Transcription
The Use of the Behavioral Health Data Portal forClinical Outcome Monitoring and ClinicalImplicationsCAPT Meghan Corso, Psy.D., Col Scott Sonnek, Ph.D.,and Adam Rodgers, PMP23 July 20200855 – 0955 (ET)“Medically Ready Force Ready Medical Force”1
PresenterCAPT Meghan L. Corso, Psy.D., ABPPChief, Behavioral Health Clinical Management TeamMedical AffairsClinical Support DivisionDefense Health AgencyDHHQ, Falls Church VA“Medically Ready Force Ready Medical Force”2
CAPT Meghan Corso, Psy.D.CAPT Meghan Corso currently serves as the Chief of Behavioral HealthClinical Operations at the Defense Health Agency. In this role, CAPTCorso is responsible for Department of Defense (DoD)-wide behavioralhealth policies, procedural instructions, and Congressional reports. Sheserves as a DoD representative to several interagency and inter-servicetask forces which address significant national or internationalbehavioral health concerns with the goal of developing and executingsolutions.CAPT Corso graduated from the American School of ProfessionalPsychology at Argosy University in Washington DC in 2006. She alsoearned board certification in Clinical Health Psychology in 2012 fromthe American board of Professional Psychology. CAPT Corso is a HealthServices Officer in the United States Public Health Service (USPHS) since2009. She also honorably served four years as a psychologist in theUnited States Air Force. CAPT Corso has earned an impressive awardhistory including USPHS Meritorious Service Medal; USPHS OutstandingService Medal; USPHS Presidential Unit Citation; USPHS OutstandingUnit Award; and U.S. Navy Commendation Medal among others.“Medically Ready Force Ready Medical Force”3
PresenterCol Scott Sonnek, Ph.D.Chair, Behavioral Health Clinical CommunityMedical AffairsClinical Support DivisionDefense Health AgencyDHHQ, Falls Church VA“Medically Ready Force Ready Medical Force”4
Col Scott Sonnek, Ph.D.Col Sonnek is the Air Force Director of Psychological Health (DPH) at the Air Force MedicalReadiness Agency (AFMRA) in Falls Church, Virginia. The Mental Health Branch at AFMRA isresponsible for subject matter expert inputs and engaging senior leaders at theHeadquarters-Air Force, Department of Defense, and Congressional levels, as well as theexpansion and management of Integrated Operational Support. Col Sonnek represents AirForce Mental Health interests at the Defense Health Agency’s (DHAs) Behavioral HealthClinical Community function, deemed the most advanced of all DHA Clinical Communities.The DPH office also administers the mental health (MH) aspects of “True North”, a multifaceted Headquarters Air Force (HAF) initiative to embed various support elements withinunits at four Air Force installations, expected to expand to 16 total bases in Fiscal Year2021.Col Sonnek completed his Clinical Psychology Residency at Wilford Hall Medical Center,Lackland AFB, TX in 1998 and received his Ph.D. in Clinical Psychology from the University ofWyoming in 1999.Col Sonnek has commanded at flight, detachment, and squadron levels. He has served as aMental Health Flight Commander at four installations and twice as a Major CommandBehavioral Health Consultant. As a faculty member at two psychology internship sites, LtCol Sonnek has helped train and launch a total of 56 Air Force Clinical Psychologists. Hedeployed to Iraq in 2009, led the joint mobile Combat Stress Control team withresponsibility for the southern half of the country, and completed 18 missions to austerelocations. In 2013, Lt Col Sonnek deployed to Bagram Airfield, Afghanistan as the 455thCombat Stress Control Detachment Commander where his team was the theater hub for allpsychiatric aeromedical evacuations and recovered/repatriated personnel during a rapid,vast drawdown of forces.“Medically Ready Force Ready Medical Force”5
Presenter(s)Adam T. Rodgers, PMPProgram Manager, Behavioral Health Data PortalBehavioral Health Clinical Management TeamClinical Support DivisionDefense Health AgencyJoint Base Lewis McChord, WA“Medically Ready Force Ready Medical Force”6
Adam T. Rodgers, PMPAdam Rodgers currently serves as the Program Manager (PM) of theBehavioral Health Data Portal (BHDP) under the Behavioral HealthClinical Management team at the Defense Health Agency. In this role,Adam Rodgers is the principal staff advisor and technical consultant tothe Chief, Behavioral Health Clinical Management Team on programmanagement issues, responsible for providing operational support,analysis, metrics development, performance reporting, resourcemanagement analysis and strategic planning for the Behavioral HealthData Portal application.Adam Rodgers graduated from Mount Saint Mary’s University, MD witha BS in History on an ROTC scholarship and commissioned into the U.S.Army in 2002. He served six years on active duty as both an Armor andSignal officer before transitioning to the Washington Army NationalGuard (12 years) where he is currently the operations officer for anInformation Operations Brigade. As a civilian, Adam has spent the last12 years working in IT project/program management, specificallymilitary Behavioral Health (BH). He split that time working as a PM forthe National Center for Tele-Health and Technology and then theArmy’s BH Service Line / DHA BH Clinical Management Team.“Medically Ready Force Ready Medical Force”7
Disclosures§ CAPT Meghan Corso, Col Scott Sonnek, and Mr. Adam Rodgers haveno relevant financial or non-financial relationships to discloserelating to the content of this activity.§ The views expressed in this presentation are those of thepresenter(s) and do not necessarily reflect the official policy orposition of the Department of Defense, nor the U.S. Government.§ This continuing education activity is managed and accredited by theDefense Health Agency, J-7, Continuing Education Program Office(DHA, J-7, CEPO). DHA, J-7, CEPO and all accrediting organizationsdo not support or endorse any product or service mentioned in thisactivity.§ DHA, J-7, CEPO staff, as well as activity planners and reviewers haveno relevant financial or non-financial interest to disclose.§ Commercial support was not received for this activity.“Medically Ready Force Ready Medical Force”8
Learning ObjectivesAt the conclusion of this activity, participants will be ableto:1. Describe the background and conditions leading to thecreation of the Behavioral Health Data Portal (BHDP).2. Outline what BHDP is to include understanding featuresand functions.3. Comprehend how DHA uses BHDP to analyze behavioralhealth data, track patient progress and outcomes, andmonitor treatment efforts.“Medically Ready Force Ready Medical Force”9
Background§ In 2013, the Assistant Secretary of Defense for HealthAffairs issued a memorandum to provide guidance onthe collection of BH clinical outcomes.§ The memo requires that clinical outcomes, based onspecific validated and standardized measures, bedocumented throughout BH care using BHDP.§ Furthering this mandate, in July 2018 DHA publishedDHA-PI 6490.02, which establishes BHDP as therequired data collection tool in BH specialty care andSubstance Use Disorder (SUD) clinics.“Medically Ready Force Ready Medical Force”10
What is BHDP?§ BHDP is a web-based system used by BH staff to collect, trackand display a patient’s current and/or past BH diagnosis andtreatment planning.§ BHDP provides improved patient tracking within and acrossBH clinics, allows for real-time information regarding ServiceMember's psychological health readiness, and enhances cliniccommunications to ensure optimal, coordinated BH care.§ Metrics established and required by DHA-PI 6490.02 arecollected from BHDP and used by DHA and clinic leadership toanalyze BH data, track patient progress and outcomes, andmonitor treatment efforts.“Medically Ready Force Ready Medical Force”11
BHDP EquipmentProvider Computer / PortalURL: ccess: .mil network onlyPatient Laptop / KioskBHDP Image – No other computer functionalityBHDP Image (Multi or Single Screen) setup by local IMDAccess: .mil network onlyBar Code Scanner Check-In“Medically Ready Force Ready Medical Force”12
Key Functions of the BHDP§ Rapid check-in capability using identification (ID) cardbarcode scans§ Sorting and filtering of provider/clinic patient lists§ Tracking of patient care team members§ Real-time graphing of clinical outcomes and symptompresentation for provider dashboards§ Integration of deployment health assessment data§ Standardized documentation templates integratedwith patient reported data“Medically Ready Force Ready Medical Force”13
Clinic FlowPatient Arrivesin Waiting RoomPatient ChecksInPROVIDERSUPPORT STAFFWithout BHDPPatientAppointmentProvider EntersAHLTA NoteAHLTA- Armed Forces Health Longitudinal Technology Application“Medically Ready Force Ready Medical Force”14
Clinic FlowPROVIDERSUPPORT STAFFWith BHDPPatient Arrivesin WaitingRoomPatient ChecksInProviderReviews BHDPPatient UsesBHDPPatientAppointmentProvider can enterDiagnosis, TreatmentModality, Risk forHarm to Self, Risk forHarm to Others andSelects Follow-upQuestionnaires“Medically Ready Force Ready Medical Force”Provider EntersAHLTA Note15
Terminology§ Sections (e.g., PHQ-9) :Question subsets, usuallyvalidated questionnaires§ Surveys (e.g., AdultPHQ-9Adult BHSurvey:Collection ofSectionsEvaluation or Follow-up) :A collection of Sectionsadministered at one timePHQ- Patient Health Questionnaire; PCL- Post-Traumatic Stress Disorder Checklist; ISI- Insomnia Severity IndexPCL-5ISI16
BHDP Clinical ScalesCLINICAL SCALEDESCRIPTIONBehavior and Symptom IdentificationScale(BASIS)-24General DistressWalter Reed Army Institute of Research (WRAIR)Functional Impairment4QPTSD - PCL-5Post-Traumatic Stress Disorder (PTSD)PHQ2 - PHQ9DepressionGeneralized Anxiety Disorder GAD2 - GAD7AnxietyAlcohol Use Disorders Identification Test AUDIT-C- AUDITAlcohol UseColumbia-Suicide Severity Rating Scale (C-SSRS)Suicidal Ideation (0-5)Couples Satisfaction Index (CSI)Couples SatisfactionISI (Optional)Insomnia Severity IndexBrief Addictions Monitor-BAM (Optional)Addictions17
BHDP Survey Timing1. Initial Adult Evaluation (15-20 min.): New Patients: Arrive 30 minutes prior to first session tocomplete the BHDP Established Patients: Providers prepare patient for BHDP2. Follow-up Survey(s) (5-10 min.): Patients arrive 15 minutes prior to each follow-up session18
Survey “Skip Logic”§ Skip Logic or Gating Questions: Patient’s response determines whetheradditional sections and/or questions are asked.EXAMPLEIf patient responds positively to having a spouse or significant other, theCouple’s Satisfaction Index (CSI) is administered. If not, CSI is skipped.CSIYESAre youmarried?NONextQuestionnaire19
Provider Portal / Patient List“Medically Ready Force Ready Medical Force”20
Patient Check-In“Medically Ready Force Ready Medical Force”21
Patient Portal000111112SE1980“Medically Ready Force Ready Medical Force”22
Patient Portal“Medically Ready Force Ready Medical Force”23
Provider Dashboard“Medically Ready Force Ready Medical Force”24
Provider’s Treatment Status IslandTreatment Status Island gives the provider a quick look at the major treatment components:Main diagnostic focus of BH treatmentOnly select additional diagnosis if it is a focus oftreatmentChoices also include closed case optionsChoices based on DoD/VA Suicide CPG.“Medically Ready Force Ready Medical Force”25
Automated Section FrequencyWhen a Diagnosis (Army and Air Force-AF) is selected, the appropriate outcome measure is scheduled for7 or 14 day frequency. If provider would like measure administered more frequently, provider can useclinical discretion to do soDiagnosisPTSDTherapyProlonged ExposurePTSDCognitive Processing TherapyPTSDEMDRPTSDOther therapiesMajor Depressive DisorderAll TherapiesAdjustment DisorderAll therapiesBipolar DisorderAll therapiesPanic DisorderAll therapiesGeneralized Anxiety DisorderOther Anxiety DisorderSleep DisorderRelationship ProblemAll therapiesAll therapiesAll therapiesAll therapiesSectionPCL-5Current 14d14d14d14dGAD7GAD7ISICSI14d14d14d14dEMDR- Eye Movement Desensitization and Reprocessing“Medically Ready Force Ready Medical Force”26
Lifetime Suicide Risk Level§ This information displays patientself-report regarding lifetimehistory of suicide risk level.§ Date of original lifetime risk levelassessment will always bedisplayed.“Medically Ready Force Ready Medical Force”27
Acute Suicide Risk Level§ Date the last screening was completedby patient will be displayed§ Current risk assessment given at everyfollow-up visit§ Information will display if completed inthe last 30 days§ Harm to others: Displays whencompleted in the last 7 days.§ Access to Weapons: Response willalways display.§ Color codes respond to yes/no“Medically Ready Force Ready Medical Force”28
BHDP Output – Notes ViewSelect “Note Text” tocopy/paste into EHRData formatted as anarrative to serve as anote that may be copiedinto EHRElectronic Health Record (EHR)“Medically Ready Force Ready Medical Force”29
BHDP Metrics§ Primary source of Tri-Service standardized outcomes data used to measure BH treatmentefficacy for all behavioral health programs throughout DHA.§ DHA developed treatment outcome metrics for posttraumatic stress disorder (PTSD), anddepression disorders using BHDP data. These measures of treatment effectiveness show therate at which patients with these disorders have a significant reduction or remission ofsymptoms. Military medical treatment facilities (MTFs) are responsible for these outcomemetrics, improving treatment effectiveness for these key BH conditions.§ MTFs, clinics, providers and researchers, and others continue to request de-identified datafor operational purposes, Quality Improvement (QI) projects, program evaluations,responses to Joint Commission findings, journal articles, conference presentations, etc.§ With the increased prevalence of BHDP data, DHA is at the forefront of outcomes basedresearch and metrics development nationally.“Medically Ready Force Ready Medical Force”30
Surveys CompletedNumber of Completed Surveys by Survey TypeAll Branches / All SurveyTypesAF Adult BHArmy Adult BHNavy Adult BHAdolescentFamily Advocacy Program(FAP)Internal Behavioral HealthConsultant (IBHC)Primary Care BehavioralHealth (PCBH)Substance UseTraumatic Brain Injury 07,1292,907Feb-2016,00146,3116,4422,567Total(Jul 19 – Feb 1734147,68144,6153,321All Time Surveys Completed 6,154,866“Medically Ready Force Ready Medical Force”743,29031
BHDP MetricsAvailable MetricsCentral repository of all DHA Behavioral Health Metrics“Medically Ready Force Ready Medical Force”32
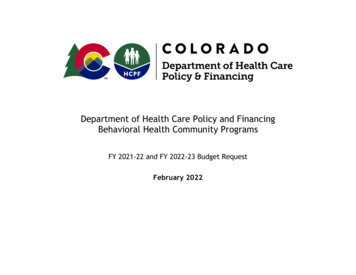
Positive Outcomes Over Time - MDDMajor Depressive Disorder (MDD) – Positive Outcomes Over TimeTARGET 47%“Medically Ready Force Ready Medical Force”33
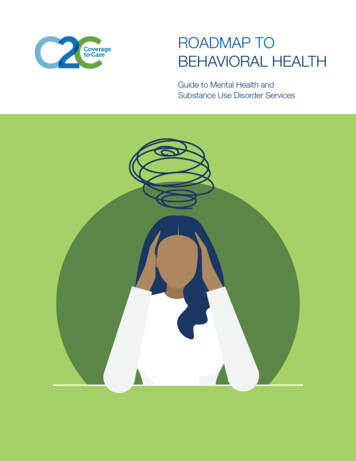
Positive Outcomes Over Time - PTSDPTSD – Positive Outcomes Over TimeTARGET 36%“Medically Ready Force Ready Medical Force”34
Evidence Based TreatmentEvidence Based Treatments Best Practices / preferred approaches for behavioral health symptom treatment# of Patients# of Patients w/ EBTEBT Utilization Rate23,90921,56090.18%TARGET 80%EBT Utilization Rate: Displays how many patients with a primary or secondarydiagnosis of PTSD, MDD, or SUD have a listed treatment modality that is an EBTthat is appropriate for the diagnosis.“Medically Ready Force Ready Medical Force”35
Therapeutic Alliance and PatientSatisfactionRelationship between the patient and provider. Essential aspect of successful therapy anddriver for positive patient outcomesPercentage of cases with a Therapeutic Alliance Score Greater then 2468.4%Percentage of patients satisfied with the ability to get an appointment with theirBH provider80.6%Percentage of patients satisfied with the friendliness, respectfulness andhelpfulness of the non-provider BH support staff within the BH clinic87.8%Percentage of patients that said their Command gave them a hard time aboutcoming to BH (Active Duty only)5.85%“Medically Ready Force Ready Medical Force”36
Key Takeaways By DoD memorandum and DHA instruction, specialty care andSUD clinics are required to use BHDP to track patient outcomes. Collecting patient data at the point of care gives clinicians andpatients a tool to discuss treatment progress and inform ongoingtreatment planning. Without consistent and comprehensive use of BHDP, MentalHealth Services (MHS) is unable to reliably monitor BHoutcomes.“Medically Ready Force Ready Medical Force”37
ReferencesAssistant Secretary of Defense for Health Affairs Memorandum, “Military Treatment Facility Mental HealthClinical Outcomes Guidance,” September 9, images/docs/OASDmemo dtd09sep13.pdfCorso, K.A., Bryan, C.J., Corso, M.L., Kanzler, K.E., Houghton, D.C., Ray-Sannerud, B., & Morrow, C.E. (2012).Therapeutic alliance and treatment outcome in the primary care behavioral health model. Families,Systems, and Health, 30(2), 87-100. https://doi.org/10.1037/a0028632Defense Health Agency Procedural Instruction 6490.02, “Behavioral Health Treatment and OutcomesMonitoring,” July 12, 2018.Flückiger, C., Del Re, A.C., Wampold, B.E., & Horvath, A.O. (2018). The Alliance in Adult Psychotherapy: A MetaAnalytic Synthesis. Psychotherapy, 55(4), 316-340. http://dx.doi.org/10.1037/pst0000172“Medically Ready Force Ready Medical Force”38
References, cont.Lambert, M.J., & Barley, D.E. (2001). Research summary on the therapeutic relationship and psychotherapyoutcome. Psychotherapy, 38(4), 357-361. , J.B., Owen, J., Valentine, J.C., Winkeljohn-Black, S., Halford, T.C., Parazak, S.E., Budge, S., & Hilsenroth,M. (2018). Therapeutic alliance, empathy, and genuineness in individual adult psychotherapy: A metaanalytic review. Psychotherapy Research, 28(4), 023Operations Order 18-02, “Behavioral Health Data Portal Implementation) – USAMEDCOM,” October 10, 2017.Operations Order 12-47, “Behavioral Health Data Portal Implementation,“ August 30, 2012.Stubbe, D.E. (2018). The Therapeutic Alliance: The Fundamental Element of Psychotherapy. Focus 16(4), 402403. cally Ready Force Ready Medical Force”39
How to Obtain CE/CME CreditTo receive CE/CME credit, you must register by 0745 ET on 24 July 2020 to qualify for the receipt of CE/CMEcredit or certificate of attendance. You must complete the program posttest and evaluation before collectingyour certificate. The posttest and evaluation will be available through 6 August 2020 at 2359 ET. Pleasecomplete the following steps to obtain CE/CME credit:1. Go to URL: ng-practices-jul-20202.3.4.5.6.Click on the REGISTER/TAKE COURSE tab.a.If you have previously used the CEPO CMS, click login.b.If you have not previously used the CEPO CMS click register to create a new account.Follow the onscreen prompts to complete the post-activity assessments:a.Read the Accreditation Statementb.Complete the Evaluationc.Take the PosttestAfter completing the posttest at 80% or above, your certificate will be available for print or download.You can return to the site at any time in the future to print your certificate and transcripts athttps://www.dhaj7-cepo.com/If you require further support, please contact us at ly Ready Force Ready Medical Force”40
presentation for provider dashboards §Integration of deployment health assessment data §Standardized documentation templates integrated with patient reported data. . Brief Addictions Monitor-BAM (Optional) Addictions 17. BHDP Survey Timing 1. Initial Adult Evaluation (15-20 min.):