Transcription
Vol. 11, No.1 - Jan. - June 2008J. Baqai Med. Univ.REVIEW ARTICLEREHABILITATION OF PARAPLEGIAFarhan Ishaque l , Mahwish Shamim2ABSTRACT:The term Paraplegia is used to define the loss of ability to move or feel both legs and lower trunk. Paraplegiais usually caused by an injury to the spinal cord at the level of thoracic, lumbar or sacral region, whichsequentially results in a loss or damaged function. Injuries resulting from a motor vehicle accident, gunshotand during sports activities may result in paraplegia. Non-traumatic factors like scoliosis, spinal tumors andspina bifida can also cause paraplegia. Paraplegic patients have an extensive stage of rehabilitation ahead.Most important goals for paraplegic rehabilitation are to increase strength, improve flexibility, increase enduranceor aerobic conditioning, gait training, transfer training and improve body positioning .KeyWords:Functional Electrical Stimulation [FES] , Gait Training, SCIINTRODUCTIONParaplegia is a term used to explain a condition for aperson who has been paralysed due to a spinal cordinjury. Paraplegia is a Greek word (Para for "two"and Plegia meaning paralysis). It involves loss ofmovement and sensation in the distal half of the body(right and left legs)l . It usually takes place as a resultof spinal cord injuries at Tl or below i.e. injury in thethoracic, lumbar or sacral regionl ,ll . The spinal cordis a cluster of nerves that transmits messages betweenthe brain and the rest of the body2.Kind of SCI Lesions:It is significant to note that the spinal.cord does nothave to be completely cut off for the loss of functionlO,12. ?70% incomplete lesions, 30% complete lesions 5 . ?60% paraplegic lesions, 40% tetraplegic lesions. ? A complete injury indicates that there is nofunction below the level of the injury; n() Il !i()!!and no controlled movement. Both sides of thebody are evenly affected. ? An incomplete injury indicates that there is somefunctioning below the level of the injury. A personwith an incomplete injury may be able to moveone limb more than another, may be able to feelbody parts that cannot be moved, or may havemore functioning on one side of the body thanthe other. ?Such injuries are known as Brown SequardSyndrome, Central Cord Syndrome, Anterior CordSyndrome and Posterior Cord Syndrome 1,12.A patient of paraplegia at B aqai Medical University, Hospital1: Senior Lecture r (BIPTRM), 2: Assistant Professor, Baqai Institute of Physical Therapy and Rehabilitation Medicine, Baqai Medical University, Karachi .
Vol. 11, No.1 - Jan. - June 2008J. 8aqai Med. Univ.Diagram showing Level of the InjuryA spinal cordinjury abovethis line wouldresult inquadraplegia Physical TherapistOccupational TherapistPsychologist/PsychiatristOrthotistSocial WorkerDieticianThe goals determined for each individual will varyaccording to the level of injuries. Every injury isonly one of its kind and two injuries categorised asthe identical level will not always show the samedeficit8 ,11.Posterior(Rear)Anterior(Front)PHYSICAL THERAPY:ooFollowing are the Common features of Paraplegia:- - Loss of movement, sensation, and reflexes belowthe level of the spinal cord injury immediatelyafter the spinal cord injury.- - Muscle weakness or paralysis in the legs, trunk orarms.- - Failure of Bowel and Bladder control, dependingon where the spinal cord injury occurred.- - Sexual variations- - Muscle spasticity.- - Gastrointestinal problems.oooREHABILITATION:Rehabilitation is the (re)integration of an individualwith a disability into society. This can be done eitherby enhancing existing capabilities or by providingalternative means . " (Robinson 1993)[05]Basically rehabilitation is dependent relatively on thelevel and type of spinal cord damage.THE REHABILITATION TEAM:The rehabilitation team facilitates to set short termand long term treatment goals for recovery. Skilledand expert professionals are part of the ParaplegicRehabilitation team, inclu?ing 11 : Physiatrist N eurologist/Neurosurgeon Orthopaedic surgeonoooPhysical therapy is the most important part of thetreatment program in rehabilitation centers.Physical therapy seeks to bring back or upholdthe ability to move.Physical therapy generally focus on reducingmuscle tone, maintaining or improving range ofmotion and mobility, increasing strength andcoordination and improving comfort. 3Physical therapy exercises help in maintainingbone density, as the paraplegic patients are moreprone to develop osteoporosis in the lower limbsespecially in the region of the hip14.Physical therapy programs may also incorporatetreatments designed to prevent certaincomplications such as frozen joints, contracturesor bedsores.Therapies may include stretching, strengthening,aerobic exercises, gait training and appropriateuse of assistive devices, such as canes, braces,walkers etc.Balance and coordination activities; transfertraining - such as how to get from bed to wheelchairor from wheelchair to car.Postural changes are also one of the big issueswhich might result in bed sores and need posturalre-education8 .Therapeutic techniques can also include such ashydrotherapy, ultrasound therapy, electricalstimulation which help in stimulation of expiratorymuscles and increasing the cross-sectional area oflarge arteries and enhance blood circulation to theparalyzed legs of individuals with SCI. 22Balanced Exercise Program:A balanced exercise program includes three types ofexerCise:
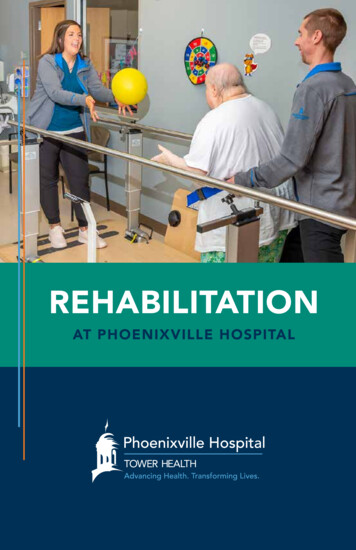
Vol. 11, No.1 - Jan. - June 2008J. Baqai Mec'J. Univ.Stretching Exercises:o Stretching is one of the most important exercisesand must be done on a regular basis, usually twicea day. That is because stretching improves theability of muscles to move the parts of bodythrough their full range of motion and releasecontracture27 . Stretching also reduce muscle spasmsand Spasticity.oEvery stretch should be performed slowly andgradually for 10 seconds. Some of the importantstretching exercises for paraplegics are as follows:Bilateral Adductors StretchingQuadriceps Stretching
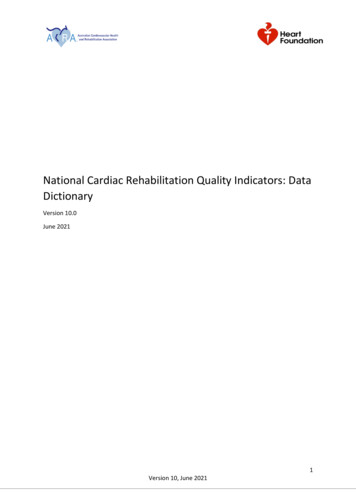
Vol. 11, No.1 - Jan. - June 2008Aerobic Exercises:Aerobic exercise helps to enhance energy levels, reducefatigue, and control body weight. It also fortifies heartand lungs and improves body's ability to use oxygen.Early rehabilitation enhances the cardiac efficiencyI9,9.Exercise training is important for the Paraplegics inthe same way as the non-handicapped individuals.Both strength (ability to develop tension) andendurance (aerobic capacity as measured by V02max) contribute to overall functional capacity.Moreover expiratory muscle training exercise help inimproving inspiratory muscle function 20 . Activeexercise gives a positive stimulus to the cardiorespiratory system. A combine contraction of upperextremity and of paralysed lower extremity musclesresults in activation of more muscle groups7.Strengthening Exercises:Strengthening exercises help in increasing muscle toneand improve the potency of muscles 17 . Resistance andendurance training enhances mobility and provides apositive sense of well-being29. Strong hip and legmuscles are needed to lift the legs to walk and strongarm muscles are needed to carry out ADLs, especiallylatissimus dorsi muscle needs to be strengthenadequately to perform the pulling and pushingactivities. Strong abdominal and back muscles helpJ. 8aqai Med. Univ.to maintain correct posture and can respond to thepain resulting from poor gait, poor posture or the useof mobility aids. Patients with spinal cord injury areable to stimulate their trunk muscles, even the musclesbelow the level of injury2. Therefore physical therapistmust concentrate on the · strengthening of trunkmusculature, which plays a crucial role in gait training.GAIT TRAINING OF A PARAPLEGICPATIENT:Walking or Gait training is the ultimate goal of aparaplegic patient. Along with strengthening andbalance exercises, physiotherapists and orthotistsrecommend certain orthosis, by the help of which apatient can perform their functional tasks not only instanding but also in walking I8 ,19. Most commonly kneeankle foot orthosis with pelvic belt (KAFO) is preferred.A swing through type of gait pattern is accomplishedwith KAFO along with elbow crutches 1. Walking isrecommended according to the ability, endurance andsafety of the patient.Trademil training also helpful ingait training of paraplegics23 . Such training programscan improve the ability of patients with incompleteparaplegia to walk on stationary surfaces. Trademiltraining improve the mobility of patients withparaplegia4 ,) 6.Gait Training, Wearing KAFOBaqai Institute of Physical Therapy and Rehabilitation Medicine
Vol. 11, No.1 - Jan. - June 2008J. 8aqai Med. Univ.Hydrotherapy: Swimming is one of the most favourable exerciseforms. Water reduces the effects of gravity, allowingweakened limbs to attain a greater range of motion.Water also helps the body so there is less stress onhips, knees, and spine. Exercises in the water can help increase musclepower and endurance and help mobilize jointsand muscles. They also help to relax muscles andimprove coordination.ASSISTIVE DEVICES:Assistive devices improve gait pattern, balance andcoordination by providing additional support andstability, and help in reduce exertion [05] .Canes:The standard cane (stick) has single shaft, with anarched top. Canes help in supporting up to 25% ofbody weight. The quad cane is a one-armed cane withfour legs and it is more stable than standard canes forstability point of view. A physical therapist or anorthotist recommend an appropriate cane and giveinstructions about handling.Wheelchair:Wheelchairs help in general functional activities ofdaily living. Paraplegics can improve their cardiovascular efficiency by wheel chair training 6.Orthosis:Orthosis are artificial devices with special splints orbraces used for gait training. There are a variety oforthosis, but for paraplegic patient a knee ankle footorthosis (KAFO) is widely recommended. They alsohelp in walking re-education of paraplegics when usedwith functional electrical stimulation 18,21 . Orthosishelp in increasing balance or remove pressure fromstressful areas of the body but on the other hand itcosts high energy for paraplegic patients. Many deviceshave been developed to improve this problem of energyexpenditure like weight-bearing control (WBC)orthosis 24 . WBC orthosis is designed to fulfil threemost important needs; a rigid frame that holds up thepatient's body weight, a special hip joint device thatreciprocally pushes each leg forward, a gas poweredfoot device that varies the sole thickness of the devicefor foot/ floor clearance, and control system of theorthosis 25 , consequently decreasing the energyexpenditure.Patient Wearing Knee Ankle Foot Orthosis Instituteof Physical Therapy and Rehabilitation Medicine(Baqai Medical University Hospital)Walker:A standard walker consists of four adjustable legs andcan support up to 50% of body weight. Walking witha walker needs sufficient upper-arm strength. Thereforestrength training and passive mobility for upperextremity is mandatory2o. The length of the walkershould be changeable so that the handgrips, can beadjusted with Hip joint. This will help patient to getgood standing posture and to walk in the proper gaitcycle with the walker. FES also plays a vital role inre-education of standing posture and useful in retainingthe physiological state of musc1es 21,26. In fact functionalelectrical stimulations (FES) are electrical stimulationof muscles in order to recover the damaged motorfunction by stimulating skeletal muscles 28 .CONCLUSION:Rehabilitation of paraplegia is a multidisciplinaryapproach and this review will help in providing anoutline about the rehabilitation of paraplegic patientsand hopefully provide some direction not only forfurther research but also recommendations forpractitioners working in the field of rehabilitation.
Vol. 11, No.1 - Jan. - June 2008REFERENCES:1. Susan. B. Osullivan, Thomas. J. Schmitz, PhysicalRehabilition, 4th edition. F. A Davis company,Philadelphia.2. Bjerkefors A, Carpenter MG, Creswell AG, Trunkmuscle activation in a person with clinicallycomplete thoracic spinal cord injury. Journal ofRehabilitation Medicine, 2009 Apr; 41(5): 390-2.3. Phil Klebine, exercisc after SCI, Pushin' OnNewsletter, Vol. 21 [1], Winter, 2003 . 4. F Felicil,a, M Bernardi\ A Rodiol, P Marchettoni\Rehabilitation of walking for paraplegic patientsby means of a treadmill, V Castellano 2 and AMacaluso l June 1997, Volume 35, Number 6,Pages 383-385.J . 8aqai Med. Univ.12. A. Bosh et al. incomplete traumatic quadriplegia:A ten year review. JAMA. Vol. 216, 1971 , 473478.13. Cowell LL, Squires WG, Raven PB. Benefits ofaerobic exercise for · the paraplegic, PMID:3534507.14. Vlychou M ., Papadaki P.J, Zavras G.M.; MalizosKN; Fezoulidis I.B. paraplegia-related alterationsof bone density in forearm and hip in Greekpatients after spinal cord injury, Rehabilitation,Vol. 25, Number 7, April 08,2003, pp. 324-330(7).15. H L Gerrits, A de Haan, A J Sargeant, H vanLangen, M T Hopman. Peripheral vascularchanges after electrically stimulated cycle trainingin people with spinal cord injury. Spinal Cord.2001 Mar; 39 (3): 156-60, 11326326.5. Prof. Dr.-Ing. Robert Riener. Neurorehabilitation,ETH Zurich & Spinal Cord Injury Center,University Clinic Balgrist, Zurich, June 2nd, 2008.16. V Dietz, M. Wirz, Jensen Locomotion PediatrClin North Am. 1996 Oct; 43 (5):1135-508858076. Cooper RA, Horvath SM, Bedi JF, DrechslerParks DM, Williams RE , Maximal exerciseresponse of paraplegic wheelchair road racersParaplegia. 1992 Aug ; 30 (8): 573-8117. M Ellenberg, M MacRitchie, B Franklin, SJohnson, D Wrisley, Aerobic capacity in earlyparaplegia: implications for rehabilitation Journal:0110911989 ; 27(4) : 261-8 . ISSN: 0031-1758.7. Michael Kjaer, Why exercise in paraplegia. BritishJournal of Sports Med. 2000; 34: 322-3230818. Stauffer Y, Allemand Y, Bouri M , Fournier J,Clavel R, Metrailler P, Brodard R, Raynard F, TheWalkTrainer-- a new generation of walking reeducation device combining orthoses and musclestimulation IEEE trans neural cyst rehabilitationeng. 2009 Feb; 17(1): 38-458. .Gayle Benson, Postural Changes After SpinalCord Injuries, Pt Pushin'On Newsletter, Vol. 17. [2], 1999.9. P. J. Pacy; R. H. Evans ; D. Halliday, Effect ofanaerobic and aerobic exercise promoted bycomputer regulated functional electricalstimulation(FES) on muscle size strength andhistology in paraplegic males, Prosthetics andOrthotics International, 17461553, Vol. 11, Issue2, 1987, Pages 75-79.10. Spinal cord injury, from Wikipedia, the freeencyclopaedia, last modified, 19 December 200611 . Medical content last reviewed, Physical medicineand Rehabilitation, Spinal cord injuries, November,2001.e:19. Tordi N, Mourot L, Chapuis A, Parrate B, RegnardJ, Effects of a primary rehabilitation programmeon arterial vascular adaptations in an individualwith paraplegia. Annals of Physical RehabilitationMedicine. 2009 Feb; 52(1): 66-73.20. Eriks-Hoogland IE, de Groot S, Post MW, vander Woude LHJ, Passive shoulder range of motionimpairment in spinal cord injury during and oneyear after rehabilitation. Journal of RehabilitationMedicine, official journal of UEMS. 2009 May;41(6): 438-4421. Pages G, Ramdani N, Fraise P, Guiraud D, Amethod for paraplegicupper-body posture
Vol. 11, No.1 - Jan. - June 2008estimation during standing: a pilot study forrehabilitation purposes. Medical and BiologicalEng Comput. 2009 Jun; 47(6): 625-33.22. Schilero GJ, Spungen AM, Bauman WA,Radulovic M, Lesser M. Pulmonary function andspinal cord injury. Respiration PhysiologyNeurobiology. 2009 May 15; 166(3): 129-41.23. Moreh E, Meiner Z, Neeb M, Hiller N, SchwartzI, Spinal decompression sickness presenting aspartial Brown-Sequard syndrome and treated withrobotic-assisted body-weight support treadmilltraining. Journal of Rehabilitation Medicine. 2009Jan; 4.24. N Kawashima, Y Sone2 , K Nakazawa 1, M Akai 1and H Yano, Energy expenditure during walkingwith weight-bearing control (WBC) orthosis inthoracic level of paraplegic patients. Spinal Cord(2003) 41, 506-51 doi:1O.1038/sj.sc.310149425. Yano H, Kaneko S, Nakazawa K, Yamamoto SI,Bettoh A, A new concept of dynamic orthosis forparaplegia: the weight bearing control (WBC)J. 8aqai Med. Univ.orthosis Prostheric and Orthotics InternationalJournal, 1997 Dec; 21(3): 222-8.26. Mandl T, Meyerspeer M, Reichel M, Kern H,Hofer C, Mayr W, Moser E, Functional electricalstimulation of long-term denervated, degeneratedhuman skeletal muscle: estimating activation usingT2-parameter magnetic resonance imagingmethods. Journal artificial Organs. 2008 Aug;32(8): 604-8.27. Dr Lisa Harvey*, Robert Herbert, Jack CrosbieDoes stretching induce lasting increases in jointROM? A systematic review. PhysiotherapyResearch International. Vol. 7, Issue:1, Pg. 1-13,29 Mar. 2006.28. Sujith OK, Functional electrical stimulation inneurological disorders. Europeon Journal ofNeurology. 2008 May; 15(5): 437-44.29. Jacobs PL, Effects of resistance and endurancetraining in persons with paraplegia. JournalMedical and Science in Sports and Exercise, 2009May; 41(5):992-7
Physical therapy seeks to bring back or uphold the ability to move. o Physical therapy generally focus on reducing muscle tone, maintaining or improving range of motion and mobility, increasing strength and coordination and improving comfort. 3 o Physical therapy exercises help in maintaining bone density, as the paraplegic patients are more