplasia and Angle Class III malocclusion. Nopatients had clefts, syndromes, or traumatic history.The mean age of patients at the time of surgery was12.0 6 1.2 years (range, 8.7–14.8 years). Seven male(mean age, 12.0 6 1.2 years; range, 10.7–14.8 years)and 18 female patients (mean age, 12.2 6 1.3 years;range, 8.7–13.7 years) were included.Presurgical patient counseling and surgery undergeneral anesthesia were provided in a one-day clinicvisit to all patients by the same surgeon. Althoughinsertion of four plates can be done under localanesthesia, young patients feel more comfortable witha procedure done under sedation or under a shortgeneral anesthesia. In all patients, the same miniplateanchorage system (Bollard Modified Miniplate, TitaLink, Brussels, Belgium) was placed in a standardizedway after a minimal invasive flap was raised, aspreviously described.24 In the upper jaw, ‘‘UpperBollards with hooks’’ were placed at the right and leftinfrazygomatic crest, while in the lower jaw, ‘‘LowerBollards with hooks’’ were placed on both sidesbetween the lower canine and the lateral incisor(Figure 1). In all patients, the Bollard miniplates werefixed with monocortical (5–7 mm length; 2.3 mmdiameter) Titamed Bollard Miniplate Screws (Titamed,Wervik, Belgium). Upper miniplates were fixed by threescrews, and two screws were used in the mandible(Figure 2). In the first six patients, self-tapping screwswere used, and in the following 19 patients, self-drillingscrews were applied. A single dose of IV antibiotics(amoxicillin and clavulanic acid) was given duringsurgery, but no corticosteroids were administered.Postsurgical instructions were given to all patients bythe same surgeon and by the referring orthodontist.Patients were instructed not to manipulate the miniplates with tongue or fingers. Loading of BollardFigure 2. The upper miniplate is fixed by three monocortical screwsat the infrazygomatic crest, and the lower miniplate with two screwsbetween the lateral incisor and the canine.modified miniplates with 150 g elastics was initiatedby the referring orthodontist 17.5 6 6.9 days (range,11–38 months) after surgery and was maintained for aperiod of 12 months. Mean follow-up was 20.8 611.1 months (range, 6.5–46.2 months).RESULTSIn 25 consecutive patients, 99 Bollard modifiedminiplates could be placed with excellent primarystability under general anesthesia. In one 12-year-oldmale patient, fixation of the upper miniplate at the rightinfrazygomatic crest with good primary stability wasnot feasible because bone conditions were soft. After abone healing period of 12 weeks, the upper miniplatecould be successfully fixed under local anesthesia. Inthe lower jaw, miniplates could be placed in all patientsbetween the lateral incisor and the canine.No infections occurred. Four patients, however,complained about irritation of the mucosa of thecheeks or lower lip at the first visit after surgery. Thiswas easily solved by covering the fixation unit of theminiplate with a small piece of soft wax, until edema ofthe soft tissues completely disappeared. The overallsuccess rate in terms of stability of Bollard miniplateanchorage was 97%. During orthodontic loading, fiveminiplates in five different patients showed signs ofmobility with small discomfort. In these cases, loadingwas interrupted for 2 months. After this period, twominiplates became stable again, and three miniplatesneeded to be removed and replaced under localAngle Orthodontist, Vol 81, No 6, 2011
1012anesthesia 3 months later. In two patients, fracture of ahook of the miniplate occurred and was solved byinsertion of a custom-made hook of a square wire inthe 0.018 3 0.025-inch tube of the fixation unit.DISCUSSIONFailure and success rates of miniscrews have beenwell investigated in the literature.25–29 Miniplates havebeen shown to be well accepted as skeletal anchorageby both patients and providers and have turned out tobe a safe and effective adjunct for complex orthodontictreatment.24 However, the success rate of miniplatesfor skeletal anchorage in orthodontics30–33 has not beeninvestigated so thoroughly as that of miniscrews, andresearch has been limited to adolescent and adultpatients. Compared with miniscrews and microscrews,miniplates showed greater stability.31 However, onlythe effect of continuous loading on miniplate stabilityhas been investigated. The forces generated byintermaxillary elastics are discontinuous in time,magnitude, and direction because of movements ofthe mandible during speech, chewing, and swallowing.To our knowledge, up to now no report has beenpublished on the failure rate of miniplates used formaxillary protraction by intermaxillary elastics in younggrowing patients. BAMP is the most critical procedureregarding stability and patient morbidity in the use ofminiplate anchorage in orthodontics. Initial mechanicalretention of osteosynthesis screws is mainly influencedby the thickness and density of the external corticalbone and is reduced in growing children comparedwith adult patients. In a prospective study on 200miniplates, most failures occurred in the youngestpatients.24 However, the mean age of patients in thisstudy was 24 years, and different miniplate designsand loading protocols were used.Results of this prospective study showed a highoverall success rate of 97%. All failures occurred in theupper jaw in contrast to reported higher failure rates ofminiscrews in the lower jaw.29,34–36 The latter data,however, were derived from clinical studies in olderpatients. Only a few studies37–39 have documented thesuccess rates of miniscrews in early teenagers. Also,in a retrospective study on the stability of 68miniplates, all failures were observed in the mandible.30 However, the patients were adults, the plates inthe lower jaw were inserted between the first andsecond molars, and the design of the plates complicated oral hygiene. All failures in our study occurred inthe youngest patients. The authors therefore proposenot to place miniplates for skeletal anchorage inorthodontics before the age of 11 years, because ofincreased risk of poor bone quality. No significantdifferences were observed in the stability of platesAngle Orthodontist, Vol 81, No 6, 2011DE CLERCK, SWENNENTable 1.Postsurgical Instructions to the Patienta,bCooling during 48 hoursSlight upright position during 48 hoursIncrease in blood pressure avoided during the first weekRinsing twice per day with chlorhexidine over 12 daysExtensive rinsing with sparkling water (5–10 times/d)NSAID over 3 daysOrthodontic loading of Bollard modified miniplates at approximately 14 days after surgeryN Manipulation of Bollard modified miniplates with tongue or fingersavoidedNNNNNNNabNo antibiotics are prescribed after surgery.NSAID indicates nonsteroidal anti-inflammatory drug.fixed by self-taping or self-drilling screws. Thereforethe authors recommend self-drilling screws, which areeasier to use.The high success rate in this study may be related toseveral factors: (1) presurgical counseling of thepatient, (2) minimal invasive surgery with decreasedpatient morbidity and adequate postsurgical instructions (Table 1), and (3) good orthodontic follow-up.Presurgical counseling is extremely important toprepare both young patients and their parents. Specialattention should be paid to the importance of avoidingrepetitive manipulation of the miniplates by tongue orfingers after surgery. Minimal invasive surgery consisting of small incisions, tunnel preparation, andgentle handling of the soft tissues is of majorimportance. Application of Elocom cream (mometasone furoate 1 mg) to the lips, additional localanesthesia (xylocaine 1% adrenaline) for vasoconstriction, and topical application of Exacyl (tranexamicacid) proved useful in decreasing postsurgical swellingand patient morbidity. Extensive rinsing with NaClduring surgery is important to avoid infection; application of wax to the miniplates at the end of surgeryproved very helpful in decreasing soft tissue irritation.Last but not least, good orthodontic follow-upconsisting of oral hygiene instructions and evaluationof miniplate anchorage (ie, local gingival status,mobility, hygiene, elastic force) is essential for treatment outcome.CONCLUSIONSN Miniplate anchorage with Bollard modified miniplatesis highly effective for bone anchored maxillaryprotraction (BAMP).N Success depends on proper presurgical patientcounseling, minimal invasive surgery, good postsurgical instructions, and orthodontic follow-up.ACKNOWLEDGMENTSThe authors thank the orthodontists T. Bataille, V. Geerinckx,L. Govaert, and H. De Clerck for their cooperation.
SUCCESS RATE OF MINIPLATE ANCHORAGE FOR BAMPREFERENCES1. Delaire J. Manufacture of the ‘‘orthopedic mask.’’ RevStomatol Chir Maxillofac. 1971;72:579–582.2. Delaire J. Treatment of Class III with dentofacial orthopedicmask. Acta Odontol Venez. 1979;17:168–200.3. Baik HS. Clinical results of the maxillary protraction in Koreanchildren. Am J Orthod Dentofacial Orthop. 1995;108:583–592.4. Kapust AJ, Sinclair PM, Turley PK.
plates with tongue or fingers. Loading of Bollard modified miniplates with 150 g elastics was initiated by the referring orthodontist 17.5 6 6.9 days (range, 11–38 months) after surgery and was maintained for a period of 12 months. Mean follow-up was 20.8 6 11.1 months (range, 6.5–46.2 months). RESULTS In 25 consecutive patients, 99 Bollard .