Transcription
JMSCR Vol 07 Issue 01 Page 1120-1128 January2019www.jmscr.igmpublication.orgIndex Copernicus Value: 79.54ISSN (e)-2347-176x ISSN (p) 2455-0450DOI: ography vs MRCP in Evaluation of Obstructive JaundiceAuthors1*Dr Sailendra Kumar Prusty , Dr Savitri Bhagat2, Dr Braja Behari Panda31PG Resident, VIMSAR, BurlaProfessor & H.O.D., Department of Radiodiagnosis, Veer Surendra Sai Institute of Medical Sciences andResearch (VIMSAR), Burla, Sambalpur, Odisha 7680173Associate Professor, Department of Radiodiagnosis, Veer Surendra Sai Institute of Medical Sciences andResearch (VIMSAR), Burla*Corresponding AuthorDr Sailendra Kumar PrustyPG Resident, VIMSAR, Burla, Sambalpur, Odisha 768017, IndiaEmail: prusty.sailendra@gmail.com, Mobile- 9861430101AbstractObstructive jaundice results from obstruction to the flow of bile into the duodenum. The study was conductedto evaluate imaging findings in USG and MRCP in 46 cases of suspected biliary obstruction duringNovember 2016 to October 2018. This cross sectional analytic study was conducted in Department ofRadiodiagnosis, VIMSAR, BURLA. All patients were subjected to USG & MRCP. Results were compared andfound MRCP superior to USG in diagnosis of obstructive jaundice.Keywords: Obstructive jaundice, USG, MRCP.2IntroductionJaundice, also known as icterus, is yellowdiscoloration of the skin and sclera due to highbilirubin levels in the blood. It may be Hemolytic,Hepatocellular or Obstructive.Obstructive jaundice results from obstruction tothe flow of bile into the duodenum. Obstructivejaundice is not a disease in itself but a symptom ofan underlying condition involving the liver, thegallbladder or the pancreas. It will usually requiresurgical intervention, and is also known assurgical jaundice. It is important to distinguishbetween the possible causes of obstructivejaundice.So, it is mandatory to determine pre-operativelythe existence, the nature and site of obstruction.USG has been always considered the first choicetechnique in the study of biliary obstructivedisease, due to its accessibility, speed, ease ofperformance and low cost1. Traditional ComputedTomography (CT) scan is usually consideredmore accurate than US for helping determine thespecific cause and level of obstruction2.Ultrasound is used as an initial modality toconfirm or exclude duct obstruction, which it doeswith at least 90% accuracy3. The range ofapplication of CT has been partially restricted byMRCP4. MRCP techniques have greatly evolved,providing high resolution images of the biliarytree with short exam duration, while remainingnon invasive without contrast medium injection5 .Dr Sailendra Kumar Prusty et al JMSCR Volume 07 Issue 01 January 2019Page 1120
2019JMSCR Vol 07 Issue 01 Page 1120-1128 JanuaryAims & Objectives To evaluate the cause and location ofbiliary obstruction To correlate MRCP with Ultrasonographyin diagnosis of obstructive jaundice Tofindouttypesoflesion(benign/malignant) causing obstructivejaundice, age & sex distribution.Material and MethodsPatients with clinical and laboratory featuressuggestive of obstructive jaundice who werereferred to Department of Radiodiagnosis,VIMSAR, Burla during the study period of 2years (November 2016- October 2018) wereincluded in the study.Exclusion criteria Patients having cardiac pacemakers andelectromagnetic implants. Patients with claustrophobia Patients not giving the consent for study. No obstructive pathology detected in USG46 patients included in the study were subjected toabdominal ultrasound followed by MRCP(Ultrasound by Philips HD 7 machine and GELOGIQ F8 Expert and MRCP by 1.5 Tesla GEsigna machine). Various features of obstructivejaundice like presence and level of obstruction,cause of obstruction, extent of obstruction andother associated findings were studied on both.MRCP findings were compared with USGfindings. The findings were tabulated andanalyzed.ResultsOut of 46 patients evaluated, maximum numbersof cases were observed in 35-75 years of agegroup. Majority of benign cause were seen in 1150 years of age group while malignant causeswere more common between 41-70 years of agegroup. Females (52.17%) were slightly more thanthe males (47.82%) in the study population.Jaundice, pain abdomen and vomiting were thefrequent presenting complaints while fever, loss ofappetite and distension of abdomen we lesscommon. Most of patients presented withcombination of symptoms (84%).Majority of pathologies observed were benign(63.04%). Most common benign disorderobserved wascholedocholithiasis(34.78)followed by benign strictures (10.86%).Choledocholithiasis and cholelithiasis were morecommonly observed in female patients. Leastcommonly observed benignpathologies werecholedochal cyst (8.69%) and pseudocyst(8.69%).Malignant pathologies were observed in 36.95%patients. Most common malignant pathology seenwas Cholangiocarcinoma (17.39%) followed byperiampullary carcinoma (8.69%), carcinomahead of pancreas (4.34%) and carcinomagallbladder (4.34%). Cholangiocarcinoma andperiampullary carcinoma were more predominantin males. Least commonly observed malignantpathology was one case of metastatic lymph nodes(2.17%) which was found in female patient.Table 1 Age Distribution of Patients StudiedAgeinYears 1516-2526-3536-4546-5556-6566-7576-85TotalNumber 5.2123.9126.082.17100Table 2 Gender Distribution of Patients StudiedGenderMaleFemaleTotalNumber of patients222446Percentage47.8252.17100Table 3 Clinical Symptom Wise Distribution ofPatients at PresentationClinical SymptomsJaundicePain in abdomenVomitingLoss of appetiteFeverDistension of abdomenLoss of weightDr Sailendra Kumar Prusty et al JMSCR Volume 07 Issue 01 January 2019No. Of .2110.868.69Page 1121
JMSCR Vol 07 Issue 01 Page 1120-1128 January2019Table 4 Benign Versus Malignant Causes of Biliary Obstruction in the Studied PopulationType of LesionBenignMalignantTotalNo. of Cases291746Percentage63.0436.95100Graph 1 Various Causes of Biliary Obstruction in the Studied PopulationGB and CBD calculi2 14CholangiocarcinomaBenign Stricture162Choledochal cyst4Periampullary CaPancreatic carcinoma4PseudocystCarcinoma gall bladder58Metastatic lymph nodesTable 5 Benign Causes of Biliary Obstruction in the Studied PopulationPATHOLOGYGB and CBD calculiBenign StricutreCholedochal cystPseudo cystUSG (25)15343%51.7210.3413.7910.34MRCP (30)17544%58.6217.2413.7913.79SURGERY (29)16544%55.1717.2413.7913.79Table 6 Malignant Causes of Biliary Obstruction in the Studied PopulationPathologyCholangiocarcinomaPeriampullary CarcinomaCarcinoma head of pancreasCarcinoma gall bladderMetastatic lymph nodesUSG (13)71221%41.175.8811.7611.765.88MRCP (16)83221%47.0517.6411.7611.765.88Surgery (17)84221%47.0523.5211.7611.765.88Table 7 Comparison of Diagnostic Values of USG and MRCP in Benign Causes of Biliary ObstructionModalityUSGMRCPSensitivity (%)8496.55Specificity (%)100100Accuracy (%)8696.66Table 8 Comparison of Diagnostic Value of USG and MRCP in Malignant Causes of Biliary ObstructionModalityUSGMRCPSensitivity (%)84.6193.75Specificity (%)100100Diagnostic accuracy (%)88.2394.11Dr Sailendra Kumar Prusty et al JMSCR Volume 07 Issue 01 January 2019Page 1122
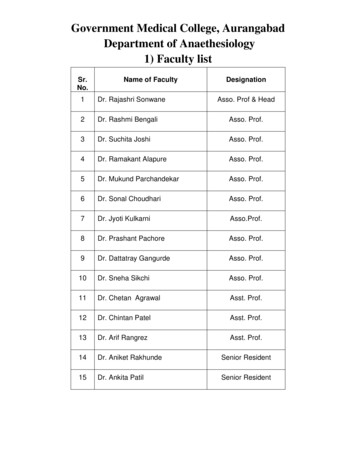
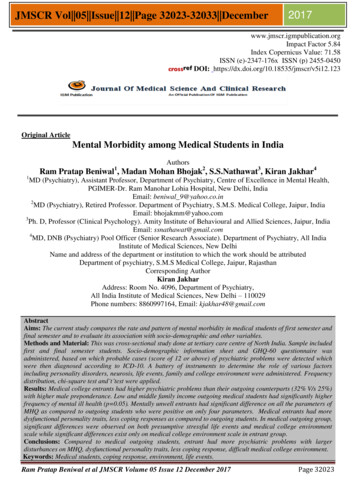
JMSCR Vol 07 Issue 01 Page 1120-1128 January2019Fig 1 CholedocholithiasisFigure (1A) USG showing echogenic calculus with PAS in distal CBDFigure (1B) MRCP image showing T2 hypointense filling defect in distal CBDFig 2 CholangiocarcinomaFigure (2A) USG showing echogenic lesion in distal CBD with dilatation of bile ducts proximal to it.Dr Sailendra Kumar Prusty et al JMSCR Volume 07 Issue 01 January 2019Page 1123
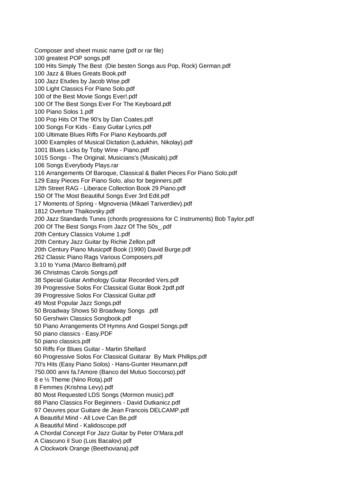
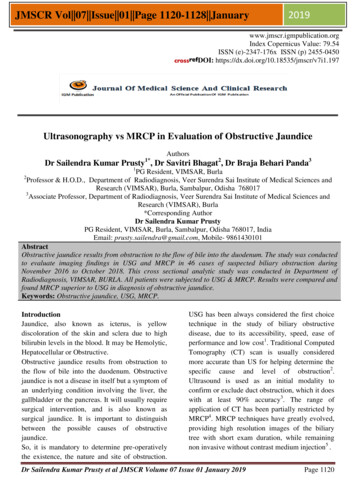
JMSCR Vol 07 Issue 01 Page 1120-1128 January2019Fig 2 (2B & 2C) MRCP showing illdefined heterogenous intensity lesion in the region of distal CBD.Moderate dilatation of proximal CBD and IHBR noted.Fig 3 Periampullary CarcinomaFig 3 (3A & 3B)USG showing hypoechoic lesion in periampullary region with dilatation of CBD & PD.Fig 3 (3C & 3D) MRCP showing illdefined T2 hypointense lesion at ampullary region with eccentricduodenal wall thickening. Dilated CBD with sudden cut off at periampullary region. PD is also dilated(double duct sign positive).Dr Sailendra Kumar Prusty et al JMSCR Volume 07 Issue 01 January 2019Page 1124
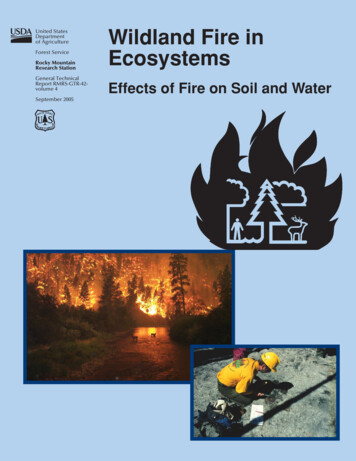
JMSCR Vol 07 Issue 01 Page 1120-1128 January2019Fig 4 Carcinoma GallbladderFig 3 (4A) USG showing obstructive billiopathy secondary to invasion of CHD by GB neck massFig 4 (4B & 4C) MRCP showing iso to hypointense lesion in the region of neck of gallbladder, infiltratinginto the CHD and thereby causing proximal dilatation of IHBR.DiscussionFrom table no 1&2- Out of 46 patients evaluated,22 (47.82%) patients were male and 24 (52.17%)patients were female. The mean age of studypopulation was 45.5 (range 4-82 years). Theaverage age of patients with benign lesions was inthe fourth decade while that of malignant lesionwas in the sixth decade.Upadhyaya et al6 studied 100 patients out ofwhich 46% were male and 54% were female,Ferrari et al7 studies 131 patients; distribution ofmale patients in Ferrari et al was 47% while thatof female 53%. Soto et al8 studies 43 patients outof which male and 53% female. In our study of 46patients, 48% were male and 52% were femalepatients. Percentage distribution of male to femaleis almost equal on our study. From above tablesex distribution in our study closely matches withUpadhaya et al, Ferrari et al and Soto et al.From table no 3- Regarding clinical symptomsmost common clinical presentation in our studywas jaundice seen in 41 (89%) patients followedby pain abdomen seen in 21 (45.65%) patients,while least common presentation was loss ofweight seen in 4 (8.7%) patients. Almost allpatients presented with combination of symptoms.Schwartz et al9 in his study reported that mostcommon presentation was jaundice seen in 68%patients followed by pain in abdomen seen in25% patients which is similar with our study.From table no 4- USG was done prior to MRCPfor all patients. 29(63%) benign and 17(37%)Dr Sailendra Kumar Prusty et al JMSCR Volume 07 Issue 01 January 2019Page 1125
JMSCR Vol 07 Issue 01 Page 1120-1128 Januarymalignant causes of biliary obstruction weredetected in the study population. Most commonpathology detected in our study is a benign entity,choledocholithiasis, constituting 16 cases of ourstudy population followed by 8 cases ofcholangiocarcinoma, a malignant pathology.From table no 5- Sixteen cases ofcholedocholithiasis were detected in our studypopulation. While USG diagnosed 15 lesions withcholelithiasis, it had difficulty in diagnosing distalCBD calculi which was easily picked up byMRCP. Our study is in concordance with Guibaudet al10 1995; in their study they found an accuracyof 100% in detecting CBD calculi on MRCP incases with equivocal sonographic results. MRCPclearly shows the IHBR dilatation, caliber of CBDand the site of the calculus, especially in the distalCBD which is difficult to visualize on ultrasound.Of the 16 patients diagnosed with CBD and GBcalculi, MRCP had accurately diagnosed all the 16cases. Our study is in concordance with Soto et al82000; In their study they found, sensitivity of 94%and specificity of 100% for detecting biliarycalculi on MRCP. Varghese et al11 who reported91% sensitivity, specificity of 98% and diagnosticaccuracy of 97% on MRCP. Sugiyama et al12reported 91% sensitivity, specifity of 100% anddiagnostic accuracy of 97% on MRCP.71Four cases of anatomic variants, choledochal cystswere present in our study. All 4 cases werediagnosed correctly by MRCP. Our study is inconcordance with Bhatt et al13 in their study theyfound 100% accuracy for MRCP in diagnosinganatomical variants.In four cases of choledochal cyst seen in ourstudy, MRCP yielded diagnostic information byproviding exact anatomical map for presurgicalevaluation. Bhatt et al13 reported choledochal cystin 10% of cases in his study. Our findings areconsistent with Bhatt et al.Four cases (28.69%) of pseudocyst resulting inbiliary obstruction were present in our studywhich was correctly diagnosed by MRCP.2019From Table 6- In our study of 46 cases,cholangiocarcinoma was seen in 8 (17.39%)casesand Periampullary carcinoma 4(8.69%) cases.Schwartz et al9 in his study of 32 cases reportedcholangiocarcinoma in 21.8% cases, Ca pancreasinn 37.5% cases and Periampillary Ca in 6.2%cases. Soto et al8 in his study of 43 cases reportedcholangiocarcinoma in 13.9% cases, Ca pancreasin 18.6% cases and Priampullary Ca in 9.3%cases.Percentage distribution of cholangiocarcinoma inour study matches with Schwartz et al. Percentagedistribution of periampullary Carcinoma in ourstudy matches with Soto et al. Overall Percentagedistribution of malignant pathologies in our studyclosely matches with Soto et al.Among the 2 cases of carcinoma head of thepancreas, MRCP accurately diagnose all 2 casesof carcinoma head of the pancreas. Two cases ofcarcinoma gall bladder and another case ofMetastatic lymph nodes causing biliaryobstruction were diagnosed by both the modalitiesachieving 100% accuracy.In our study final diagnostic criteria ishistopathology and postoperative findings. In ourstudy of 46 cases, surgery/Histopathologicalcorrelation was done in 41 cases. Out of 46 cases,4 cases were inoperable tumours. In these casesdiagnosis was confirmed by FNAC. However in 1case of Caroil’s disease surgery/Histopath/FNACwas not advisable hence, MRCP diagnosis wasconsidered as final diagnostic.Depending upon these 45 case in whichsurgery/histopathological/FNAC correlation wasdone, following statistical values are derived.From Table no 7 - Sensitivity, specificity anddiagnostic accuracy for benign pathologies in ourstudy was 84%, 100% & 86% respectively onultrasound. On MRCP sensitivity was 96.55% ,specificity was 100% and accuracy was 96.66%for cases with benign conditions.Verma et al14 demonstrated the sensitivity andspecificity of 85.3% and 88.4% on ultrasound,92.3% and 86% on MRCP respectively fordetecting the benign etiology of obstruction.Dr Sailendra Kumar Prusty et al JMSCR Volume 07 Issue 01 January 2019Page 1126
JMSCR Vol 07 Issue 01 Page 1120-1128 JanuaryFerrari FS et al7 demonstrated similar findings forbenign lesions in their study. The diagnosticaccuracy, sensitivity and specificity of USG was78.62%, 16.67%, 97.29% and MRCP was93.13%, 90%, 94% respectively.From Table no 8- Sensitivity and specificity formalignant pathologies in our study was 84.61%and 100% respectively on USG while that onMRCP was 93.75% and 100% respectively.Likelihood ratio can’t be calculated as specificityis 100% From this it is clear that MRCP is ies than USG, while specificity of bothUSG and MRCP remains same.Verma et al14 demonstrated the sensitivity andspecificity of 88.4% and 85.3% on ultrasound,86% and 92% on MRCP respectively for detectingthe malignant etiology of obstruction . Ferrari FSet al7 demonstrated the diagnostic accuracy,sensitivity and specificity of USG 93.13%,61.12%, 98.23% and 93.13%, 90%,94% ofMRCP respectively.ConclusionMRCP was superior to Ultrasound. Ultrasoundstill remains the primary investigative modality ofchoice. MRCP serves as an accurate and noninvasive, non ionizing imaging method forevaluation of pancreatico-biliary anatomy andpathology. It is very useful tool in case of obesepatients. MRCP is the modality of choice foroptimal characterization of the causative lesions inmost of the cases obstructive jaundice whichallows safe surgical management decisions.Potentially useful in patients undergoing biliaryenteric anastomosis for knowing the level andextent of strictures.References1. Hakansson K, Ekberg O, Hakansson HO,Leander P: MR and ultrasound inscreening of patients with suspected biliarytract disease. Acta Radiol. 2002; 43:80–86.2. Fleischmann D, Ringl H, Schofl R, PotziR, Kontrus M, Henk C, et al. Three2019dimensional spiral CT cholangiography inpatients with suspected obstructive biliarydisease: comparison with logy. 1996; 198: 861-8.3. Gibson RN, Yeung E, Thompson LN, CarrDH, Benjamin IS, Blumgart LH, AllisonDJ. Bile duct obstruction: Radiologicevaluation of level, cause, and tumourresectability. Radiology. 1986;160:43-7.4. Zandrino F, Benzi L, Ferretti ML, et al.Multislice CT cholangiography withoutbiliary contrast agent: technique and initialclinical re- sults in the assessment ofpatients with biliary obstruction. EurRadiol. 2002; 12: 1155–61.5. Reinhold C, Bret PM. MR cholangiopancreatography. Abdom Imaging. 1996;21: 105-16.6. Upadhayay V, Upadhyaya DN, UnsariMA, Shukla VK. Comparative assessmentof imaging modalities in biliaryobstruction. Indian J Radiol Imaging2006;16:577-82.7. Ferrari FS, Fantozzi F, Tasciotti L, VigniF, Scotto F, Frasci P. US, MRCP, CCTand ERCP: A comparative study in 131patients with suspected biliary obstruction.Med Sci Monit 2005;11:MT8-18.8. Soto JA, Alvarez O, Múnera F, Velez SM,Valencia J, Ramírez N. Diagnosing bileduct stones: Comparison of unenhancedhelical CT, oral contrast-enhanced CTcholangiography, and MR cholangiography. AJRAm JRoentgenol2000;175:1127-34.9. Schwartz LH, Black J, Fong Y et al.gallbladder carcinoma Findings at MRimaging withMRcholangiopancreatography. J Comput Assist Tomogr2002;26:405-410.10. Guibaud L, Bret PM, Reinhold C et al(1994) Diagnosis of choledocholithiasis:value of MR cholangiography. AJR Am JRoentgenol 163:847–850Dr Sailendra Kumar Prusty et al JMSCR Volume 07 Issue 01 January 2019Page 1127
JMSCR Vol 07 Issue 01 Page 1120-1128 January201911. Verghese J.C, Liddell R.P, Rarrell et al.The diagnostic accuracy of magneticresonance cholngiopancreatography andultrasoundcomparedwithdirectcholangiography in the detection ofcholedocholithiasis. Clinical Radiology.1999;54(9):604-614.12. Sugiyama M, Atomi Y & Hachiya J et al.Magnetic resonance cholangiographyusing half-Fourier acquisition for diagnosing choledelocholithiasis. AmericanJournal of Gastronterology.1998; 93(10):1886-1890.13. Bhatt C, Shah PS, Prajapati HJ, Modi J etal. Comparison of Diagnostic Accuracybetween USG and MRCP in Biliary andPancreatic Pathology. Ind J Radiol Imag.2005; 15:177-181.14. Verma SR, Sahai SB, Gupta PK. MunshiA, Verma SC, Goyal P, obstructiveJundice- Aetiological Spectrum , clinicalbiochemical and Radiological EvaluationAt A Teriary Care Teaching Hospital. TheInternet Journal of Tropical Medicine 2010Volume 7 Number 2.Dr Sailendra Kumar Prusty et al JMSCR Volume 07 Issue 01 January 2019Page 1128
(Ultrasound by Philips HD 7 machine and GE LOGIQ F8 Expert and MRCP by 1.5 Tesla GE signa machine). Various features of obstructive jaundice like presence and level of obstruction, cause of obstruction, extent of obstruction and other associated findings were studied on both.