Transcription
SeriesFungal infections 4Neglected endemic mycosesFlavio Queiroz-Telles, Ahmed Hassan Fahal, Diego R Falci, Diego H Caceres, Tom Chiller, Alessandro C PasqualottoFungi often infect mammalian hosts via the respiratory route, but traumatic transcutaneous implantation is also animportant source of infections. Environmental exposure to spores of pathogenic fungi can result in subclinical andunrecognised syndromes, allergic manifestations, and even overt disease. After traumatic cutaneous inoculation,several fungi can cause neglected mycoses such as sporotrichosis, chromoblastomycosis, mycetoma,entomophthoramycosis, and lacaziosis. Most of these diseases have a subacute to chronic course and they can becomerecalcitrant to therapy and lead to physical disabilities, including inability to work, physical deformities,and amputations. For many years, paracoccidioidomycosis was considered the most prevalent endemic systemicmycosis in the Americas, but this situation might be changing with recognition of the worldwide presence ofHistoplasma capsulatum. Both paracoccidioidomycosis and histoplasmosis can mimic several infectious and noninfectious medical conditions and lead to death if not recognised early and treated. Cutaneous implantation andsystemic mycoses are neglected diseases that affect millions of individuals worldwide, especially in low-incomecountries where their management is suboptimum because challenges in diagnosis and therapeutic options aresubstantial issues.IntroductionCutaneous implantation mycosesNeglected tropical diseases (NTDs) are a diverse seriesof endemic diseases that prevail in tropical orsubtropical climates worldwide. They are infectiousdiseases usually affecting people living in low-incomecountries in Asia, Africa, and Latin America. NTDsusually affect populations that do not travel abroad,with little political voice and low visibility. According toWHO, a high prevalence of NTDs is associated withpoverty and other disadvantageous conditions.1Individuals affected by NTDs are often the world’spoorest populations, often living in remote rural areas,urban slums, or conflict zones. Although progress hasbeen made for some NTDs, many of these diseases arenot on the public health radar, by contrast with otherhigh-profile global diseases.1 WHO and otherorganisations such as the G-FINDER project recogniseseveral helmintic, protozoan, bacterial, and viralinfections as NTDs, but most fungal infections havenot yet reached such status. However, in 2016,mycetoma was included as the only fungal disease inthe WHO list of NTDs, and chromoblastomycosis wasadded in 2017.1–4The burden and medical impact of fungal diseasesare largely unknown and often underestimated,especially for endemic fungal infections. Endemicmycoses can be divided into two groups: implantation(subcutaneous) mycoses in which the fungal agentsgenerally infect transcutaneous wounds; and systemicmycoses, in which thermodimorphic fungi are inhaledcausing infection and can disseminate. Fungal(mycotic) keratitis is an implantation mycosis andfulfils criteria for an NTD, although it is a globalproblem with occasional cases in high-income nontropical countries; this disease will not be addressed inthis paper.Implantation mycoses are a heterogeneous groupof fungal diseases, which present months or years afterinitial infection.5 This group includes sporotrichosis,chromoblastomycosis (chromomycosis), mycetoma,lacaziosis (lobomycosis), and entomophthoramycosis(subcutaneous zygomycosis). These diseases primarilyaffect the cutaneous and subcutaneous tissues, but inmost cases they also involve adjacent structures such asthe lymphatics, cartilage, fascia, joints, and bones.5–8Most implantation mycoses occur in tropical andsubtropical regions of the world and usually affectindividuals involved in outdoor activities such asagriculture, hunting, mining, and lumbering. Lesscommonly, children, travellers, and visiting workersdevelop implantation mycoses.5–9 These diseases mimicseveral infectious and non-infectious disorders and theirburden is underestimated because of a lack of diagnosisin the areas where they occur (table 1).SporotrichosisSporotrichosis is the most prevalent and widespreadimplantation mycosis in the world. For more than acentury, this disease was believed to be caused by a singlespecies, Sporothrix schenckii, but more recent molecularphylogenetic methods have shown that this fungus has awide spectrum of biodiversity with several sibling species.These species vary by virulence, mode of transmission,clinical manifestations, and response to therapy. Thetaxonomy of the Sporothrix genus has recently beenrevised and is now classified according to its phenotypicand biochemical characteristics together with itsmolecular profile. The original S schenckii sensu latocontains clinically relevant cryptic species with diversegeographical distribution: S schenckii sensu stricto andSporothrix globosa cause sapronotic sporotrichosiswww.thelancet.com/infection Published online July 31, 2017 cet Infect Dis 2017Published OnlineJuly 31, 7See , ee (17)30319-5This is the fourth in a Series ofeight papers about fungalinfectionsHospital de Clínicas, FederalUniversity of Paraná, Curitiba,Brazil (F Queiroz-Telles MD);Mycetoma Research Centre,University of Khartoum,Khartoum, Sudan(Prof A H Fahal); InfectiousDiseases Service, Hospital deClínicas de Porto Alegre, PortoAlegre, Brazil (D R Falci PhD);Centro Universitário La Salle,Canoas, Brazil (D R Falci);Mycotic Diseases Branch,Centers for Disease Control andPrevention, Atlanta, GA, USA(D H Caceres PhD, T Chiller MD);Santa Casa de Misericórdia dePorto Alegre, Porto Alegre,Brazil (A C Pasqualotto MD); andUniversidade Federal deCiências da Saúde de PortoAlegre, Porto Alegre, Brazil(A C Pasqualotto)Correspondence to:Dr Flavio Queiroz-Telles,Department of Public Health,Federal University of Paraná,Curitiba, Paraná 80060-240, Brazilqueiroz.telles@uol.com.br1
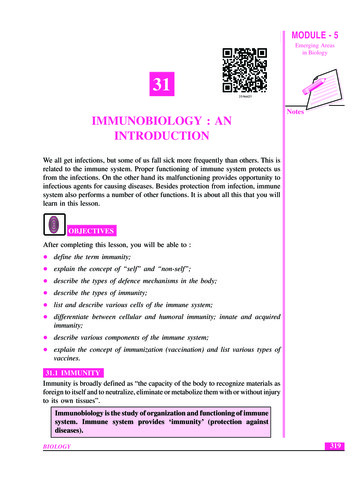
SeriesKey messages The burden and medical importance of endemic mycoses remain underestimated. Most of the serious endemic fungal infections have not yet reached the status ofneglected diseases as defined by WHO. The most relevant implantation mycoses are sporotrichosis, chromoblastomycosis,and mycetoma. Most of these infections occur in underdeveloped tropical andsubtropical regions of the world. Sporotrichosis caused by Sporothrix schenckii sensu lato is a sapronosis and occursworldwide, whereas sporotrichosis caused by Sporothrix brasiliensis is ananthropozoonosis affecting human beings, cats, and dogs. The disease can occur asoutbreaks that might affect thousands of people. Chromoblastomycosis is a potentially debilitating disease caused by several melanisedfungi found in plants or soil. It has an occupational risk and diagnosis relies onvisualisation of the typical muriform (sclerotic) cells by direct microscopy. Mycetoma causes high morbidity and affects poor populations living in remote areasof the world. This disease causes painless subcutaneous masses, sinus formation,and occasional discharge of grains. Entomophthoramycosis, also known as subcutaneous zygomycosis, causes chronicdestructive lesions that can be diagnosed by a combination of microscopy, culture,and histopathology. Lacaziosis, also known as lobomycosis, is an exotic and mysterious disease. Mostaffected individuals are from the Amazon region. Lacazia loboi, which infects humanbeings and dolphins, has never been cultivated in vitro. It is recalcitrant to antifungaltherapy. Histoplasmosis and paracoccidioidomycosis are the most relevant neglected endemicsystemic mycoses in Latin American countries. These diseases are commonlymisdiagnosed as tuberculosis, resulting in a substantial delay in treatment. Histoplasma capsulatum infection is expanding outside the American endemic area.It is a frequent cause of disseminated disease in endemic regions. Regions with thehighest burden of histoplasmosis usually lack effective methods of diagnosis (antigendetection) and treatment (lipid formulations of amphotericin B). Paracoccidioidomycosis has a substantial impact on public health. It mostly affectsmale farmers in their productive ages, potentially making them unable to work.See Online for appendixworldwide. These species are ubiquitous and infectionusually occurs via transcutaneous inoculation ofcontaminated plant debris.28 Sporothrix luriei is restrictedto Africa and Asia and Sporothrix brasiliensis is restrictedto Brazil. Most Asian isolates are S globosa.29–31 All causativeagents of sporotrichosis can be recovered from classicenvironmental sources of infection for S schenckii sensulato, apart from S brasiliensis, which is associated withfeline transmission of the disease.31–34 S brasiliensis is anemerging anthropozoonosis affecting human beings,cats, and dogs. Sick cats usually have a heavy S brasiliensisfungal burden, which can be transmitted directly in theyeast form.34 Beyond transcutaneous inoculation relatedto plant or animal trauma, other ports of entry such asrespiratory, conjunctival, and osteoarticular routes ofinfection can also occur.35,36Epidemiology and geographical distributionAreas endemic for sporotrichosis include Latin America,India, Australia, South Africa, China, and Japan.5,31Prevalence is not uniform and varies according to the2epidemiological pattern of transmission. The highestestimated prevalence rates of infection range from 0·1%to 0·5% in some Latin American countries.5,31 A fewhyperendemic areas of sporotrichosis have beenidentified—namely, in Mexico, Peru, and China.31,37–40Case reports from several countries have been published,but outbreaks and clusters of cases can occur. The largestreported sporotrichosis outbreak involved more than3000 miners in South Africa during the 1940s.41 However,a larger outbreak of cat-transmitted sporotrichosis iscurrently occurring in Brazil. In the state of Rio deJaneiro, the number of human cases jumpedfrom 759 between 1998 and 2004 to more than 4000 in 2014,mostly resulting from feline transmission. This outbreakis expanding to neighbouring Brazilian regions34,42,43(figure 1).Clinical presentationMost patients present with cutaneous forms ofsporotrichosis that include fixed cutaneous (25%) andlymphocutaneous (55%) involvement.6 Cutaneous dis seminated forms are reported in immunocompetent andimmunosuppressed individuals.44 Extracutaneous involve ment has rarely been described, notably pulmonary,osteoarticular, ophthalmic, and CNS infection. Meningitisis more frequently seen in immunocompromisedindividuals. An increased number of immunoallergicforms (eg, erythema nodosum, arthralgia, myalgia, andchorioretinitis) have been described during the continuingoutbreak in Brazil.35,36DiagnosisCulture remains the gold standard for diagnosis ofsporotrichosis. Clinical specimens should be inoculatedon Sabouraud agar and incubated at room temperaturefor 1–4 weeks. Microscopy is useful only in the presenceof high fungal load. ELISA serodiagnosis has shownaccuracy and low cross-reactivity to detect a range ofclinical forms of sporotrichosis.45TreatmentThe best therapeutic choice for cutaneous and lympho cutaneous forms of sporotrichosis is itraconazole,with either terbinafine or super-saturated potassiumiodide as second-line options.5,10,11 If possible, plasmaconcentrations of itraconazole should be monitoredduring treatment. For meningitis and disseminateddisease, lipid amphotericin B (3–5 mg/kg per day) is abetter option. The roles of posaconazole and isavuconazolehave yet to be determined (table 1, appendix).ChromoblastomycosisChromoblastomycosis is the second most prevalentimplantation mycosis in the world. This disease is causedby melanised (dark pigmented) fungi, which are almostall members of the Herpotrichiellaceae family.5,12 Themost prevalent species causing chromoblastomycosiswww.thelancet.com/infection Published online July 31, 2017 http://dx.doi.org/10.1016/S1473-3099(17)30306-7
Seriesare Fonsecaea pedrosoi, Fonsecaea monophora, andCladophialophora carrionii. Sporadic cases may be causedby Phialophora verrucosa, Rhinocladiella aquaspersa,Exophiala spp, and other species of Fonsecaea.17,46,47Advances in molecular taxonomy have shown thatthe biodiversity of chromoblastomycosis agents hasincreased without substantial clinical or therapeuticcorrelation.48 An inability of Toll-like receptors toEpidemiology and geographicaldistributionClinical presentationDiagnosisTreatmentSporotrichosisGlobal geographical distribution;variable sex and age distribution.Plant or soil transmission: mainly inindividuals in contact with vegetationand soil (eg, agriculture activities,gardening, plant manipulation,mining, hunting, other outdooractivities). Zoonotic transmission:mainly from cats, occasionally fromdogs, birds, armadillos, and fish.Opportunistic disease: alcoholism,steroids, AIDS, TNF inhibitorsFixed cutaneous involvement:polymorphic skin lesions (eg, papules,nodules, ulcers, verrucous lesions,plaques) following trauma.Lymphocutaneous involvement:nodules, ulcers, abscesses trackingalong regional lymphatic chains;regional adenopathy. Extracutaneousforms: pulmonary, osteoarticular,neurological, and ophthalmologicalMycology: microscopy has limitedsensitivity. Culture of clinical samples(eg, biopsy samples, pus, exudates,or aspirates) remains the gold standard;fungal dimorphism must bedemonstrated. Serology: ELISA mightbe helpful in CNS infection.Histopathology: non-specific in mostimmunocompetent patients; yeastcells, cigar-shaped cells, asteroid bodies,and Splendore-Hoeppli reaction areseen in 30% of cases apart from inimmunocompromised hostsFixed or lymphocutaneous: oralitraconazole 200 mg per day for2–4 weeks after lesions resolve, usuallyfor total of 3–6 months. Refractory orintolerant patients: oral terbinafine500 mg twice daily, SSKI 40–50 dropsthree times daily, oral fluconazole400–800 mg per day (only in patientswho cannot tolerate other agents). Otherclinical presentations: combination ofitraconazole and terbinafine, plusamphotericin B5,10,11ChromoblastomycosisGlobal tropical distribution, usually inmen aged 30–50 years; affectsfarmers, gardeners, and lumberjacks;a risk factor is non-use of protectivegloves, footwear, or garments whenworking with plants and soil products.Occupational risk for people workingwith palm trees, black tea and rubberplantations, etc. Possible geneticsusceptibility.Slow clinical progression usually limitedto the skin and subcutaneous tissue inwhich initial erythematous papularlesions might gradually evolve todisplay varying morphologies, such asnodular, tumoral (cauliflower-like),plaque, verrucous, and cicatriciallesions. Affects feet and legs mostfrequently; can transform intosquamous cell carcinomaMycology: the observation of muriformcells (sclerotic bodies) is diagnostic.Examination of scrapings, exudate,or aspirates, or vinyl adhesive tapepreparations on wet mountexamination. Culture with molecularidentification is necessary for speciesidentification. Histopathology:pseudoepitheliomatous hyperplasia,granulomatous reaction, andepidermic abscess associated withmuriform cells are usualSurgery effective in early stages;itraconazole (200–400 mg per day),terbinafine (250–500 mg per day),terbinafine (500 mg per day) plusitraconazole (50–100 mg per day);combination therapy (itraconazole withterbinafine or flucytosine) for severecases, oral posaconazole (400 mgtwice daily) in patients with diseaserefractory to itraconazole or who areintolerant of itraconazole;cryotherapy12–14EumycetomaMen aged 20–40 years who work asherders, farmers, or other fieldlabourers;15 increasingly in travellers totropical endemic areas5,16Local chronic, progressive,multifistulous, suppurative, tumorallesions discharging grains. Infectioninvolves cutaneous and subcutaneoustissues, fascia, and eventually muscleand bone17Observation of grain colour andtexture; deep surgical biopsy samplescontaining grains that can be culturedor fixed for histopathology;immunodiffusion, ELISA, PCR withDNA sequencing; MRI or CT todetermine bone involvement2,5,18For Scedosporium apiospermum andmelanised fungi causing so-called blackgrain eumycetoma, surgery andantifungal therapy with oral itraconazole(400 mg), often given for 7–12 months;oral posaconazole (400 mg twice daily)in patients with disease refractory to orwho are intolerant of itraconazole.5,19For Fusarium spp infections, voriconazoleor posaconazole are indicatedEntomophthoramycosisInfections usually caused by fungi ofthe order Entomophthorales, usuallyin immunocompetent individuals.Basidiobolomycosis usually occurs inchildren and conidiobolomycosismostly in adults20Basidiobolomycosis: usually chronicand progressive course; hard nodulesthat spread, often over thighs andbuttocks, eventually ulceratingoverlying skin; other affected sitesinclude maxillary sinus, palate,gastrointestinal tract, retroperitonealspace, and lungs.21 Conidiobolomycosis:begins with swelling of inferior nasalcones and extends to facial andsubcutaneous tissues and paranasalsinuses; subcutaneous nodules mayattach to underlying tissues, causingfacial disfigurement22Histology: wide sparse septate, thinwalled hyphae with right-anglebranching. Splendore-Hoeppli reactionpresent with basidiobolomycosis(sometimes withconidiobolomycosis)20Most commonly used therapy isitraconazole (100–200 mg per day);potassium iodide, or terbinafine mightbe a second option. Amphotericin B forsevere and disseminated disease21,23LacaziosisAdult men living or working in theAmazon rainforest. Farmers, miners,hunters, rubber workers, and militarypersonnel are at risk24,25Lesions are indolent, evolving overmany years; polymorphic cutaneouslesions, mostly plaque and noduleswith keloid-like features; pinna of theear most commonly affected; initiallesion followed by traumatic orautoinoculation; nodule distributionfollows lymphatic system24,26Microscopy of tissue smears fromlesions, examination of vinyl adhesivetape preparation; cannot be cultured.Serological tests: high sensitivity butlack specificity; antigenic crossreactivity with Paracoccidioides spp26Wide surgical excision,electrodesiccation in early stage ofdisease, cryosurgery; clofazimine(300 mg per day until clinicalimprovement, then 100 mg per day for 2 years).24 Amphotericin B, flucytosine,and azoles usually ineffective, except forlocalised lesions that might respond tolong courses of posaconazole27SSKI saturated solution of potassium iodide. TNF tumour necrosis factor.Table 1: Main characteristics of the endemic implantation mycoseswww.thelancet.com/infection Published online July 31, 2017 http://dx.doi.org/10.1016/S1473-3099(17)30306-73
Series4000Human cases of sporotrichosis35003000fungus. For correct species identification, fungal DNAsequencing is required.Total number of cases diagnosedbetween 1998 and 2012Human cases 4000Feline cases 3800Canine cases 042006200820102012YearFigure 1: Cases of sporotrichosis diagnosed in Rio de Janeiro between 1996and 2012The cat-transmitted sporotrichosis outbreak is expanding to other regions inBrazil and involves human, feline, and canine hosts.34,42,43recognise pathogens might be a key component ofpathogenesis.49Epidemiology and geographical distributionFungi causing chromoblastomycosis are components ofplant or soil microbiota and infection follows severaltypes of wounds, many of which occur during agriculturalactivities.15,50–53 Chromoblastomycosis mainly occurs intropical and subtropical zones in Latin America, Africa,and Oceania.12 Most cases are reported in Brazil, Mexico,southern China, Australia, and Madagascar.53–57 Estimateddata gathered from case series reports and surveyssuggest that the incidence of this disease might rangefrom 1 per 6800 (Madagascar) to 1 per 8625 (USA) in thetotal populations of these countries.15,58 This infection islikely to be present in many African countries, but isunderdiagnosed.Clinical presentationAfter an uncertain period of incubation, the initial lesionsarise at the site of inoculation. Over weeks and months,these can evolve to cutaneous and subcutaneouspolymorphic lesions. In advanced cases, different lesionpatterns have been observed.12,13,48 The clinical forms ofthe disease might be associated with cytokine cellularmediated response and in severe cases, the production oftumour necrosis factor α and interleukin 10 has beendetected.13,59,60DiagnosisFor confirmation of a diagnosis of chromoblastomycosis,visualisation of the typical muriform (sclerotic) cellsby direct microscopy (potassium hydroxide 10–40%digestion) or in tissue sections is required. Muriformcells appear as chestnut or rounded melanised fungalelements crossed by longitudinal and transverse septa.12,61In culture, the organisms grow slowly on Sabouraud agarcontaining antibiotics, yielding a melanised filamentous4The best therapeutic method for small initial lesions issurgical excision. Diagnosis is often delayed and systemicantifungal therapy is usually required. Long-term therapywith itraconazole is the best option for inoperablelesions. The response rate to itraconazole rangesfrom 15% to 80%, depending on the causative agent andseverity of the disease.12,14,62,63 Terbinafine is anotheroption, and for refractory cases, the combination ofitraconazole with terbinafine or flucytosine can beused.63,64 The addition of physical methods such asphotodynamic, local thermotherapy (heat or cold), orimmunoadjuvants (eg, topical imiquimod)63–66 mightimprove response rates. Of the new e 1, appendix).MycetomaMycetoma is a chronic, progressive, implantationinflammatory disease characterised by severe and stigma tising deformities, disability, and high morbidity. Thedisease can be caused by fungi (eumycetoma) and severalmembers of the bacterial order Actinomycetales(actinomycetoma), and it affects the poorest populations inthe most remote tropical and subtropical regions of theworld. Mycetoma is a disease that causes minimalmortality but high morbidity;67 it leads to devastatingdeformities that can result in many negative socioeconomiceffects. The lack of national and international attentionand awareness has led to a knowledge gap that substantiallyaffects patient care and impedes control.68Epidemiology and geographical distributionAlthough the true incidence and prevalence of mycetomaare not known, a prevalence of 14·5 per 1000 inhabitantshas been reported in some endemic areas.69,70 There areno definitive studies on the route of transmission formycetoma. The causative organisms are thought tooriginate in soil or animal dung and are inoculated in thesubcutaneous tissue after minor injuries such as thosecaused by thorn pricks. There is a clear relation betweenmycetoma and individuals who walk barefoot andworkers engaged in manual labour in rural areas, but noone is exempt. No animal reservoir has been identified,although rare cases have occurred in several vertebrates.2,71The causative organisms are distributed worldwide butare endemic in several tropical and subtropical countries,making up what has been called the mycetoma belt.The belt includes, among others, central Africa(Chad, Ethiopia, Mauritania, Sudan, Senegal, andSomalia) as well as Mexico, India, Venezuela, and Yemen.The mycetoma belt is characterised by a hot, dry climatewith a short, heavy rainy season. Eumycetoma is mainlyendemic in Africa.16,72www.thelancet.com/infection Published online July 31, 2017 http://dx.doi.org/10.1016/S1473-3099(17)30306-7
SeriesClinical presentationMycetoma is clinically characterised by a triad of apainless subcutaneous mass, sinus formation, andoccasional discharge of material including pathogno monic grains. Grains are hard, differ in colour, andhave the size of a coarse grain of sand. The mass isprogressive and usually spreads to invade the deepertissues and bones, resulting in local structuraldeformity and functional impairment. The mostcommon sites of infection are the limbs. Rarely, thetrunk, perineum, head and neck, and other body sitescan be affected.Males are more commonly affected than females. Mostpatients are young adults from poor socioeconomicbackgrounds with minimal education. Mycetomais frequently seen in farmers and students. About20–25% of patients are children, who become stigmatisedand often drop out of school. Most cases present withadvanced disease, which is thought to be because of poorhealth education, scarcity of rural health facilities, andeconomic limitations in seeking care.68–70DiagnosisThe causative organisms can be detected by cytologicalsmears and surgical tissue biopsy examinations, grainmicroscopy, and fungal culture. For appropriatetreatment, the distinction between actinomycetomaand eumycetoma is mandatory. Species identificationis helpful for epidemiological studies, especially ifmolecular methods are used. Unfortunately, serologyis insensitive and lacks specificity. Most of thediagnostic techniques are not available for people withmycetoma. There are also no point-of-care testsavailable for use in mycetoma-endemic villages.18Imaging is required to delineate the disease extent,especially for defining bone involvement and surgicalexcision options.TreatmentCure rate is 25–35% at best. Treatment for eumycetomaconsists of prolonged antifungal therapy with secondgeneration triazoles. Itraconazole is the most commonlyused drug,73 but there is a potential role for voriconazoleor posaconazole, or antifungal combinations, inrefractory patients or even as first-line therapy. Afterazole therapy, surgical excision of the remaining mass isrecommended.74 Postoperative antifungal treatment ismandatory to reduce recurrence. Amputation is oftenneeded in cases of advanced disease.74 Current treatmentoptions are usually associated with substantial toxicity, inaddition to limited efficacy. Median treatment duration is12 months, which makes it expensive for patients as wellas for health authorities in endemic areas5,73 (table 1).In addition to disappointing cure rates, there is a highlevel of therapy dropout (55%), high need for amputation(15%), and frequent recurrence (27·5%). Because of thesuboptimal management and high costs associated withstandard treatment, many patients with mycetomaprefer alternative medicines. There is an urgent needfor new, safe, and effective medicines for use in ruralsettings (appendix).74EntomophthoramycosisA less frequent implantation endemic mycosis caused byfungi of the order Entomophthorales, subphylumEntomophthoramycota, is called entomophthoramycosisor entomophthoromycosis, also known as subcutaneouszygomycosis. This disease is mostly reported intropical and subtropical countries and encompassesconidiobolomycosis, caused by Conidiobolus coronatus andConidiobolus incongruus, and basidiobolomycosis, causedby Basidiobolus ranarum.20 These fungi are found in soilmicrobiota. B ranarum has been isolated from insects anddecaying vegetables and also from the intestines of somereptiles, amphibians, and domestic and wild mammals.Although its prevalence is highest in tropical andsubtropical zones in Africa, Asia, and Latin America, theburden of basidiobolomycosis might be expanding, withseveral cases reported in the USA.5,75 Conidiobolomycosisis mostly reported in west Africa, South America,Saudi Arabia, Oman, India, and Taiwan.20,22Clinical presentationHuman conidiobolomycosis is a slowly progressive diseasethat mainly affects the mucocutaneous facial structuressuch as the nose, cheeks, upper lip, and mucosa of theparanasal sinuses and pharynx. With progression, thelesions are usually associated with indolent diffuse oedema,leading to disfigurement and sequelae.22,75Basidiobolomycosis is more prevalent in men than inwomen, but it also affects children. Most people infectedwith B ranarum are apparently immunocompetent.Initially, erythematous nodular lesions are observed on thetrunk and limbs but with time, they can converge with anecrotic appearance and cellulitis. The infection canspread locally, affecting muscles, bones, regional lymphnodes, and even the adjacent organs. Increasing numbersof cases involve the gastrointestinal system. The clinicalpicture might mimic that of inflammatory bowel disease,especially Crohn’s disease and malignancy.21DiagnosisBoth forms of entomophthoramycosis are easilydiagnosed by microscopy, fungal culture, and histo pathological examination of biopsy specimens. Hyphaeare broad, distorted, with very few septations, and showright-angle branching, as seen in mucormycosis. Unlikewith mucormycosis, an immunoallergic reaction,the Splendore-Hoeppli reaction, an eosinophilic andamorphous deposit of hyaline material around parasites,resulting from local antigen–antibody reaction, mightbe observed with entomophthoramycosis. Molecularmethods are useful for fungal identification of culturesand directly from tissue.9www.thelancet.com/infection Published online July 31, 2017 http://dx.doi.org/10.1016/S1473-3099(17)30306-75
Seriesis almost exclusively seen in South America’s Amazonarea, usually affecting some specific Indian populations,farmers, or people living in the rainforest.5,24 The diseasehas been identified in dolphins outside the endemicarea, including in south Brazil, Suriname, Florida (USA),and France;78,79 these dolphins might have been infectedwhen swimming through rivers from the Amazonbasin.25Most patients with lacaziosis
therapy. Histoplasmosis and paracoccidioidomycosis are the most relevant neglected endemic systemic mycoses in Latin American countries. These diseases are commonly misdiagnosed as tuberculosis, resulting in a substantial delay in treatment. Histoplasma capsulatum infection is expanding outside the American endemic area.