Transcription
Operations Research:Decision Support Toolsto Reduce Wait TimesMichael W. CarterHealth Care Resource Modelling GroupMechanical and Industrial EngineeringUniversity of Torontoe-mail: carter@mie.utoronto.caApril 1, 2005Operations Research Models for Wait Lists1
OutlineBrief intro to Operations Researchz Queueing Theoryz– Examples and LimitationszSimulation Modeling– Continuous models (System Dynamics)– Discrete Event modelszMathematical Programming– Matching Capacity to DemandApril 1, 2005Operations Research Models for Wait Lists2
Brief Intro to O.R.Started during WWII in UKz Quantitative analysis: math, physics, statsz Canadians involved from the startzApril 1, 2005Operations Research Models for Wait Lists3
Queueing Theory PrimerQueues are everywhere: bank machines,grocery stores, airports, phone calls,elevators, EDs, etc.z Basic idea:z– Given average service and arrival rates– can calculate average wait time, expectedqueue size, utilization rate, and more– Several assumptions involvedApril 1, 2005Operations Research Models for Wait Lists4
Simple examplezBank machine:– Average service rate:z30 people/hour [2 minutes each]– Average arrival rate:z15 people/hour [one every 4 minutes]– Utilization – 50%April 1, 2005Operations Research Models for Wait Lists5
Some AssumptionsFirst come – first servedz Independentz– Customs at airport?– Prescheduled appointments?zIdentically distributed– Different times of day?Service rate is faster than the arrival ratez Everyone is served – no “reneging”zApril 1, 2005Operations Research Models for Wait Lists6
Three Types of Health Queues1. Short term: “Daily” problem– Average service rate faster than arrival rate2. Long term: “Monthly” problem– Average service rate equals arrival rate– Queue size never changes!3. Catastrophe: Queue grows out of control– Average arrival rate faster than service rate!April 1, 2005Operations Research Models for Wait Lists7
Problem #1Queueing theory formulae only apply tothe short term problem!z Assumes that the “server” has some idletimez Otherwise, impossible to predict queuecharacteristics!zApril 1, 2005Operations Research Models for Wait Lists8
Solution?zIf you want no idle time, you must have:– A buffer of people on the wait list– Arrival rate Service rateOccasionally, you may need to provideadditional capacity to reduce the wait listz Of course, you must know the arrival rate!zApril 1, 2005Operations Research Models for Wait Lists9
Problem #2For the long term problem, in mostsituations, we have little or no knowledgeof Arrival volumes!z Wait lists are hiding in doctors’ officeszApril 1, 2005Operations Research Models for Wait Lists10
Problem #3For the short term problem, in mostsituations, we have little or no knowledgeof service rates!z We know what was booked, but typically,no one records how long appointmentsactually took.zApril 1, 2005Operations Research Models for Wait Lists11
Problem #4zEven if the average demand is equal to theaverage capacity, if there is variationqueues will form because unmet demand iscarried forward, but unfilled capacity islost.April 1, 2005Operations Research Models for Wait Lists12
Problem #5zThere are perverse incentives for having aqueue:– it keeps a service busy and apparently essentialto the service– waiting list initiatives are awarded to serviceswith queuesApril 1, 2005Operations Research Models for Wait Lists13
Have you ever counted them?Nuclear Medicine at William Oslerz Endocrinology at the Cleveland ClinczApril 1, 2005Operations Research Models for Wait Lists14
CPOE at SunnybrookzComputerised Physician Order Entry– In-patient medication orderszzQuestion: How many computer terminalsshould be allocated to each ward?“Docs should never have to wait for acomputer”April 1, 2005Operations Research Models for Wait Lists15
CPOE at Sunnybrookzzzcompare expected waiting time andresulting clinician “ill-will” with the costof purchasing additional workstations;A maximum acceptable waiting time usedto calculate the minimum number ofworkstationA combination of the two approachesApril 1, 2005Operations Research Models for Wait Lists16
Prioritized WaitlistzPriorities make the average worse!– Basic rule in scheduling: SPT – doing “ShortestProcess Time” jobs first will minimize theaverage waiting time.– Adding priorities (e.g., in the ED) often meansthat the short ones go last.– Some priorities are medically necessary – butshould be used with caution!April 1, 2005Operations Research Models for Wait Lists17
Simcoe County CCACzServices– Nursing– Therapies– Personal SupportzMeals, bathing, dressing, cleaning, living skills .– Placement ServiceszApril 1, 200521 Long term care facilities – 1,763 bedsOperations Research Models for Wait Lists18
Simcoe County CCACzTherapies–––––Occupational therapy (OT)Physiotherapy (PT)Diet/Nutrition (NUT)Speech pathology (SP)Social work (SW)April 1, 2005Operations Research Models for Wait Lists19
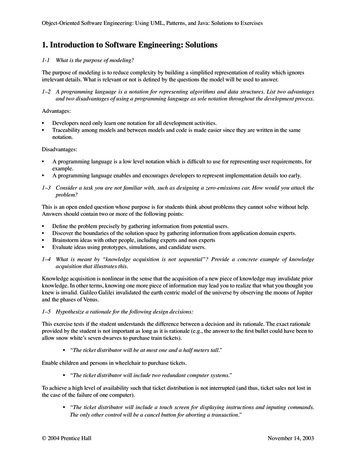
Total Cost to Clear Wait List 250,000 200,000 150,000Cost 100,000 50,000 0Pr 1April 1, 2005Pr 1 2Pr 1-3Pr 1-4Operations Research Models for Wait Lists20
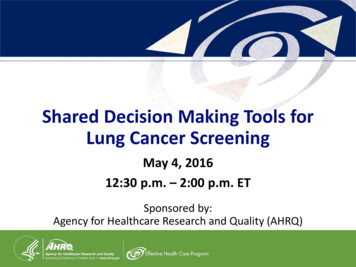
OT- Priority 1- Forecast 1311975310Actual DataForecasted Data
Estimating Waiting TimeQueueing Theory: Given the customerarrival rate , and the system servicerate , we can analytically compute anumber of statistics (expected wait time,expected number of patients waiting,etc.) for each service.z This can be extended to multiple priorityqueueszApril 1, 2005Operations Research Models for Wait Lists22
Monthly Arrival & Service RatesServicePriority 1(λ1)Priority 2(λ2)Priority 3(λ3)Total(λ)ServiceRate 9.3915.68SW16.518.297.542.2936.06
Decision Support ToolszzModel 1: Given limits on the queue foreach priority (maximum acceptablewait times) compute the minimumservice level required.Model 2: Given a fixed service level( ), compute the expected wait times.April 1, 2005Operations Research Models for Wait Lists24
Network of QueueszzzzMany queues involve a sequence of wait lists:– ED ICU Ward ALC LTC– GP Surgeon Lab Surgeon OR etcEach one is a queue – each has an arrival rate andservice rate/LOSWe typically don’t know arrival or service rate formany partsAnalysis is more complex (computer simulation)April 1, 2005Operations Research Models for Wait Lists25
Hospital Patient Simulation1989: Nursing Crisis in Ontarioz Ont. Min. of Health & Five Hospitalsz Prof. Linda O’Brien-Pallas (Nursing)z 1995: Efficient Use of Resources!z “What if?” Simulation toolzApril 1, 2005Operations Research Models for Wait Lists26
CHEO: Emergency RoomChildren’s Hospital of Eastern Ontario:Ottawa 1993z Paediatric Teaching Hospitalz 50,000 patient visits per year in the ERzApril 1, 2005Operations Research Models for Wait Lists27
CHEO: Waiting Times (1993)% pat's.April 1, 2005504540353025201510500-1 hr 1-2 hr 2-3 hr 3-4 hr 4 plusOperations Research Models for Wait Lists28
CHEO: Emergency Room20 % of patients wait over two hoursz Eleven suggestions by staffz Simulation used to evaluate scenariosz Fast track clinicz New Casualty Officerz Staggered start timeszApril 1, 2005Operations Research Models for Wait Lists29
Generalized Simulation of OntarioEmergency Departments: Toward a BetterUnderstanding of Patient Length-of-Stay:The CROWDED studyMW Carter1, DJT Fernandes1,2, MJ Schull2, GS Zaric3, G Geiger41 HealthcareProductivity Laboratory, Mechanical & Industrial Engineering, U of Toronto;2 Institute for Clinical Evaluative Sciences;3 Richard Ivey School of Business, University of Western Ontario4Sunnybrook and Women’s College Health Sciences CentreApril 1, 2005Operations Research Models for Wait Lists30
BackgroundzzzzzED overcrowding and waiting - majorproblemMost analysis based on LOS dataA few simulation models - typically modelLOSDoes not help us analyze improvementsWanted to understand what happens in an EDApril 1, 2005Operations Research Models for Wait Lists31
CIHR & SSHRC fundingCROWDED study: Causes and Relationshipsof Overcrowding and Waiting in DifferentEmergency Departmentsz Two full time research assistants for one yearz One full time PhD student: DominicFernandesz Cross section of hospitals in type & geographyz– 3 rural, 4 community and 3 teaching from eachgeographic area of OntarioApril 1, 2005Operations Research Models for Wait Lists32
The Hospital PartnerszzzAcademic– Kingston General– Sunnybrook &Women's– London HSCRural– Quinte Health Corp– Stevenson Memorial– South MuskokaApril 1, 2005Community– Royal Victoria Barrie– Sudbury Regional– MarkhamStouffville– Windsor RegionalOperations Research Models for Wait Lists33
Models for Assessment ofBlood Product Shortages: Likelihoodand ConsequencesSomayeh Sadat, Renata Kopach, Daniel FrancesDepartment of Mechanical & Industrial EngineeringUniversity of TorontoApril 1, 2005Operations Research Models for Wait Lists34
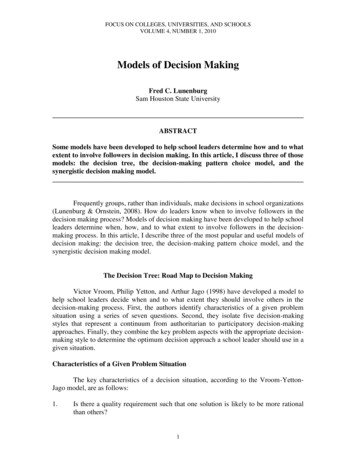
RationalNeed to quantify the incidence and medicalconsequences of blood products shortagesTaking into account:– Uncertain supply and demand– Product outdates and wastes– Transit time in rural areasApril 1, 2005Operations Research Models for Wait Lists35
Blood ProductSupply Chain:Conceptual ModelRegionBlood CentreBleed RequestsNon-bleed Requests7/241 hr expiry07-216 hr expirySupplyMon-Sat14-22WasteImports08-24Blood CentreSunnybrookTrauma/ICU7/241 hr expiryToronto StockBleedRequests1 hr expiryOutdatedNon-BleedRequests Cancer6 hr expiry07-211 hr expiryMedicine07-211 hr expirySurgery7/241 hr expiryWasteSunnybrook StockOutdated7 hrdelayDailyPlannedRequestMon-Fri 011 hr expiry
System Dynamics Simulation forCardiac Resource Allocationat Trillium Health CenterSomayeh Sadat, Caroline Chan, Michael CarterApril 1, 2005Operations Research Models for Wait Lists37
Cardiology at TrilliumzzzzCommunity Hospital which also serves asthe regional cardiac care centre forcommunities west of Toronto, OntarioConducts 10% of all cardiac procedures inOntarioPerforms more than 7,000 cardiac surgeriesannuallyPerforms unique procedure: beating heartsurgeryApril 1, 2005Operations Research Models for Wait Lists38
Cardiac Patient Flow at TrilliumED LOSEmergencyDepartmentOther AcuteHospitalsP1 effect ofcardiologistavailability on patienttransfers Heart FunctionClinic Effect of CSPUnurse ratio Effect of CSPU bedsutilization ratio Physician's OfficeED2CSPUCSPUCCUCardiac ORCARU2C or CARU2DCSSUMedicine UnitsCSICUDaySurgeryRehabilitationAlternativeLevel of Care
Mathematical Programming:Strategic HospitalPlanning ModelMid 1990’s – 3 year cuts of 18%z John Blake Ph.D. thesis - Mt. Sinai Hospz Understand relationship between revenues,costs, resources.z Mathematical modelz Goal Programming formulationzApril 1, 2005Operations Research Models for Wait Lists40
Problem Statement Identify a case mix for physicians that:z Enablesthe hospital to break even.z Providesphysicians with a stable income.z Allowsphysicians, as much as is possible,to perform their target mix of cases.April 1, 2005Operations Research Models for Wait Lists41
Two Goal Programming ModelszVolume model:– Fix the cost of each CMG– Determine the case mix that meets targetszCost model:– Fix the case mix (volume) for each CMG (atcurrent levels)– Determine the cost reductions necessary tomeet targetsApril 1, 2005Operations Research Models for Wait Lists42
Project Results Used during 1996 (plan for 11% cut) Intuition at hospital: Retain clinically important services (oncology) Eliminate “unimportant” services (dental, ENT,ophthalmology)Model recommendations: increase dental/eye/ENT decrease thoracic, oncologyThoracic surgery was eliminated in 1997April 1, 2005Operations Research Models for Wait Lists43
Western Canada Wait List ProjectWait lists are anecdotal!z Plus, every doc has his/her own priorityz WCWL has developed standard priorityinstrumentsz But, how will that help reduce wait times?z Need to develop models of resources topredict impact on wait times.zApril 1, 2005Operations Research Models for Wait Lists44
Cardiac Care Network of OntarioCurrently fund 110 surgeries per 100,000pop.z What would happen to wait lists if theyfunded 120? 130?z Developing simulation model with CCNOand ICES (Jack Tu)zApril 1, 2005Operations Research Models for Wait Lists45
Readingsz“Operations Research and Health Care: AHandbook of Methods and ApplicationsSeries”, Kluwer International Series inOperations Research and Management Science,Vol. 70, Brandeau, Margaret L.; Sainfort,Francois; Pierskalla, William P. (Eds.) 2004,872 p.April 1, 2005Operations Research Models for Wait Lists46
Simcoe County CCAC zServices -Nursing -Therapies - Personal Support zMeals, bathing, dressing, cleaning, living skills . - Placement Services z21 Long term care facilities - 1,763 beds. April 1, 2005 Operations Research Models for Wait Lists 19 Simcoe County CCAC zTherapies