Transcription
Original articleEffect of Different Modes of Mechanical Ventilation on ChronicObstructive Pulmonary Disease Patients with Respiratory FailureRegarding Echocardiographic Changes and Diaphragmatic UltrasoundcAhmed G. EL gazzar a, Tarek S. Essawy a, Basem M. Aglan b, Emad F. Ibrahim , Enas W.Mahdy daDepartment of chest disease,Benha faculty of medicine,BanhaUniversity,Egypt.bDepartment of cardio-thoracicsurgery, Benha faculty ofmedicine, Banha University,cAbstractObjectives and aim:Recently, a concern has emerged with regardto the potential adverse effects of invasive mechanical ventilationon the respiratory muscles. This entity was originally termedEgypt. Department of criticalcare, Benha faculty of medicine,BanhaUniversity,Egypt.ddepartment of anesthesia andsurgical intensive care, Benhafaculty of medicine, BanhaUniversity, Egypt.ventilator-induced diaphragmatic dysfunction (VIDD). This studyCorrespondence to: Enas W.out on 100 mechanically ventilated chronic obstructive pulmonaryMahdy,Departmentofanesthesia and surgical intensivecare, Benha faculty of medicine,Banha University, EgyptdiseaseEmail:enaswageh@yahoo.comaimed to detect the impact of different modes of mechanicalventilation on diaphragmatic performance and echocardiographicparameters of COPD patients by using diaphragmatic ultrasoundand ECHO.Patients and methods: The present study was ment of diaphragmatic ntfortheadditiontomodesofmechanical ventilation. These patients were randomly allocatedaccording to modes of mechanical ventilation that used into fourgroups, each one included 25 patients. Results:There was a highlyReceived: 26 October 2021Accepted: 13 December 2021statistically significant decrease in diaphragmatic performancewhen controlled mechanical ventilation (CMV) was applied onlyon patients, in contrary diaphragmatic performance was improvedwhen pressure support ventilation (PSV) combined with CMV where no significant change indiaphragmatic mobility parameters occurred. And also no significant correlation was detectedbetween echocardiographic parameters (left ventricular ejection fraction, right ventricular size,tricuspid annular plane systolic excursion, right ventricular systolic pressure) and differentmodes of mechanical ventilation. Conclusion: The best diaphragmatic performance was on PSV,which improved lung volumes and ventilation, and may increase the rate of success of the62
Mechanical ventilation moods and COPD, 2022weaning process. In addition, we concluded that the echocardiographic finding was not affectedby different modes of mechanical phragmatic iseasehypertension,corpulmonale,right(COPD) is a common respiratory problemventricular dysfunction, and left ventricularthat includes bronchitis and emphysema. Itdysfunction too. Echocardiography providesis becoming a major health and economica rapid, noninvasive portable and accurateproblem worldwide; in 1990, it was the sixthmethod to evaluate the right ventricularmost common cause of death and be thirdfunction, right ventricular filling pressure,most common cause at 2020 (1).tricuspidregurgitation,functionandCOPD is a multi-systemic disease thatmainly affects and the lungs, and the musclemass.Therespiratorymusclesforcedecreases resulting in a negative impact onthe possible alteration of the ventilator andexercise capacity (2).Diaphragm is themain responsible of tidal volume in rasound is becoming widely used in theintensive care unit (ICU) to detect anycardiac,respiratoryordiaphragmaticchanges in COPD patient under mechanicalventilation (5, 6, and 7). Ultrasound may beusefulingivingagoodideaofcardiorespiratory state at different phases ofCOPD and during weaning of ventilationAt rest; studies have shown that the(8).impairment of diaphragmatic mobility mightbe associatedwithalterationsintheprincipal pulmonary function parameters(3). COPD affects pulmonary blood vessels,right ventricle, and also left ventricle whichlead63todevelopmentofpulmonaryThis study aimed to assess the impact ofdifferent modes of mechanical ventilation ondiaphragmaticperformanceandechocardiographic parameters of COPDpatients by using diaphragmatic ultrasoundand ECHO.
Benha medical journal, vol. 39. issue 1, 2022electrolytes imbalance were excluded fromPatients and methods:the study.This prospective, randomized, observerblinded and comparative clinical trial wasconducted at Critical care department,Benha university hospitals from JanuaryThese patients were randomly allocatedaccordingtomodesofmechanicalventilation that used into four groups. Anonline randomization program was used to2020 to September 2021.generateanumberlistAfter local ethical committee approval and(http://www.randomizer.org).patient’s (or his relatives) informed writtenrandomization numbers ofconsent, this study was conducted on 100in opaque envelopes which were opened byCOPD male patients who fulfilled thethe study investigator.Patientwere concealeddiagnostic criteria of COPD, on invasivemechanical ventilation, their ages 40years, hemodynamically stable, and fullyIn the first group (Group PCV) (25 patients),Pressure controlled ventilation (PCV) wasused only as a mode of ventilation for thoseconscious.patients.Patients who were intubated because ofsurgical or medical problems other thanCOPD,patientswithascites,colonicdistension, lung collapse, lung fibrosis,pleural effusion, any mechanical factor inIn the second group (Group VCV) (25patients), Volume controlled ventilation(VCV) was used only as a mode ofventilation for those patients.the chest or abdomen interfering withIn the third group (Group PCV PSV) hpressure-controlleddiaphragmatic paralysis or diaphragmaticventilation (PCV) and pressure supporthernia, patients with chest deformities thatventilation (PSV) were applied alternativelycan affect diaphragmatic mobility (i.e.on those patients.kyphosis scoliosis), patients with primarycardiac diseases (i.e. myocardial infarction,cardiomyopathy, pericardial effusion, etc.),Unstablehemodynamics,comatose,neuromuscular disorder, Organ failure or64In the fourth group (Group VCV PSV) (25patients), both volume-controlled ventilation(VCV) and pressure support ventilation(PSV) were applied alternatively on patients.
Mechanical ventilation moods and COPD, 2022At Day 1 and Day 4 of invasive mechanicaldiaphragmatic mobility and measurement ofventilation, All patients were subjected to anechocardiographic parameters of all patientsassessment of:-by the same operator.1- Full historyThe right hemi-diaphragm excursion (DE)was measured by using a 3.5 C (bandwidth2- General, local examination.2–5 MHz) convex phased array probe (a3- ECG.low-frequency with greater depth), M-mode4- Chest radiography antero-posterior view.was used by used it during inspiration andexpiration and then calculate the distance5- Routine laboratory investigations such asbetween the dome and bottom of thecomplete blood count, Liver functions,diaphragmatic line in freeze mode. M-moderenal profile, electrolytes.had more advantage than B-mode as it more6- Assessment of diaphragmatic mobilityusing baseline chest ultrasound aticdiaphragmaticmeasured by an M12L linear array probefour-chamberviewawaspreferred as all the patients wereformeasuringthefollowing parameters left ventricularejection fraction (LVEF) , Rt ventricularsize , Tricuspid annular plane systolicExcursion(TAPSE)andRightUltrasound with double probe (LOGIQ F8GE MEDICAL SYSTEMS CHINA CO.wasused(DT)wasforassessmentanterior axillary line at intercostal spacenumber 7 and number 8, givingan imagethat giving a complete picture about the liverand the lung and a zone of appositionbetween them using the B mode. Both of thepleural lining and the peritoneal liningappeared clearly as two approximatelyparallel echogenic lines. The space betweenthem resembles diaphragmatic thickness.ventricular systolic pressure (RVSP) .LTD)thickness(bandwidth: 5–13 MHz) that placed at theechocardiography,emphysematousless time consuming than B-mode.diaphragmaticthickness (DT).7- Transthoracicaccurate and easier for interpretation andofLeft ventricular ejection fraction (LVEF)was measured by M-mode, 2-D techniquesin the left parasternal short-axis and longaxis views. Computer software on the65
Benha medical journal, vol. 39. issue 1, 2022ECHOmachinewasusedtoassessquantitative left ventricular function.Right ventricular size was assessed bymeasurement of the right internal mid cavitydimension in the apical roni correction). Qualitative datawere presented as numbers and percentagesand were analyzed using the χ2 and Fisherexact tests. A P-value less than 0.05 wereconsidered significant, whereas a P-valueTricuspid annular plane systolic excursionless than 0.01 were considered highly(TAPSE) was measured by putting the M-significant.mode cursor on the lateral tricuspid annulus,and the maximum plane systolic excursionof the lateral annulus was calculated.Sample size was calculated according to apilot study for the 1st five patients in eachgroup. Assuming that the power of the studyRight ventricular systolic pressure (RVSP)was 80% and alpha error was 0.05 to detectwas calculated on the basis of the modifieda clinically significant difference betweenBernoulli equation and was considered to bethe measurement of diaphragmatic excursionequal to the sPAP, RVSP trans tricuspid(primary outcome) at 1st and 4th days. Thepressure gradient right atrial pressurecalculated effect size was 0.548. Twenty two,Trans tricuspid gradient is 4v2 (v peakpatients were calculated in each group. Wevelocity of tricuspid regurgitation, m/s),consideredRight atrial pressure was estimated from theovercome the dropout.25patientspergrouptoend- expiratory diameter of the inferior venacava.Results:Statistical analysis:-Study Involved 100 men patients, divided in4 groups according to mode of mechanicalAnalysis of data was performed by usingSPSS (version 16; SPSS Inc., Chicago,Illinois, USA). Quantitative data werepresented as mean and SD and wereanalyzed using a one-way analysis ofvariance test. Significant ANOVA test was66ventilation that used, each group involved25 patients, ranging in age between 40 to 78years with no significant value regarding ageand patient’s weight ranging between 70 to89 KG with no significant value regardingweight (table 1).
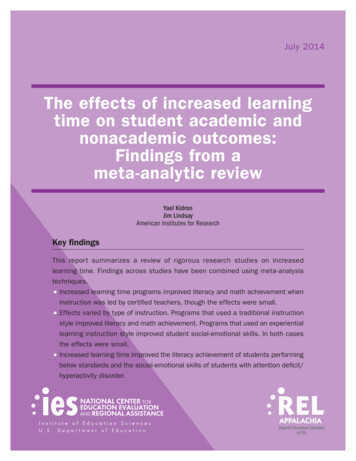
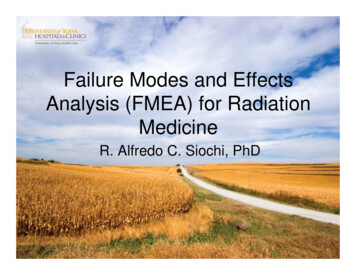
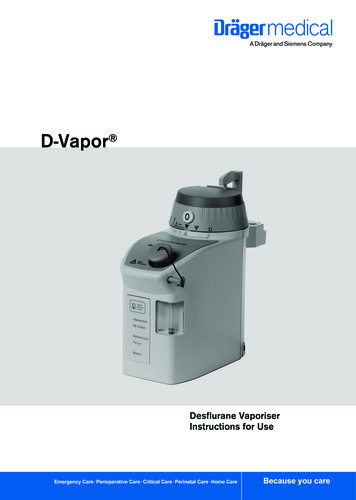
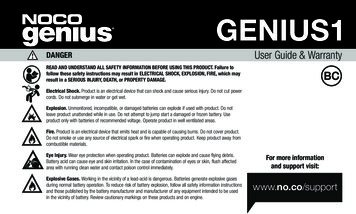
Mechanical ventilation moods and COPD, 2022Table 1- Detailed Demographic characteristics in 4 groupsGroup PCVGroupGroupGroupp-valueCVVPCV PSVVCV PSVAge(years)57.16 10.4356.84 10.5156.24 9.7557.12 9.530.98Weight(kg)77.88 4.3781.04 4.8178.96 4.9880.68 4.000.054Diaphragmaticexcursion(DE)wassignificant value in both first and secondmeasured for all patient in four groups at 1stgroups as there is decrease in DT with use ofthday and 4 day of MV on different modes,PCV and VCV alone but no significantin both first group (PCV) and second groupchanges occur in DT when PCV or VCV(VCV) there was significant decrease in DEmode combined with PSV mode (fig. 2).with use of PCV alone or VCV alone but onRegarding Echocardiographic parameters inthe contrary in both third and fourth groupform LVEF , RV size , TAPSE and RVSPthere was no significant changes in DEwere measured at 1st day and 4th day of MVwhen PCV or VCV mode combined withatPSV mode (fig 1).differentmodes,allfourEchocardiographic parameters results showAnd also results of diaphragmatic thicknessno significant changein all groups of(DT) measurement for all patient in fourdifferent modes of MV in both 1st and 4thgroups at 1st day and 4th day of MV onday.(fig 3,4,5 and 6).different modes, reveals that there isDE65****cm43At 1st day2At 4th day10Group PCV Group VCVGroupPCV PSVGroupVCV PSVFigure 1: Diaphragmatic Excursion Measurements in 4 groups at 1st and 4th day of MV67
Benha medical journal, vol. 39. issue 1, 2022DT3****2.5mm21.5At 1st day1At 4th day.0.50Group PCV Group VCVGroupPCV PSVGroupVCV PSVFigure 2: Diaphragmatic thickness Measurements in 4 groups at 1 st and 4th day of MV.LVEF7570%65At 1st day60At 4th day5550Group PCV Group VCVGroupPCV PSVGroupVCV PSVFigure 3:- LVEF Measurements in 4 groups at 1st and 4th day of MV68
Mechanical ventilation moods and COPD, 2022RV size3530mm252015At 1st day10At 4th day50Group PCV Group VCVGroupPCV PSVGroupVCV PSVFigure 4:- RV Size Measurements in 4 groups at 1st and 4th day of MVTAPSE2.52cm1.5At 1st day1At 4th day0.50Group PCVGroup VCVGroupPCV PSVGroupVCV PSVFigure 5:- TAPSE Measurements in 4 groups at 1st and 4th day of MV69
Benha medical journal, vol. 39. issue 1, 2022RVSP4035mmHg302520At 1st day15At 4th day1050Group PCVGroup VCVGroupPCV PSVGroupVCV PSVFigure 6: RVSP Measurements in 4 groups at 1 st and 4th day of MVDiscussionVentilating a COPD patient is often difficultearly initiate with spontaneous breathings,because the disease may not have aadjusting the work of breathingreversibleFurther,diaphragm is a fundamental respiratoryquantification and management of dynamicmuscle whose dysfunction may be veryhyperinflation (DH) at bedside is verycommon in patients undergoing mechanicaldifficult (9) so the choice of method andventilation. Diaphragmatic dysfunction isventilator parameters to be used must beassociatedspecific for each patient’s disease severity.ventilation and weaning failure (12). U/S isOne of the complications that should bewidely available inside the ICU that provideavoided is dynamic over-inflation anddirect, bed side , rapid visualization andconsequenthasassessment of the diaphragmatic mobilityventilatory and hemodynamic repercussionsand diaphragmatic function as the main(10). In patients on controlled mechanicalrespiratory muscle which may be used asventilation, there is serious diaphragmaticindicator for the weaning outcome (13).component.auto-PEEP,whichdysfunction and atrophy and, for thisattempts should be made for the patient to70withprolonged(11).ThemechanicalIn this study we assessed the impact ofdifferent modes of mechanical ventilation on
Mechanical ventilation moods and COPD, 2022diaphragmaticanddecrease of diaphragm thickness in aboutechocardiographic parameters of COPD10% in 47 (44%), and unchanged in 47patients by using diaphragmatic ultrasound(44%), and increased by more than 10% inand ECHO.13 (12%). On the other hand, thickness therewashigh significant decrease indiaphragmaticin non-ventilated patientsandIn the study which was was conducted fromdiaphragmatic thickness when controlledDecember 2018 to February 2019 at Ciptoventilation modeas pressure-controlledMangun kusumo National Hospital, thirtyventilation or Volume controlled ventilationventilated critically ill patients in the ICUused alone , in contrary no significantwere included (15). Baseline demographicchangediaphragmaticdata were collected. Baseline end-expiratoryparameters with use controlled ventilationdiaphragm thickness was measured withinandoneinbothpressureexcursionnot vary over time following extubation calalternatively. And also it showed that thereventilation and repeated every 24 hours forwas an insignificant correlation betweenfour days, and recorded of mortality andechocardiography as regard left ventricularduration of mechanical ventilation resultsejection fraction, right ventricular size,show no significant differences in thetricuspid annular plane systolic excursion,followingright ventricular systolic pressure andthickness according to gender, body massdifferent modes of mechanical ventilation.index and modified Rankin Score. TheThis was agreed with (14)study that involves107 patients were enrolled shortly afterinitiating ventilation along with 10 nonventilated patients inintensive care unit(control subjects). Diaphragm thickness andcontractileactivity(quantifiedbytheinspiratory thickening fraction) were dailymeasured by ultrasound. Results found thatduring71the first week of ventilation,dataasbaselinediaphragmsubjects were divided into two groups’duration of mechanical ventilation less thanseven days and duration of ventilation ofseven days or more, and showed that Themean baseline diaphragm thickness was 2.11 0.15 mm. and also decrease of diaphragmmuscle thickness that occurred in about 24hours. . It was found that rapid decrease indiaphragm muscle thickness corresponded
Benha medical journal, vol. 39. issue 1, 2022withlongerdurationofmechanicalventilation those worse outcomesspontaneous breathing trial with pressuresupport ventilation were enrolled. PatientsIt was revealed that the largest decrease inthickness occurred during the first 72 hoursof MV. Diaphragm atrophy occurs quicklyin mechanically ventilated patients and canwith airflow obstruction were excluded.These patients in pain and this may interferewith diaphragmatic mobility who excludedfrom our study (19).accurately be monitored using ultrasoundThis was in agreement with the study which(16).assessedA study found that decreasedtwenty-fouradultmechanicaldiaphragm and intercostal muscle thicknessventilated patients for more than 48 h andthat were measured on days 1, 3, 5, and 7consideredwith ultrasonography were frequently seenCardiorespiratory variables, oxygenation,in mechanical ventilated patient. They iogram findings were analyzed atventilation and increase length of ICU staysbaseline and after 30 minutes in pressure(17). Whereas in another study (18), it wassupport ventilation and T‐tube, found that nofound that low baseline diaphragm muscleechocardiographicmass occurred in prolonged mechanicalobservedventilation and associated with a higher riskventilation and T‐tube (20).withprolongedof in-hospital .DopplerweresupportThis was in the contrary to that study whichOn the contrary a study showed thatfound that spontaneous breathing trial (SBT)patients admitted to the ICU after majorinduced changes in central hemodynamicselective surgery who met criteria for aand helps in identifying patients at high riskspontaneous breathing trial with pressureof cardiac-related weaning failure whensupport ventilation, found that there was nodocumenting a depressed left ventricularstatisticallyinejection fraction (LVEF). This can bediaphragmatic excursion with increasingexplained by different groups of patients asventilator support. This difference may beall patients mechanically ventilated for moredue to difference in selection of the patientsthan 48 hours and fulfilled weaning criteriawhere patients admitted to the ICU afterincluding COPD patients, patients withmajor elective surgery who met criteria for aacute respiratory failure, patients with severe72significantchange
Mechanical ventilation moods and COPD, 2022sepsis and septic shock, cardiogenic shockand patients with neurological disorders andmechanical ventilation in COPD and asthma. MedIntensiva 35:288–98. [PubMed] [Google Scholar].stroke were enrolled in their study, also SBTwas performed over a 30 minute periodusing T-piece (21)This was highly in agreement with the studywhich proved that spontaneous breathing(SB) intensity is negatively associated withthe development of VIDD. Maintenance ofSB at an intensity of 60%-80% mayeffectively prevent the occurrence of VIDD(22).Conclusion:This study provided the impact of mobilityonandechocardiographic parameters and ticventilationweakness,butspontaneous mode of ventilation withpressure supportimprove diaphragmaticperformance by improving lung volumesand ventilation as observed and esan ,Cristian Oancea, rache (2014) : Diaphragmaticmuscle ultrasound in COPD patients .EuropeanRespiratory Journal .44. 802.3-Wellington Pereira, Dos Santos Yamaguti,Elaine Paulin, Simone Shibao, Maria CristinaChammas (2008): Air trapping: The major factorlimiting diaphragm mobility in chronic obstructivepulmonary disease patients.Respirology.13.138-144.4. Daniels LB, Krum men DE, Blanchard DG(2004): Echocardiography in pulmonary vasculardisease. Cardio Clin ;22:383–99. [PubMed] [GoogleScholar].5. Caille V, Amiel JB, Charron C, Belliard G,Vieillard-BaronA,VignonP(2010):Echocardiography: a help in the weaning process.Crit Care ;14(3):R120. DOI: 10.1186/cc9076. [PMCfree article] [PubMed] [CrossRef] [Google Scholar].6. Soummer A, Perbet S, Brisson H, Arbelot C,Constantin JM, Lu Q (2012): Ultrasoundassessment of lung aeration loss during a successfulweaning trial predicts postextubation distress*. CritCare Med.;40(7):2064–2072. [PubMed] [CrossRef][Google Scholar].7. Kim WY, Suh HJ, Hong SB, Koh Y, Lim CM(2011) : Diaphragm dysfunction assessed byultrasonography: influence on weaning 2627–2630.[PubMed][CrossRef][Google Scholar].References:8. Mayo P, Volpicelli G, Lerolle N, Schreiber A,DoelkenP,Vieillard-BaronA(2016):Ultrasonography evaluation during the weaningprocess: the heart, the diaphragm, the pleura and thelung. Intensive Care Med; 42(7):1107–1117.[PubMed] [CrossRef] [Google Scholar].1. García Vicente E, Sandoval Almengor JC, DíazCaballero LA, Salgado Campo JC (2011): Invasive9-Qaseem A, Wilt TJ, Weinberger SE, HananiaNA, Criner G, van der Molen T.(2011): Diagnosisparameters changes occurred on differentmodes of mechanical ventilation.73
Benha medical journal, vol. 39. issue 1, 2022and management of stable chronic obstructivepulmonary disease: A clinical practice guidelineupdate from the American College of Physicians,American College of Chest Physicians, AmericanThoracic Society, and European Respiratory Society.Ann Intern Med; 155:179-9.16-Philippe G. Jorens , Tom Schepens, WalterVerbrugghe, (2015): The course of diaphragmatrophy in ventilated patients assessed withultrasound. Critical Care volume, 19: 422.10-Jezler S, Holanda M, José A (2007): ConsensoBrasileiro de Ventilação Mecânica. Ventilaçãomecânica na doença pulmonar obstrutiva crônica(DPOC) descompensada. J Bras Pneumol. 2007;33(1):111–8.17-Jun Oto , Nobuto Nakanishi , Yoshitoyo Ueno ,Emiko Nakataki , Taiga Itagaki and MasajiNishimura (2019):Change in diaphragm andintercostal muscle thickness in mechanicallyventilated patients: a Journal of Intensive care 18:3.11-Vivier E, Mekontso Dessap A, Dimassi S,Vargas F, Lyazidi A, Thille AW, et al. (2012):Diaphragm ultrasonography to estimate the work ofbreathing during non-invasive ventilation. IntensiveCare Med; 38:796–803.18-Michael C. Sklar, Martin Dres, Eddy Fan(2020): Association of Low Baseline DiaphragmMuscle Mass With Prolonged Mechanical Ventilationand Mortality Among Critically Ill Adults JAMAnetwork open ;3(2).12- Giovanni Ferrari, Giovanna De Filippi,Fabrizio Elia, Francesco Panero, GiovanniVolpicelli, Franco Aprà (2014): Diaphragmultrasound as a new index of discontinuation frommechanical ventilation. Critical Ultrasound Journal,6:8-9.19-Umbrello M, Paolo F, Daniela L, Andrea G,Ilaria P, Angelo P, et al. (2015): Diaphragmultrasound as indicator of respiratory effort incritically ill patients undergoing assisted mechanicalventilation: a pilot clinical study, Critical Care19:161.13-Osman A, Hashim R (2017): Diaphragmatic andlung ultrasound application as new predictive indicesfor the weaning process in ICU patients. TheEgyptian Journal of Radiology and NuclearMedicine, n107–111.14-Niall D Ferguson , Ewan C Goligher, EddyFan, Margaret S Herridge, Alistair Murray,Stefanie Vorona, Debbie Brace (2015): evolution ofdiaphragm thickness during mechanical ventilation.Impact of inspiratory effort, American journal ofrespiratory and critical care medicine 192 (9), 1080108821-Caille V, Arniel JB, Charron C, Belliard G,VieillardBaronA,VignonP.(2010):Echocardiography: a help in the weaning process.Crit Care.; 14:120, doi: 10.1186/cc9076.15-Bram Kilapong, Dita Aditianingsih, RudyantoSedona, Adhrie Sugiarto, Thariqah Salamah(2021): Diaphragm muscle thinning in mechanicallyventilated critically ill patients JPMA. The Journal ofthe Pakistan Medical Association Volume 712: 2.M, Silvia R, Janete S, Deise M,,andAntonio N.(2011): Echocardiographicduring weaning from mechanical.Clinics (Sao Paulo). 2011 Jan; 66(1):22-Luo Z, Han S, Sun W, Wang Y, Liu S, Yang L(2020): Maintenance of spontaneous breathing at anintensity of 60%–80% may effectively ysfunction. PLoS ONE 15: (3).To cite this article: Ahmed G. EL gazzar, Tarek S. Essawy, Basem M. Aglan, Emad F. Ibrahim, .Enas W. Mahdy. Effect of Different Modes of Mechanical Ventilation on Chronic ObstructivePulmonary Disease Patients with Respiratory Failure Regarding Echocardiographic Changes andDiaphragmatic Ultrasound. BMFJ 2022;39 (1): 62-74. DOI: 10.21608/bmfj.2021.102965.150874
Mechanical ventilation moods and COPD, 2022 63 weaning process. In addition, we concluded that the echocardiographic finding was not affected