Transcription
American Thoracic Society International ConferenceEDUCATIONInnovations inFellowship Education2017 Highlights BookMay 19-May 24, 2017Washington, DCconference.thoracic.org
2017 INNOVATIONS IN FELLOWSHIP EDUCATIONHIGHLIGHTSTABLE OF CONTENTSInstitutionAbstract TitlePageThe following five programs were selected by the ATS Training Committee as the standout programs in educationalexcellence this year. The University of Washington submitted the top Innovations abstract for 2017. University of WashingtonLeadership Education for Critical Care Fellows Using Simulation4Boston UniversityAn Interactive, Flipped-Classroom Approach to Introducing Pulmonary Fellows toFlexible Bronchoscopy6Mount Sinai St. Luke’s-WestICAHN School of MedicinePromoting Humanism in Pulmonary & Critical Care Medicine: For Fellows,By Fellows7Oregon Health and SciencesUniversityUsing High Fidelity Simulation-based Education to Improve PractitionerCompetence and Comfort in Ventilator Management8The Medical University of SouthCarolinaA Longitudinal Curriculum in Critical Care Ultrasonography Training for Pulmonaryand Critical Care Medicine Fellowships9The ATS would like to showcase the additional institutions who submitted an abstractto the 2017 Innovations in Fellowship Education programInstitutionAbstract TitleEastern Virginia Medical SchoolImplementation of a Multifaceted Faculty Development Program11Mount Sinai St. Luke’s-WestICAHN School of MedicineTeaching Skills of Quality Improvement in a Pulmonary & Critical Care Fellowship:A Team Project in the Ambulatory Setting12Mount Sinai St. Luke’s-WestICAHN School of MedicineAn Innovative, Longitudinal, Simulation-Based Medical Education Curriculum forPulmonary and Critical Care Fellows13Mayo ClinicAn Innovative Continuity Clinic Pilot Study Featuring the ‘Fellow of the Day’14Mount Sinai Beth IsraelA Mastery-Learning Model for Longitudinal Critical Care Ultrasound TrainingUsing an Online Archiving and Feedback System16New York University Schoolof MedicineA Novel Blended Learning Course on Ultrasound for Rapid Assessment ofAcute Respiratory Failure18Northwestern University FeinbergSchool of MedicineImplementation of an Integrated Research and Clinical Conference atan Academic Pulmonary and Critical Care Medicine Program20Perelman School of Medicine atthe University of PennsylvaniaLongitudinal Career Development Curriculum for Pulmonary-CriticalCare Fellows21Rush University Medical CenterDevelopment, Implementation, and Maintenance of a Comprehensive PalliativeCare Curriculum for Pulmonary and Critical Care Fellows23University of Kansas MedicalCenter; University of Colorado;University of Wisconsin; Universityof Iowa; University of New Mexico;Rush UniversityMulti-Institution Cooperative Ultrasound Program for Midwest CriticalCare Fellowships25ATS 2017 International ConferencePage1
2017 INNOVATIONS IN FELLOWSHIP EDUCATIONHIGHLIGHTSUniversity of TorontoThe “Ghost Review” Project: Self-regulated Professional Development Activity toImprove Peer Review Skills Amongst Early Career Researchers26Winthrop HospitalImprovement in Chest Radiograph Interpretation Through the Development of aFormal Curriculum27ATS would like to showcase the following three institutions who submitted an updated abstract.The University of Arizona submitted the Top Update for 2017InstitutionAbstract Title University of ArizonaAdvanced Airway Management in Critical Care Fellowship Training: CurriculumAdjustment Aimed at Improving Patient Outcomes29Baylor College of MedicineFive Year Evaluation of an Interactive Respiratory Therapy Curriculum in PediatricPulmonology Fellowship Training30Children’s Mercy HospitalAn Innovative Tool for Fellow Education and Recruitment322PageATS 2017 International Conference
HIGHLIGHTS2017 INNOVATIONS IN FELLOWSHIP EDUCATIONPROGRAM DETAILSThe American Thoracic Society greatly valuesa strong fellowship program as a means ofacademic and clinical success. In an effort torecognize programs that implement exceptionalpractices, the ATS Training Committee developedthe Innovations in Fellowship Education AwardProgram. All pulmonary, critical care, sleep, andallergy fellowship programs (adult and pediatric)were invited to submit one abstract showcasinga novel and innovative best practice method.Abstracts were reviewed and ranked by the ATSTraining Committee based on the following criteria:1. Innovation: How unique is the educationalprogram? What is new and different?2. Implementation / Sustainability: How wasthe program implemented and how effectivewas such implementation? Was this programsustainable over time?3. Transferability: How easily might thiseducational program be adopted by otherprograms?4. Outcomes: Are there reported outcomesor plans to measure them? The goal of thisprogram is to honor fellowship programs thatdemonstrate educational excellence and sharethese best practices with other programs.All abstracts that were received arepublished within this booklet. The ATSTraining Committee would like to thankall the programs that submitted abstractsand applauds them for their innovative andoutstanding work!The committee is pleased to honor the following top programs:University of WashingtonOregon Health and Sciences UniversityLeadership Education for Critical Care Fellows UsingSimulationUsing High Fidelity Simulation-based Education to ImprovePractitioner Competence and Comfort in VentilatorManagementBoston UniversityAn Interactive, Flipped-Classroom Approach to IntroducingPulmonary Fellows to Flexible BronchoscopyMount Sinai St. Luke’s-West-ICAHNSchool of MedicineThe Medical University of South CarolinaA Longitudinal Curriculum in Critical Care UltrasonographyTraining for Pulmonary and Critical Care MedicineFellowshipsPromoting Humanism in Pulmonary & Critical CareMedicine: For Fellows, By FellowsATS 2017 International Conference3
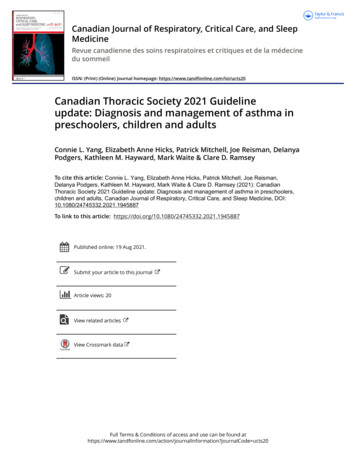
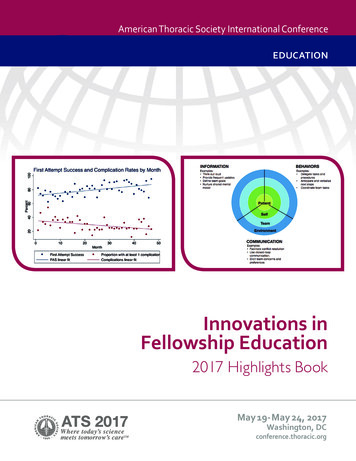
HIGHLIGHTS2017 INNOVATIONS IN FELLOWSHIP EDUCATIONTOP ABSTRACT OF 2017! CONGRATS!University of WashingtonSeattle, WALeadership Education for Critical Care Fellows Using SimulationAbstract Authors: Trevor C. Steinbach MD; Rosemary Adamson MB BS; David Carlbom MD; Nicholas J. Johnson, MD;Patricia A. Kritek MD, EdM; and Başak Çoruh, MDProgram Director: Mark Tonelli, MDType of Program: Pulmonary/Critical CareBACKGROUNDLeadership skills are essential for critical carephysicians. Most fellowship programs do not includefocused education about leadership. Furthermore,there is no commonly employed framework forleadership training within pulmonary and critical caremedicine. In order to address this gap in currenttraining, a formal curriculum aimed at teachingleadership skills to critical care medicine fellows wasdeveloped using a novel framework. High-fidelitysimulation was employed as a means to practiceand solidify newly learned leadership techniques andbehaviors.METHODSCommonly identified leadership skills and behaviorswere extracted from a review of the literature andused to develop a Crisis Leadership Framework (Fig.1). This framework was used to teach leadershipskills to first-year critical care fellows at a singleinstitution. These skills were then assessed usinghigh-fidelity simulation of low-frequency, highrisk critical care scenarios, with fellows leadingmultidisciplinary teams consisting of physicians,nurses, and respiratory therapists. Each scenarioconcluded with a clinical debrief led by the fellow.Immediate feedback on leadership behaviors wasprovided by the non-participating fellows, facilitatedby a faculty member, using the Crisis LeadershipFramework. Leadership skills were formallyassessed by course faculty using the Non-TechnicalSkills for Surgeons (NOTSS) assessment tool (Fig.2). Participants were also surveyed regarding theirperceptions of the utility of the training and theirleadership skills.4RESULTSAfter the first simulation session, all participatingfellows (N 11) agreed that they better understoodkey concepts of leadership (45% strongly agree,55% somewhat agree) and all reported feeling betterprepared to lead a team during crisis (45% stronglyagree, 55% somewhat agree). Ninety-one percentof fellows felt comfortable leading a clinical debrieffollowing the session (36% strongly agree, 55%somewhat agree). NOTSS ratings improved in alldomains (scale 1-4) between the first and secondsimulation session: the situational awareness meanscore increased from 2.5 to 3.3, communication andteamwork from 2.0 to 3.3, leadership from 2.0 to 3.0,and decision-making from 2 to 2.3.DISCUSSIONImplementation of a leadership curriculum withincritical care fellowship training is both feasible andwell-received by trainees. Focused development ofleadership skills using simulation enhanced fellows’perceived leadership knowledge and preparationas well as their adoption of leadership behaviors.Further studies are needed to see if exposure to thiscurriculum translates to improved leadership skillsand team performance during real-life emergencies.ATS 2017 International Conference
HIGHLIGHTS2017 INNOVATIONS IN FELLOWSHIP EDUCATIONFIGURE 1FIGURE 2ICU EMERGENCIES NOTSS CHECKLISTSimulation dateObserverSimulation SELEMENTELEMENT RATING*FEEDBACK ON PERFORMANCEAND DEBRIEFING NOTESGATHERING INFORMATIONUNDERSTANDING INFORMATIONPROJECTING AND ANTICIPATINGFUTURE STATEDECISION MAKINGCONSIDERING OPTIONSSELECTING AND COMMUNICATINGOPTIONIMPLEMENTING AND REVIEWINGDECISIONSCOMMUNICATIONAND TEAMWORKEXCHANGING INFORMATIONESTABLISHING A SHAREDUNDERSTANDINGCOORDINATING TEAM ACTIVITIESLEADERSHIPSETTING AND MAINTAININGSTANDARDSSUPPORTING OTHERSCOPING WITH PRESSURERating*1 PoorPerformance endangered or potentially endangered patient safety, serious remediation is required2 MarginalPerformance indicates cause for concern, considerable improvement is needed3 Acceptable Performance was of a satisfactory standard but could be improved4 GoodPerformance was of a consistently high standard, enhancing patient safety; it could be used as a positive example forothersNot ApplicableN/AATS 2017 International Conference5
HIGHLIGHTS2017 INNOVATIONS IN FELLOWSHIP EDUCATIONBoston UniversityBoston, MAAn Interactive, Flipped-Classroom Approach to Introducing Pulmonary Fellows to FlexibleBronchoscopyAbstract Authors: David Chiasiang Chu, MD and Christine Campbell Reardon, MDProgram Director: Christine Campbell Reardon, MDType of Program: Pulmonary/Critical CareBACKGROUNDFlexible bronchoscopy is an essential skill forpulmonary fellows to master over the course offellowship. In many programs, there is an orientationthat includes an introduction to bronchoscopy.However, the amount of instruction and hands-onexperience that fellows receive prior to performingclinical bronchoscopies is often very limited.Additionally, information obtained in the courseof performing clinical bronchoscopies may bevariable. In order to prepare our fellows to performbronchoscopy prior to performing the procedurein live patients, and to standardize the informationthey received, we developed an interactive, flippedclassroom and simulation-based curriculum tointroduce flexible bronchoscopy to pulmonaryfellows.METHODSWe performed a needs assessment of currentpulmonary fellows and faculty about the familiarityand comfort of fellows with bronchoscopy topicsand procedural skills. Based on the results ofthis survey, we created a curriculum of relevantbronchoscopy topics to provide more hands-ontraining early in the first year of training. Ourcurriculum included a half-day orientation, consistingof a 30-minute didactic session followed bybronchoscopy practice on plastic models and witha high-fidelity virtual reality (VR) simulator. Fellowswere instructed to complete 15 VR bronchoscopiesusing the simulator within the first 3 months oftraining. Additionally, over the first month of training,fellows participated in three 1-hour sessions ina flipped-classroom format covering generalbronchoscopy topics. Prior to these sessions,fellows were provided with 2-3 page outlinesof bronchoscopy topics we created based on a6current review of the literature. Each session wasfacilitated by a faculty member, using a PowerPointpresentation and notes we created to guide keyteaching points. The sessions began with questionsbased on the provided outlines to assess if fellowshad reviewed the material. Then, the fellowsparticipated in a case-based group discussionabout management decisions focused on the topicsassigned for each session.RESULTSIn this ongoing study, 6 first-year fellows wereassessed at the start of orientation using theAPCCMPD novice bronchoscopy cognitive test toestablish their baseline level of knowledge. Repeatassessment is planned after 12 months of clinicalrotations to determine the long-term retention ofinformation following participation in the curriculum.Their scores will be compared to the scores offellows (N 6) who completed their first year oftraining prior to implementation of the introductorycurriculum. Additionally, fellows will be surveyedon their perceptions of the utility of the sessions,training materials and self-directed practice with VRbronchoscopy.DISCUSSIONWe have created an interactive flipped classroomand simulation-based curriculum to coverbronchoscopy topics early in fellowship training. Ourinnovation lies in both the creation of quick referencematerials for fellows to use when planning andperforming bronchoscopy, and in the introductionof this information in an interactive format. Thiscurriculum was created to be self-contained andwould require little preparation to implement at otherinstitutions.ATS 2017 International Conference
HIGHLIGHTS2017 INNOVATIONS IN FELLOWSHIP EDUCATIONMount Sinai St. Luke’s-West-ICAHN School of MedicineNew York, NYPromoting Humanism in Pulmonary & Critical Care Medicine: For Fellows, By FellowsAbstract Authors: Mirna Mohanraj, MD; Nisha Kotecha, MD; Janet Shapiro, MDProgram Director: Mirna Mohanraj, MDType of Program: Pulmonary/Critical CareBACKGROUNDHumanism in healthcare is characterized by acompassionate relationship between physician andpatient. It reflects attitudes and behaviors that aresensitive to the values and background of others.Trainee burnout, poor cross-cultural interactions andlimited understanding of how patients experienceillness are a few factors that impair trainees’provision of humanistic care. Inattention to wellbeing may lead to job dissatisfaction, emotionalexhaustion and psychological impairment. Wedeveloped a fellow-devised and fellow-directedcurriculum to strengthen practice of patient-centeredcare and to promote physician well-being.METHODSA needs assessment was compiled from previouslyvalidated questionnaires on mindfulness,stress and burnout. Nine fellows completed thequestionnaire. Each month, a fellow leader – underfaculty supervision - becomes a ‘mini-expert’ in acurriculum topic by exploring relevant materials andcreating an interactive discussion forum. Sessiontopics range from moral distress to spiritualityin medicine to resilience in training. Fellowparticipants are engaged via various techniquesand resources including meditation, literatureand narrative medicine. In addition, the programaddresses several ACGME-mandated areas offocus: recognition of impairment in self and peers;fatigue mitigation; accountability to patients, societyand the profession; sensitivity to a diverse patientpopulation; leadership and communication.ATS 2017 International ConferenceRESULTSSelected notable results from the needs assessmentinclude: 78% felt emotionally drained after work;33% stated they have difficulty respecting patientvalues in decision-making; 45% reported that theytalked about work in a negative way; 22% reportedthey did their job mechanically; 56% felt that workdemands interfered with relieving patient suffering;33% felt they did not tolerate work pressure well.After five sessions, the baseline questionnaire wasre-administered with marked improvements inseveral areas. Only 22% felt emotionally drainedafter work; zero fellows felt they had difficultyrespecting patient values in decision-making, and12% reported talking about work in a negative way.While the course is in its early stages, qualitativereviews indicate that learned strategies areimmediately applicable to self-care and patientcare. As supervisors and mentors to junior trainees,fellows model learned strategies in daily interactions.Faculty have been inspired to engage via literaturereview and faculty development sessions in topics ofhumanism and well-being.DISCUSSIONTrainee-devised programs in humanism and wellbeing may be more impactful than those devisedat the program- or system-level. This is a uniqueprogram where fellows are both leaders andparticipants. The curriculum can be easily adoptedand adapted (with zero financial investment) formedical trainees at any level.7
HIGHLIGHTS2017 INNOVATIONS IN FELLOWSHIP EDUCATIONOregon Health & Science UniversityPortland, ORUsing High Fidelity Simulation-based Education to Improve Practitioner Competence andComfort in Ventilator ManagementAbstract Authors: Matthew D. Champion, MD; Jeffrey A. Gold, MD; Stephanie A. Nonas, MDProgram Director: Jeff A. Gold, MDType of Program: Pulmonary/Critical CareBACKGROUNDMechanical ventilation is an integral part oflife-supportive care for critically ill patients.Numerous studies demonstrate significantunderuse of lung protective (low tidal volume)ventilation. Failure to recognize the indicationsfor lung protective ventilation and incorrectimplementation of these practices may be due inpart to inadequate training. Didactic-only curriculafall short in preparing trainees to identify changingrespiratory physiology, such as air trapping, acutepneumothorax, or developing ARDS. Additionally,deliberate practice and assessment of traineesin mechanical ventilation is often limited by ourinability to control the environment, patient mix, andconcerns about patient safety. Simulation affordsa unique educational opportunity for teaching andassessment. We have developed a simulation-basedventilation curriculum aimed at increasing our traineereadiness to manage mechanical ventilation.METHODSWe identified gaps in practice related to ventilatormanagement through direct assessment, facultysurveys, and chart review of adverse patient events.Based on these identified gaps, we developed asimulation-based curriculum consisting of baselineknowledge and skills assessment, brief introductionto the simulation environment, and three interactivehigh-fidelity sessions designed to mimic an ICUenvironment. The trainees progressively “manage”a simulated patient on a ventilator – from intubationto writing orders to responding to developingARDS to managing ventilator emergencies. Eachsession contains three basic patient scenarios:1) normal lungs, 2) obstructive lung disease, and3) hypoxemic respiratory failure – each case witha built in ventilator “emergency” such as acutepneumothorax or mainstem intubation. Betweencases there is a structured formative debrief to goover core concepts and interactive question/answerwith the simulation leader. Following each sessionthe trainees evaluate the usefulness of each scenario8as well as their own comfort level in dealing with thescenario before and after the simulation.RESULTS15 critical care fellows (PGY 4-6) have participatedin our simulations, including 7 fellows as part oftheir introductory “bootcamp.” The overall courseevaluation for the ventilation/ARDS simulations was4.83/5; 86% felt the course taught new information/skills and 100% reported that training improved theircomfort with ventilation/ARDS (Figure). We havevalidated our ventilator knowledge pre-test, and arenow validating our skills and knowledge post-test.DISCUSSIONHigh-fidelity simulation is a viable educationalapproach to allow deliberate practice surroundingmechanical ventilation. Our ongoing studieswill determine the impact of training on clinicalperformance and we plan to expand our curriculumto the broader range of trainees and critical carepractitioners at our institution.FIGURE 1ATS 2017 International Conference
HIGHLIGHTS2017 INNOVATIONS IN FELLOWSHIP EDUCATIONThe Medical University of South CarolinaCharleston, SCA Longitudinal Curriculum in Critical Care Ultrasonography Training for Pulmonary andCritical Care Medicine FellowshipsAbstract Authors: Branden W. Luna DO; Nicholas J. Pastis MD; and John T. Huggins, MDProgram Director: Nicholas J. Pastis, MDType of Program: Pulmonary/Critical CareBACKGROUNDCritical care ultrasound (CCUS) is a noninvasive toolused to diagnose unspecified shock states, acuterespiratory failure, assess volume resuscitation,identify a source in septic shock, and for proceduralguidance. While ACGME guidelines recommend theuse of ultrasound to improve safety and successof many procedures done in the ICU, no officialstatement has been published regarding formalCCUS training during pulmonary and critical caremedicine (PCCM) fellowship. The authors aim todescribe a comprehensive CCUS curriculum used toteach thoracic, abdominal, and vascular ultrasound,along with basic echocardiography.METHODSThe curriculum consisted of three distincteducational domains: basic ultrasonography andknobology, image acquisition skills, and imageinterpretation skills. We included 3 phases ofCCUS training: (1) Onboarding distance learningcovering both basic ultrasonography/knobologyand image interpretation skills; (2)a 1-day bootcamp with traditional didactic teaching sessions,problem based learning sessions that emphasizesclinical application of CCUS findings, and hands-onpreceptor led training sessions; (3) a longitudinalreview which emphasizes building an image portfoliowith periodic mentor review and multidisciplinaryCCUS conferences. All content is based on learningobjectives as recommended by the 2009 ACCP/SRLF consensus statement on CCUS training.Evaluation of our subjects, which were 5 first yearPCCM fellows, was done by traditional multipleATS 2017 International Conferencechoice written testing along with multimedia platformbased questions and covered basic ultrasoundobjectives, image interpretation skills, and clinicalapplication questions. These domains were testedprior to beginning our educational intervention andimmediately after our boot camp sessions. Subjectswere also tested on image acquisition skills priorto our educational intervention using a simulatedpatient and checklist based evaluation. Theywere then retested 4 months into the longitudinalexperience using the same method as which theywere pre-tested prior to the boot camp intervention.RESULTSFive first year fellows at our institution underwent theCCUS curriculum. Fellows were evaluated in imageinterpretation and problem based critical applicationof CCUS. Cumulative performance on pre-testand post-test evaluations was 57.3% and 92%respectively. We also evaluated image acquisitionskills prior to and after our intervention and 4months of structured image portfolio developmentand dedicated educational sessions on CCUS. Thecumulative performance on pre-test and post-testswere 50.1% and 82.4% respectively.DISCUSSIONCCUS curriculum incorporated into fellowshiptraining which utilized online distance learningmodules, traditional didactic sessions, problembased learning exercises, and hands-on trainingwith preceptor oversight was successful in achievinginitial and longitudinal competency in a small cohortof fellows.9
2017 INNOVATIONS IN FELLOWSHIP EDUCATIONHIGHLIGHTSFIGURE 1: GRAPHIC REPRESENTATION OF CCUS CURRICULUMFIGURE 2: FELLOW PERFORMANCE ON BASIC ULTRASONOGRAPHY AND IMAGE INTERPRETATION DOMAINS10ATS 2017 International Conference
HIGHLIGHTS2017 INNOVATIONS IN FELLOWSHIP EDUCATIONEastern Virginia Medical SchoolNorfolk, VAImplementation of a Multifaceted Faculty Development ProgramAbstract Authors: Joshua Sill, MD; Michael Hooper, MD; Heather Newton, EdD; Agatha Parks-Savage, RN, EdDProgram Director: Joshua Sill, MDType of Program: Pulmonary/Critical CareBACKGROUNDThe Accreditation Council for Graduate MedicalEducation (ACGME) stipulates that all internalmedicine residency programs and subspecialtyfellowship programs must monitor and track facultydevelopment. The ACGME places specific emphasison this topic, requiring periodic evaluations of facultydevelopment curricula as part of the ongoing selfstudy process and annual program evaluations.Challenges to faculty development include limitedfaculty time, discordant participant schedules,and the resources required for administration ofthe program. Eastern Virginia Medical Schoolimplemented a new pulmonary and critical carefellowship program in the spring of 2014. Inkeeping with ACGME policy, we developed afaculty development program for the fellowship’sfaculty members. We present our experience withthe development of a new, multifaceted facultydevelopment program.RESULTSOverall feedback from faculty members waspositive. They found the curriculum to be helpful andnot overly time consuming. Having required itemseither coincide with previously scheduled meetingsor be available in a short, self-directed, online formatwas appreciated by faculty members. The sitevisitors during a recent ACGME lauded the facultydevelopment program, stating that it was in keepingwith “best educational practices.”METHODSIn developing our program’s faculty developmentcurriculum, we sought to maximize opportunities forcollaboration with our core residency program andwith the sponsoring institution. Doing so, allowed usto focus our resources on items that were specific toour subspecialty, rather than duplicating the effortsof others. Our curriculum included several differenttypes of activities. 1) Concise, online, computerbased training modules were developed withassistance from the sponsoring institution. 2) Brieftalks and small group discussions were presentedby different faculty members at the beginning ofmonthly faculty meetings. 3) Highlights from theminutes of the Graduate Medical Education Councilmeeting were emailed to faculty members monthlyfor review. 4) Faculty members were encouraged toattend national educational meetings or educationalsessions at national subspecialty meetings. 5)Faculty were encouraged to attend an ongoingfaculty development lecture series provided by thesponsoring institution.REFERENCESPhilibert I, Lieh-Lai M. A practical guide tothe ACGME self-study. Journal of GraduateMedical Education. September 2014; 612-614.Acknowledgements Linda Archer, PhD, Vice Deanfor GME, Designated Institutional Official, EasternVirginia Medical School Chrisandra Knight, ProgramCoordinator, Pulmonary and Critical Care MedicineFellowship Program, Eastern Virginia Medical SchoolElza Mylona, PhD, MBA, Vice Dean for FacultyAffairs and Professional Development, EasternVirginia Medical SchoolATS 2017 International ConferenceCONCLUSIONSFaculty development is an important part of anyACGME-approved internal medicine subspecialtyfellowship program. Working within the frameworkof pre-existing institutional and core residencycurricula may help to make the process moreefficient. Limiting the time requirements imposedon the faculty members may help improve facultyparticipation.11
HIGHLIGHTS2017 INNOVATIONS IN FELLOWSHIP EDUCATIONMount Sinai St. Luke’s-West-ICAHN School of MedicineNew York, NYTeaching Skills of Quality Improvement in a Pulmonary & Critical Care Fellowship:A Team Project in the Ambulatory SettingAbstract Authors: Edwardine Mirna Mohanraj, MD; Steven Chakupurakal, MD; and Janet Shapiro, MDProgram Director: Edwardine Mirna Mohanraj, MDType of Program: Pulmonary/Critical CareRATIONALEImprovement in patient outcomes and reductionin medical errors are the focus of healthcareinstitutions. Fellows entering subspecialty fields arecharged with ‘improving the quality and safety ofhealthcare at both the individual and systems levels’.Few resources exist to aid in the design of feasibleand sustainable curricula in quality and safety. Wedeveloped a novel, longitudinal curriculum in qualityimprovement for subspecialty fellows centered on anannual team project in the ambulatory setting. Theaims were to teach principles of quality improvementand safety, promote trainee monitoring of practiceimprovement, implement process improvements,and foster teamwork and leadership skills. Theteam project provided a framework for fellows toachieve competence in practice-based learning andimprovement and systems-based practice.METHODSThe longitudinal QI curriculum consists of 4 distinctelements: completion of the Institute for HealthcareImprovement Basic Certificate in Quality andSafety (year 1), participation in departmental anddivisional QI committees and initiatives (years 2-3),development and leadership of individual QI projects(years 2-3) and participation in an annual groupQI project (all years). 9 Pulmonary & Critical Carefellows worked jointly on this project under facultysupervision. The fellows identified a practice gap:patients with high-risk indeterminate pulmonarynodules had inconsistent surveillance imaging.Fellows elected to improve the process for timelyradiographic monitoring. The project began withinstruction on tools of quality improvement. Seniorfellows led three subgroups: mission statement,process map, and data collection strategy. Progresswas presented at bimonthly project meetings.12RESULTSThe ‘mission statement’ subgroup reviewed thepulmonary nodule literature and articulated the goalthat 100% of patients with indeterminate nodulesshould undergo timely chest CT surveillance. The‘process map’ subgroup elucidated the processfor CT scan scheduling and identified multiplepatient-based and systems-based roadblocks. Allfellows reviewed their patient panels: 660 clinicvisits over a three-month period. Baseline datarevealed that only 80% (21/26) of ordered CT scanswere actually scheduled. A process of stream-liningthe appointment and authorization process wasaccomplished with interdisciplinary involvement
excellence this year. The University of Washington submitted the top Innovations abstract for 2017. University of Washington Leadership Education for Critical Care Fellows Using Simulation 4 Boston University An Interactive, Flipped-Classroom Approach to Introducing Pulmonary Fellows to Flexible Bronchoscopy 6 Mount Sinai St. Luke's-West-