Transcription
SEPTEMBER 2012Research to Practice inSelf-DeterminationIssue 3:Self-Determinationand HealthLEARN ABOUT:The Role of SelfDetermination in ReducingHealth DisparitiesA Self-Advocate’s View ofHealth Self-ManagementSuccessful HealthPromotion StrategiesClinical Teaching Resourcesfor Training HealthProfessionalsPublished by theNational Training Initiativeon Self-Determination andthe Association of UniversityCenters on DisabilitiesFunded by U.S. Department of Health andHuman Services, Administration onDevelopmental Disabilities,grant no. 90-DD-0659Research to Practice inSelf-Determination SeriesIntroductionPeople who are self-determined make things happen intheir own lives. They know what they want and how to getit. They choose and set goals, then work to reach them. Theyadvocate on their own behalf, and are involved in solvingproblems and making decisions about their lives.The purpose of this series,Research to Practice in SelfDetermination, is to describe keyissues in the field of developmentaldisabilities that can be enhancedby considering efforts to promoteself-determination. Each issue isprepared with a social-ecologicalframework in mind. Thisframework calls for strategies forintervention and support to takeinto account both the capacitiesof the person and the demands ofthe environment. Interventionsto promote self-determinationshould focus on enhancing personalcapacity, improving opportunity,and modifying the environment.A series of seven issues will beproduced, each focusing on aspecific topic: self-advocacy,health, employment, communityservices, aging, family support, andsiblings. The format for these issueswill include definitions, a briefreview of the literature, promisingpractices, applied examples, andtargeted recommendations forscaling-up efforts. This series isintended for use by people withdevelopmental disabilities, familymembers, professionals, state andfederal agencies, and academicprograms. By collaboratingwith and enabling each of theseentities, the goal of full inclusionfor people with developmentaldisabilities can be realized.
Inside1Self-Determination and Health2The Role of Self-Determination in Reducing HealthDisparities Among People with Intellectual andDevelopmental Disabilities5Health Matters for People with Intellectual andDevelopmental Disabilities: Take Charge!7Special Olympics: From Health Disparities to AthleteLeadership Programs8Self-Determination, Technology and Health11My Health, My Choice, My Responsibility: A Curriculumto Promote Health Self-AdvocacyPublishers13Health Self-Management: A Self-Advocate’s ViewNational Training Initiativeon Self-Determination15Association of University Centerson DisabilitiesIn Our Own Words: Parents Advice on PromotingHealth Self-Advocacy for Individuals withDevelopmental Disabilities18Starting Early: Paving a Path Towards Interdependencein Health ManagementEditors20Healthy Relationships, Sexuality and Self-DeterminationAllen A. Schwartz, PhDBarbara Levitz, MSEdDavid O’Hara, PhDDonna M. Clark24The Physician’s Role in Promoting Health andSelf-Determination: An Interview with Dr. SherylWhite-Scott26Promoting Self-Determination in Oral Health28Hard Wired for Health: Clinical Teaching Resourcesfor Training Health Professionals to Promote SelfDetermination and More Effective Health Care forPeople with Intellectual and Developmental DisabilitiesLayoutCrystal PariseauThe National Gateway to Self-Determination Leadership Consortium Includes:Carl F. Calkins, PhD, Co-PI; Institute for Human Development, University of Missouri-Kansas CityMichael Wehmeyer, PhD, Co-PI; Lifespan Institute, University of KansasAnsley Bacon, PhD; Westchester Institute for Human Development, New York Medical CollegeTamar Heller, PhD; Institute on Disability and Human Development, University of Illinois, ChicagoHill Walker, PhD; Center on Human Development, University of Oregon
Self-Determination and HealthDavid O’Hara, PhDThis Research to Practice Guide willfocus on the potential of promotingself-determination in health whichhas only recently been explored as ameans of reducing the ongoing andsignificant health disparities experiencedby people with intellectual anddevelopmental disabilities (I/DD).The existence of persistent healthdisparities among people with I/DD wasfirst confirmed by the Surgeon General’s2001 report, Closing the Gap. Since then,the Healthy Athletes Program of SpecialOlympics has consistently demonstratedhigh levels of unmet health need in theareas of vision, hearing and dental care(Corbin, Holder & Hood, 2005). A recentstudy of Medicaid expenditure data foundthat people with I/DD were six times morelikely to have Type II diabetes than peoplewithout intellectual disabilities, as well ashaving an average of four other chronichealth problems (Reichard & Stolze, 2011).Until recently, health care strategiesto deal with these health disparitieshave tended to focus on better trainingfor primary care physicians, dentists,and other health care providers (Corbinet al., 2005) or the use of checklists bypractitioners to identify unmet healthneeds (Robertson, Roberts, Emerson,Turner, & Greig, 2011). Not untilthe international conference held atthe Westchester Institute for HumanDevelopment in 2003, was it suggestedthat promoting self-determination inhealth should be a key strategy in reducinghealth disparities. (Scheepers et al.,2005). Articles in this Guide by Vitale,and Marks & Sisarak describe some ofonly a limited number of projects thathave specifically focused on providingaccessible information, supports, and toolsdirectly to the person with I/DD or theircaregivers in order to achieve better health.This Research to Practice Guidereviews the current state-of-the-art effortsto reduce health disparities among peoplewith I/DD by increasing opportunitiesfor self-determination in their healthcare; that is, opportunities for healthself-management, self-advocacy, decision-making, and choice. It will describe thecurrent small body of research focusedon enhancing self-determination inhealth for people with I/DD, but will notbe limited by this. While existing formalresearch on the role of self-determinationin health might be incomplete, thisGuide will also tap into a more extensivebody of expert knowledge — from theexperiences of self-advocates, familymembers, and professionals — that isready to be translated into practice.Among the barriers to effectivehealth care is the issue of how well aperson understands and follows healthinstructions, usually defined as howhealth literate they are. But the Instituteof Medicine reported in 2010 that only12% of Americans have “proficient healthliteracy”; in other words, only 12% followhealth instructions well enough to achievebetter health care. So almost by definitionpeople with intellectual disabilities are notlikely to meet current standards of healthliteracy. This Guide explores existing anddeveloping practices that can support whatwe are calling “functional health literacy”for people who have reduced potential forachieving existing definitions of healthliteracy. Several articles describe successfulpeer-supported models of healthpromotion based upon curricula designedfor people with I/DD. Technology willalso play a significant role in supportingpeople with cognitive limitations tobecome more involved in their healthcare. The Guide includes an article byStock, Davies & O’Hara summarizingresearch underway to design health selfmanagement applications for direct use bypeople with I/DD, employing accessiblesmart technologies such as touch screentablets and mobile phones. Viewing healthliteracy as a behavioral concept, this articledescribes how prompting and coachingfeatures of smart technologies can helppeople with intellectual disabilitiesfollow healthy routines, for examplein nutrition and exercise, to alter theirlifestyles and achieve better health.Much of the “knowledge-to-practice”incorporated into the Guide comesfrom people with I/DD themselves andtheir families, who see opportunities forbetter health self-management, selfadvocacy, and self-direction in theircurrent experiences with the health caresystem. They are looking for organizedways to make their voices and opinionsheard in order to increase their personalinvolvement with, and control of, theirhealth care experiences. The Guidepresents several articles by self-advocatesand parents who share experiences abouthow to promote self-determination inhealth self-management. Recently, existinghealth care surveys have been translatedinto accessible formats for use by peoplewith I/DD, allowing them to express theirsatisfaction with the services they receiveand directly express their opinions aboutchoice- and decision-making in their dailylives (O’Hara, Davies, et al, 2010). . Usingcustomer feedback to improve servicesand health outcomes is an important trendin health care, and the ability of peoplewith cognitive limitations to provide suchfeedback, is a significant development.Good health for people withI/DD depends on successful ongoinginteractions between the personand caregivers with their health careteam. Therefore, training health careprofessionals to support people withI/DD in achieving health literacy andself-determination is another importanttopic covered in the Guide. Those whoeducate health care professionals havedeveloped training curricula and healthpractice guidelines to accomplish thesegoals. Specific competencies include; howto enhance the individual’s experienceswith health practitioners, skills foreffective communication, and methodsthat make it more likely that peoplewith I/DD will adopt better healthpromotion, wellness, and preventionactivities (See the articles by Vitale,and Marks & Sisarak). This Guide alsocontains articles by several practitionerswho describe their efforts to incorporateself-determination promotion into theirpractices. It describes several new andpromising curricula designed to enhanceNational Gateway to Self-Determination1
the skills of people with I/DD and thosewho support them, in working with theirhealth providers to become more activelyinvolved in their health management.Finally, the Guide brings a real lifeview and important perspective throughpersonal stories by people with I/DD,family members, and practitioners, aboutwhat works and what does not. Our taskis to create a climate for integrating whatwe know about individual empowermentand self-determination in health for peoplewith I/DD, with effective professionaltraining and a supportive environment.In this way, the health care communitywill be equipped with, and able to use,a range of effective communicationstrategies, cognitive and behavioralsupports, and adaptive technologiesto better engage people with I/DD intaking charge of their own health.ReferencesCorbin, S., Holder, M., & Hood, H. (2005).Changing attitudes, changing the world: Thehealth and health care of people with intellectualdisabilities. Washington, DC: Special Olympics.O’Hara, D., Davies, D., & Stock, S. (2011,November 28). Designing and using cloudbased interactive patient satisfaction, symptomreport and care management surveys to supportefficacy studies of new patient care pathways.Presentation to Royal Society of MedicineeHealth and Telemed Annual Conference,London, UK.Reichard, A., & Stolze, H. (2011). Diabetesamong adults with cognitive limitationscompared to individuals with no cognitivedisabilities. Journal of Intellectual andDevelopmental Disabilities, 49(30), 141-154.Robertson, J., Roberts, E., Emerson, E.,Turner, S., & Greig, R. (2011, November). Invitedreview: The impact of health checks for peoplewith intellectual disabilities: a systematic reviewof the evidence. Journal of Intellectual DisabilityResearch, 55(11), 1009-1019.Scheepers, M., Kerr, M., O’Hara, D.,Bainbridge, D., Cooper, S-A., Davis, R.,Fujiura, G., Heller, T., Holland, A., Krahn,G., Lennox, N., Meaney, J., & Wehmeyer, M.(2005, September/ December). Reducing healthdisparity in people with learning disabilities:A report from the health issues special interestresearch group of the International Associationfor the Scientific Study of Intellectual Disabilities.Journal of Policy and Practice in IntellectualDisabilities, 2(3/4), 249-255.Somers, S., & Mahadevan, R. (2010). Healthliteracy implications of the Affordable Care Act.Institute of Medicine, Washington, DC.U.S. Public Health Service. (2001, February).Closing the Gap: A National Blueprint forImproving the Health of Individuals with MentalRetardation. Report of the Surgeon General'sConference on Health Disparities and MentalRetardation. Washington, DC.David O’Hara, PhD, is the COO ofthe Westchester Institute for HumanDevelopment, a University Center forExcellence in Developmental Disabilities, inaffiliation with New York Medical College(NYMC). He holds a faculty appointment inthe School of Health Sciences and Practice.The Role of Self-Determination in ReducingHealth Disparities Among People withIntellectual and Developmental DisabilitiesDavid O’Hara, PhDIn 2003, an international groupconvened at the Westchester Institute forHuman Development and made one ofthe first explicit statements identifyingthe promotion of self-determination asa core strategy in the reduction of healthdisparities among people with intellectualand developmental disabilities (I/DD).The group stated, “All processes to reducehealth disparity should include a focuson promoting and enhancing individualeducation and choice over healthcare andhealth-related decisions” (Scheepers etal., 2005). Among the recommendationsfrom this international group werethe ideas that “support systems shouldenable” people with I/DD to exerciseself-determination, and they shouldbe assumed to be capable of exercising“greater control over their lives.”These recommendations have a lot ofhistory to overcome. An early report found2that for over 50% of people withI/DD, others make health care decisionsand choices for them (Wehmeyer &Meltzer, 1995; Shogren et al., 2006). In fact,the ability to exercise self-determinationat all often depends on the livingenvironment of the individual with I/DD(Stancliffe, Abery & Smith, 2000). A recentstudy from the Netherlands interviewedpeople with I/DD about their diabetesand their health care and found an almostcomplete absence of efforts to improvethe health status of their study groups bypromoting their active engagement inself-determination activities in their healthcare experience (Cardol, Rijken, & vanSchrojenstein Lantman-deValk, 2012).However, the accumulation of evidenceon the extent to which intellectual abilityrelates to specific health disparitiesshould now provide us with an impetusfor change. For example, people withNational Gateway to Self-Determinationcognitive limitations are almost six timesmore likely (19.4% vs. 3.8%) to experienceType 2 diabetes than the generalpopulation (Reichard & Stolze, 2011).But enhancing self-determinationon its own will not be enough tosubstantially reduce health disparities.As the international group also found,there are other factors at work. Theconcept of disparity in health is oftenused to highlight population inequalitieswhich are politically important, suchas health disparities between differentracial and ethnic groups. But for peoplewith I/DD this simple relationship is lessclear. There can be several reasons fordifferences in health such as poor accessto healthcare for people or an increase inpersonal disease susceptibility as a resultof a genetic syndrome such as Downsyndrome. An understanding of healthdisparity as it relates to people with I/
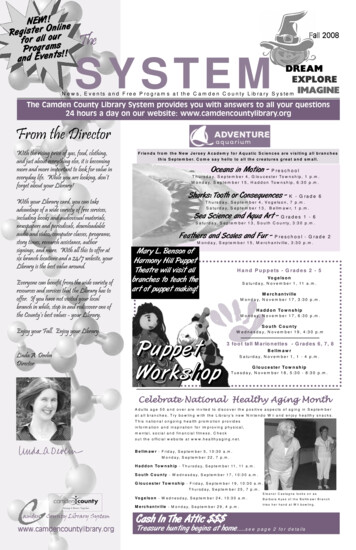
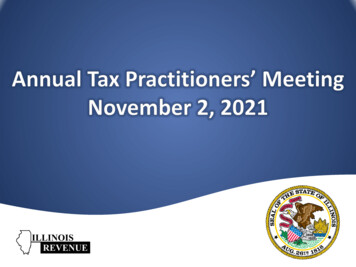
DD must reflect multiple factors. Theinternational workgroup found evidenceto propose four working definitions ofhealth disparity, characterized by: (1)decreased life expectancy; (2) increasedmorbidity, such as the co-occurrence ofchronic health conditions; (3) increases innegative determinants of health, such aspoverty; and (4) differences in both accessto health care and the quality of services.The term, “cascade of healthdisparities” has been used to capturethe cumulative impact of these differentsources of health disparity and theircontribution to poorer health outcomes forpeople with ID/D (Krahn, Hammond, &Turner, 2006). Many people withI/DD start life with multiple adversehealth conditions or begin to experiencethe health consequences of coping withmultiple chronic health conditionsthroughout their life course (figure 1).These health disparities are particularlystriking when comparing the prevalencerates for chronic health conditions(figure 2, Reichard, Stolze & Fox, 2011).Access to appropriate health carethen adds its own contribution to thehealth disparities between people withI/DD and the general population. Again,Medicaid expenditure survey datahighlight the critical importance of accessto preventive care for people with I/DD,and that they are often at a disadvantage(figure 3, Reichard, Stolze & Fox, 2011).The importance of regular healthcheck-ups to either identify or ensureattention to critical health care needs isgradually gaining acceptance (Robertson,Emerson, Turner, & Greig, 2011).Compounding the problem of healthdisparity among people with I/DD isthe adverse impact of socio-economicconditions on access to health care(Emerson, Hatton, & McLean, 2007).There is limited research thatspecifically addresses how increased selfdetermination for people with I/DD mightimprove their health experience and healthoutcomes, but the research that does existoffers several indicators of such a positiveeffect (Shogren et al., 2006). For example,Wehmeyer and Palmer (2003) found thatyouth who left high school with higherlevels of self-determination were morelikely to be employed in jobs with higherwages and health insurance. This suggeststhe potential of self-determination topositively impact socioeconomic status,one of the fundamental determinants ofhealth for people with I/DD (Graham,2005). The right to consent to medicaltreatment is another critical first step inpromoting self-determination in health.Wehmeyer and Metzler (1995) found intheir survey of opportunities to expressself-determination in everyday life thatonly 18% of people with I/DD indicatedthey independently consented formedical care, another 26% indicated theyconsented with support, but the majority,56%, indicated someone else consented forthem. Yet research has demonstrated thatpeople with mild to moderate intellectualdisabilities do have the capacity toconsent to standard medical treatment,and that with support they can also takean active role in decisions about morecomplex treatment (Cea & Fisher, 2003).Other research on the concept ofthe quality of life indicates that there isinteraction among the core dimensionsFigure 1Higher Rates of Adverse Health Conditions for People with I/DDConditionOuellette-Kuntzet al., 2005Communication limitationPhysical DisabilitiesBehavioral/ psychiatricSensory (hearing, vision)Epilepsy and neurologicaldisordersDermatologyFractures/ lacerationsGastrointestinalCardiovascular 30% 30% 30% 10-20%Krahn et chalock et al., 2002), so that effortsto promote self-determination have thepotential to influence the health-relateddimensions of physical and emotionalwell-being. Thus the skills and resourcesthat promote self-determination in generalshould also have the potential to enablepeople with I/DD to better manage theirown health and medical care and achievebetter health and wellness outcomes.Research on the leading evidence-basedmodel of chronic disease care (Wagner etal., 2001) has demonstrated that chronicdisease self-management educationalprograms are effective. Participants insuch programs achieve improvementsin health behaviors, self-efficacy, healthstatus, and healthcare use. New smarttechnologies provide a variety of accessibleand appropriate health promotion andwellness materials designed to enablepeople with I/DD to learn about theirhealth needs and engage in behaviorsthat promote positive health and medicaloutcomes (see articles in this Guiderelated to the “My Health, My Choice, MyResponsibility” and “Self-Determination,Technology and Health”). By increasingthe skills of people with I/DD so they canbecome more engaged and effective inthe management of their own health andwellness, and enhancing the capacity ofhealth delivery systems to provide accessand cognitive supports, the importantgoal of reducing health disparities for thispopulation may finally be within reach.ReferencesCardol, M., Rijken, M., & van SchrojensteinLantman-deValk, H. (2012). People with mildto moderate intellectual disability talking abouttheir diabetes and how they manage. Journal ofIntellectual Disability Research, 56(4), 351-360.Cea, C. D., & Fisher, C. B. (2003). Healthcare decision-making by adults with mentalretardation. Mental Retardation, 41, 78-87.Emerson, E., Hatton, C., & McLean Jr.,W. (2007). Contribution of socioeconomicposition to health inequalities of British childrenand adolescents with intellectual disabilities.American Journal on Mental Retardation,112(2), 140-150.Graham, H. (2005). Intellectual disabilitiesand socioeconomic inequalities in health:An overview of research. Journal of AppliedResearch in Intellectual Disabilities, 18, 101–111.Krahn, G., Hammond, L., & Turner, A.(2006). A cascade of disparities: Health andhealth care access for people with intellectualdisabilities. Mental Retardation andDevelopmental Disabilities Research Reviews:Special Issue: Preventive Health and IndividualsNational Gateway to Self-Determination3
Figure 2Reichard, Stolze and Fox, 2011Figure 3Reichard, Stolze and Fox, 20114National Gateway to Self-Determinationwith Mental Retardation, 12(1), 0-82.Reichard, A., & Stolze, H. (2011). Diabetesamong adults with cognitive limitations comparedto individuals with no cognitive disabilities.Journal of Intellectual and DevelopmentalDisabilities, 49(30), 141-154.Reichard, A., Stolzle, H., & Fox, M. (2011).Health disparities among adults with physicaldisabilities or cognitive limitations comparedto individuals with no disabilities in the UnitedStates. Disability and Health Journal, 4 (2), 59-67.Robertson, J., Roberts, E., Emerson, E.,Turner, S., & Greig, R. (2011). Invited review: Theimpact of health checks for people with intellectualdisabilities: A systematic review of the evidence.Journal of Intellectual Disability Research, 55(11),1009-1019.Scheepers, M., Kerr, M., O’Hara, D.,Bainbridge, D., Cooper, S-A., Davis, R., Fujiura,G., Heller, T., Holland, A., Krahn, G., Lennox,N., Meaney, J., & Wehmeyer, M. (2005).Reducing health disparity in people with learningdisabilities: A Report from the health issuesspecial interest research group of the InternationalAssociation for the Scientific Study of IntellectualDisabilities. Journal of Policy and Practice inIntellectual Disabilities, 2(3/4), 249-255.Schalock, R. L., Brown, I., Brown, R.,Cummins, R. A., Felce, D., Matikka, L., et al.(2002). Conceptualization, measurement, andapplication of quality of life for persons withintellectual disabilities: Report of an internationalpanel of experts. Mental Retardation, 40,457–470.Shogren, K., Wehmeyer, M., Reese, R., &O’Hara, D. (2006). Promoting self-determinationin health and medical care: A critical componentof addressing health disparities in people withintellectual disabilities. Journal of Policy andPractice in Intellectual Disabilities, 3(2), 105–113.Stancliffe, R. J., Abery, B. H., & Smith, J.(2000). Personal control and the ecology ofcommunity living settings: Beyond living-unitsize and type. American Journal on MentalRetardation, 105, 431–454.Wagner EH, Austin BT, von Korff M. (1996).Organizing care for patients with chronic illness.Milbank Quarterly. 74:511–544.Wehmeyer, M., & Metzler, C. (1995).How self-determined are people with mentalretardation? The National Consumer Survey.Mental Retardation, 33, 111–119.Wehmeyer, M. L., & Palmer, S. (2003). Adultoutcomes for students with cognitive disabilitiesthree years after high school: The impact ofself-determination. Education and Training inDevelopmental Disabilities, 38, 131–144.David O’Hara, PhD is the COO ofthe Westchester Institute for HumanDevelopment, a University Center forExcellence in Developmental Disabilities, inaffiliation with New York Medical College(NYMC). He holds a faculty appointment inthe School of Health Sciences and Practice.
Health Matters for People withIntellectual and Developmental Disabilities:Take Charge!Beth Marks, RN, PhD and Jasmina Sisirak, PhD, MPHPeople with intellectual anddevelopmental disabilities (I/DD), alongwith their families, and community-basedorganizations (CBOs) have advocatedfor their rights and opportunities inmany areas of community life, includingeducation, employment, housing,recreation, commerce, and civicengagement (Marks, Sisirak, & Heller2010a). Access to health care, healthpromotion, and disease prevention iscritical in being able to achieve andsustain community engagement; however,people with disabilities continue theirstruggle to receive accessible (e.g.,affordable, available) and acceptable(e.g., culturally relevant, satisfactory)health care. Like other under-servedpopulations, health promotion activitiescan enable people to take controlover and to improve their health (PanAmerican Health Organization, 2001).Extending advocacy to health andwellness activities is a key element forbridging equity gaps and achievingself-direction among people with DD.HealthMatters CAP is an NIH-fundedcollaboration which aims to enhancehealth status and optimize full communityparticipation of people with I/DD acrossthe lifespan. Through HealthMatters CAP,we are introducing a new approach, inwhich, two CBOs (NorthPointe Resourcesof Zion, IL and ARCA of Albuquerque,NM) and an academic institution(University of Illinois at Chicago) areworking together to find practicalsolutions using evidence-based curriculaand training to improve health. Currently,we are building the HealthMatters CAP infrastructure to facilitate andsustain healthy choices and behaviorsamong people with DD to improve theirhealth status through the following: workforce capacity developmentfor health promotion incommunity sectors; health advocacy capacity buildingfor people with DD; and, active participation among peoplewith DD in health promotionand health advocacy (www.HealthMattersProgram.org).Community EngagementWith the need for equality in healthcare for people with DD, CBOs supportingpeople with DD have a leadership rolewithin their communities to advocatefor improved access to quality healthservices, including health promotionand disease prevention. Disabilityservices professionals are key liaisonsto provide training across communitysectors to improve health literacy amongpeople with I/DD, their families, andprofessional and direct support people.The HealthMatters Train-theTrainer Workshop: Becoming aCertified Instructor (Marks & Sisirak2008) is an evidence-based, interactiveworkshop instructed by AdvancedCertified Instructors. During theworkshop, participants from communityorganizations are provided organizationaland individual support to implementa tailored 12-week physical activityand health education program that canbe personalized to meet the needs ofpeople with DD. This program uses theevidence- based curriculum entitledHealth Matters: The Exercise and NutritionHealth Education Curriculum for Peoplewith DD (Marks, Sisirak & Heller 2010b).The one-day workshop aims to teachparticipants how to do the following: 1)start and implement a physical activityand health education program using theExercise and Nutrition Health EducationCurriculum; 2) identify strategies formotivating and engaging individualswith DD in a physical activity and inhealth education; 3) teach core conceptsrelated to physical activity and nutrition(e.g., heart rate, blood pressure, use ofequipment, safety); 4) support people withDD to incorporate physical activity andhealthy lifestyles into activities of dailyliving, and, 5) evaluate the effectivenessof a health promotion program.People with DD have a right to receiveeducation and services that promotetheir health. The HealthMatters Workshopincorporates the concepts of choice,self-determination, self-efficacy, selfadvocacy, rights and responsibility. Formaximum involvement of people withDD in making and achieving physicalactivity and nutrition goals, havingthe power of direct support staff andorganizational support in the provisionof health promotive rather than curativeactivities can improve health outcomes.Health AdvocacyThe lives of people with DDincorporate a culture of interdependencyin that many people live their entirelives relying on their family membersand multiple professionals for support(Carnaby 1998). People with DD continueto lack control over situations andpractices influencing their lives and healthstatus. As such, in addition to the need tobuild skills among individuals with DD,building collective efficacy among proxyagents such as health care professionalsNational Gateway to Self-Determination5
group and self-directedness to promotesocial change in health care for peoplewith I/DD (Bandura, 2000,1994).Peer Supportand direct care professionals is imperativein our efforts to foster self-direction.The Building Capacity to PromoteHealth Advocacy among People withDD workshop uses an evidence-basedcurriculum (Marks Sisirak & Cutler 2008)that aims to increase understandingof the health care experiences and theneeds of adolescents and young adultswith DD among health care professionalsand their caregivers. This workshopcovers the following four critical areasfor increasing and supporting healthadvocacy skills among people with DD: Health Care Interactions: Charityto Advocacy - Review the historicalfactors that impact attitudes, beliefs,and treatment of people with DD. Health Promotion: Beyond IllnessCare - Discuss determinantsof health and issues relatedto nutrition, physical activity
National Gateway to Self-Determination 1 Self-Determination and Health David O'Hara, PhD This Research to Practice Guide will focus on the potential of promoting self-determination in health which has only recently been explored as a means of reducing the ongoing and significant health disparities experienced by people with intellectual and