Transcription
UW PACCPsychiatry and Addictions Case ConferenceUW Medicine Psychiatry and Behavioral SciencesPRIMARY CARE MANAGEMENTOF OBESITYLYDIA CHWASTIAK MD, MPHASSOCIATE PROFESSORUNIVERSITY OF WASHINGTONDEPARTMENT OF PSYCHIATRY AND BEHAVIORAL SCIENCESMARCH 22, 2018UW PACC 2018 University of Washington
GENERAL DISCLOSURESThe University of Washington School ofMedicine also gratefully acknowledges receipt ofeducational grant support for this activity fromthe Washington State Legislature through theSafety-Net Hospital Assessment, working toexpand access to psychiatric services throughoutWashington State.UW PACC 2018 University of Washington
SPEAKER DISCLOSURES Nothing to discloseUW PACC 2018 University of Washington
OBJECTIVES1. Consider assuming a larger role in preventionand management of obesity, especiallyamong patients with serious mental illness2. Learn specific strategies for brief counselingwithin clinic visits3. Understand the effectiveness of behaviorallifestyle modification and pharmacologictreatments for obesityUW PACC 2018 University of Washington
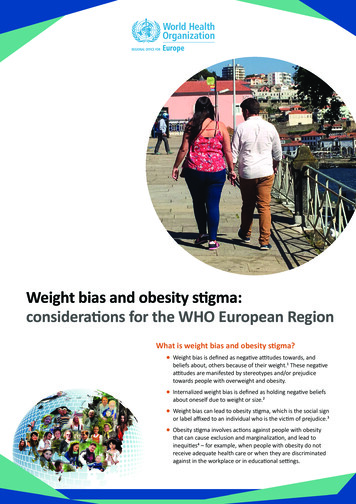
EPIDEMIOLOGY OF OBESITY 2011-2014: 68% of USadults are overweight;36.5% are obese2nd leading cause ofpreventable death 147 billion in htmlUW PACC 2018 University of Washington
APA/AMP 2017: Primary Care Skills for PsychiatristsDEFINITION OF OBESITYBMINIH 29.923-26.9ObesityClass I30-34.9 27Class II35-39.9Class III 40IdealWaist CircumferenceMaleFemaleNIH102cm88 cmAsianAmer90cm80 cmUW PACC 2018 University of Washington
EVIDENCE-BASED ent Patient and FamilyEducation BehavioralCounseling LifestyleModification ExerciseInterventions Diet Interventions Standardpharmacologictreatment AntipsychoticSwitchingAHRQ Publication No. 12-EHC063-EF; April 2013Surgical BariatricsurgeryUW PACC 2018 University of Washington
“5 A” APPROACHAssess Physical activity level Physical abilities Beliefs and KnowledgeAdvise Health risks Beliefs of change Appropriate “dose” of physical activityAgree Co-Develop personalized action plan Set specific physical activity goals based on interestsand confidence levelAssist Identify barriers and create strategies to addressthem Identify resources for physical activity and socialsupportArrange Specify plan for follow-up Check on progress/ maintenance of changeAuYoung, M., et al. Am J Med, 129(10), 1022-1029.UW PACC 2018 University of Washington
EXERCISE IS MEDICINE (2007) 2010 National Health Interview Survey: 1/3of all adults who visited a physician in the lastyear were advised by their physician to startor continue exercising EIM Goal: Physical activity assessment andexercise prescription a standard part of thedisease prevention for all patients Assess: Physical activity as a vital signBarnes, P. a. S., CA. (2012). Sallis, R. (2015). Phys Sportsmed, 43(1), 22-26.UW PACC 2018 University of Washington
“PRESCRIPTION FOR EXERCISE”Advise: 2-3 minutesPrescription Frequency Intensity Type Timea simple exercise prescription would be to advise the patientto walk 30 minutes at a brisk pace on 5 days each week.UW PACC 2018 University of Washington
UW PACC 2018 University of Washington
MAKE A SPECIFIC PLAN The more detailed the plan, the more likely it will befollowed. In the plan, consider: Date or days of the week– What time of day– How long– With whom– Other aspects that need to be planned Ask patient– How likely are you to do this?UW PACC 2018 University of Washington
BUILDING SUCCESS It’s an experiment, a trial, it’s notforever Suggest they act first and seewhat happens Praise any success they make Go slow and start small Reframing “failure” is essentialUW PACC 2018 University of Washington
COUNSELING ABOUT DIET 44 RCT, 18,000 participants– Outcomes Reduce saltReduce fatIncrease vegetablesIncrease fiberRees K, et.al. Cochrane 2013, Issue 12. CD002128.UW PACC 2018 University of Washington
CHOOSEMYPLATE.GOV Read the labels: compare sugar Make half your plate vegetables and fruits Vary your proteinUW PACC 2018 University of Washington
LIFESTYLE MODIFICATION Diabetes Prevention Program (n 3,234 at 27 centers)1 RCT, 3 arms: metformin, placebo, lifestyle modification– Training and support--Goals– loss of 7% of initial body weight– 150 minutes of physical activity per week Lifestyle group reduced 3-year risk of developingdiabetes by 58% (metformin by 31%) Widely disseminated intocommunity settings21Diabetes2AliPrevention Program Group, N Engl J Med 2002; 346(6): 393-403.MK et al. Health Affairs 2012; 31(1): 67-75.UW PACC 2018 University of Washington
EFFECTIVENESS IN SERIOUS MENTAL ILLNESS IN SHAPE (n 133)– Physical Activity, nutrition and smoking– Improved fitness at 3,6,9,12m ACHIEVE (n 291)– 18 months: individual group exercise, nutrition– 37.8% lost 5% IBW (compared to 22.7% of control, p 0.0009) STRIDE (n 200)– 12 months (6 6 months)– physical exercise, food records, personalized plans,cognitive strategies– 40% lost 5% BW c/w 17% controls (p 0.001) at 6 monthsDaumit GL et al. N Engl J Med 2013; 368: 1594-1602Green CA et al. Am J Psychiatry Am J Psychiatry. 2015 Jan;172(1):71-81Bartels SJ, et. al. Psychiatr Serv 2013; 64(8): 729-736UW PACC 2018 University of Washington
BEHAVIORAL WEIGHT LOSS INTERVENTIONSMost likely to be effective:Less likely to be successful: Longer duration (24 weeks) Manualized Combined education andactivity Both nutrition and physicalexercise Evidence-based (proveneffective by RCTs) Briefer duration interventions General wellness or healthpromotion education-only Non-intensive, unstructured,or non-manualizedinterventionsBartels S, et al. SAMHSA-HRSA Center for Integrated Health Solutions,2012UWPACC 2018 University of Washington
Metabolic Liability of MedicationsLow riskModerate riskHigh in M et al. Postgraduate Med 2013; 125 (5):Werneke U, Taylor D, Sanders TA. Curr Psychiatry Rep; 2013; 15: 347UW PACC 2018 University of Washington
SWITCH TO REDUCE METABOLIC RISK (CAMP)Weight change .5-3-3.0-3.5-3.5-4-44812162024Week of visitStroup TS, et al. Am J Psychiatry 2011; 168: 947-956UW PACC 2018 University of Washington
PHARMACOTHERAPYAgentEvidence in schizophreniaMetformin3 kg weight loss at 16 weeks1*Phentermine-TopiramateTopiramate: 5 kg weight glutide* FDA approval for weight lossJarskog LF, et al. Am J Psychiatry 2013; 170:1032-1040Das C, et al. Annals of Clinical Psychiatry 2012; 24(3): 225-239 /None /NoneUW PACC 2018 University of Washington
BARIATRIC SURGERY Indications based on current guidelines– Class III obesity (BMI 40 kg/m2)– Class II obesity (BMI 35-39.9) with medicalcomplication (DM, Sleep apnea)– Class I obesity with poorly-controlled T2 DM Mean BMI of those having procedures is 45NHLBI, NIH Publication No. 98-4083, 1998Buchwald H et al JAMA 2004; 292 (14): 1724-1737UW PACC 2018 University of Washington
BARIATRIC SURGERY Mean BMI of those havingprocedures is 45Months0-2Change in BMI Indications based on currentguidelines– Class III obesity (BMI 40kg/m2)– Class II obesity (BMI 3539.9) with medicalcomplication (DM, Sleepapnea)– Class I obesity with poorlycontrolled T2 DM036912-4Medical-6RYGB-8SG-10-12NHLBI, NIH Publication No. 98-4083, 1998Buchwald H et al JAMA 2004; 292 (14): 1724-1737Schauer PR, et al. N Engl J Med 2012; 366: 1567-1576UW PACC 2018 University of Washington
QUESTIONS?UW PACC 2018 University of Washington
2018 University of Washington . BARIATRIC SURGERY Indications based on current guidelines - Class III obesity (BMI 40 kg/m2) - Class II obesity (BMI 35 -39.9) with medical complication (DM, Sleep apnea) - Class I obesity with poorly -controlled T2 DM Mean BMI of those having procedures is 45