Transcription
National Oral Health Conference - Louisville - April 17, 2018Innovative Interprofessional PediatricDentistry Curriculum & Infant Oral CareProgram Address Disparities in Oral HealthFrancisco Ramos-Gomez DDS, MPH, MS 1Hamida Askaryar MPH, RDH, MCHES 11 UCLASession: Oral HealthAbstract: 388322School of Dentistry1
Presenter DisclosuresThe following personal financial relationships withcommercial interests relevant to this presentation existedduring the past 12 months:No relationships to disclose2
Objectives What is SPICE-PD? Describe the IPE curriculum Describe Infant Oral care Program (IOCP)and community collaborations SPICE-PD evaluation framework3
SPICE-PD: Strategic Partnership for InterprofessionalCollaborative Education in Pediatric Dentistry Establish an Integrated Oral andPrimary Healthcare Clinical TrainingProgram Prepare postdoctoral pediatric dentiststo provide care for underserved andspecial needs groups and communities Enhance training in dental public healthhttp://www.uclachatpd.org4
Understanding Children’s oral health policy andadvocacy5
Scope of the Problem ECC – Most common chronic disease of childhood (60-90% worldwide1,2,3) Medicine/Nursing & Dentistry- “Silos” usually “See adentist” yet insufficient providers in many underserved communities Not traditionally a part of medical school or pediatric med residencytraining.USPSTF has recommended Fluoride Varnish application in Primary Caresince 2014 5 – PCPs see children up to ten times first two years- PCPs arewell positioned to ameliorate this disease burden.6
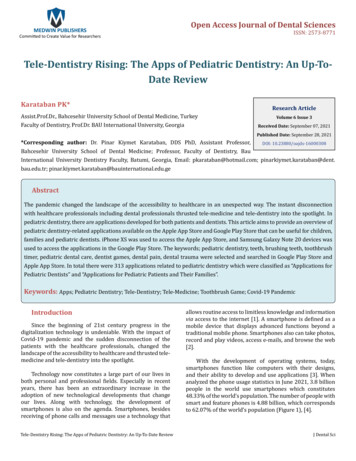
As a health care professional(MDs & RNs), how often do you Apply Fluoride varnishPerform oral health risk assessments &screen for Early Childhood Caries (ECC)Provide anticipatory guidance for oralhealth70%16%17%30%20%30%23%7% 3%20%40%3%16%(N 30)NeverRarelySometimesOftenAlways7
3 Part IPE CurriculumA: Smiles forLife Modules/App(6) &selectedreadingsB: Oral healthlecture &fluoridevarnish labC: Clinical IPEexperience atInfant Oral CareProgram (IOCP) Needed – Oral Assessment missing in most programso HEENT INCLUDE “oral”: HEENOT (Haber et al., 2015 4)o Core clinical competencies for PCPso Lack awareness of oral care Lifespan Approach – What to assess interventionso HRSA grant focus: prenatal child to 5 yrs old8
3 Part IPE CurriculumA: Smiles forLife App &selectedreadingsB: Oral healthlecture &fluoridevarnish labC: Clinical IPEexperience atIOCP Caries Risk Assessment Tools (CRA) CAMBRA 7 (Dr. Ramos-Gomez) – Lecture by Pediatric Dentist American Academy of Pediatrics - Oral HealthAssessment Tool 8 Reviewing videos/cases studies Fluoride varnish Lab - with RDH Comfort with equipment9
Training A & B10
White SpotLesions11
AAP Oral Health Assessment Form for PCPs 9,10 Document caries risk anticipatoryguidance Available free12
3 Part IPE CurriculumA: Smiles forLife App &selectedreadingsB: Oral healthlecture &fluoridevarnish labC: Clinical IPEexperience atInfant Oral Careprogram IPE with Pediatric Dentistry – A first Infant Oral Care Clinic – true IPE Clinical Practicums Training scheduling issues- align schedulesof MDs, RNs, pediatric & general dentalresidents (AEGDs/GPRs)13
Infant Oral Care Program (IOCP)www.uclaiocp.org Interprofessional training site- emphasizing prevention. Med/Dental integrated community clinics but also nontraditional sites such as WIC, preschools, and Head Start. Majority of patients: low SES, underserved & families ofcolor.Over 978 children seen at IOCP (2010-now)- 254 casesmaintained with no decay, 40 cases maintained at WSL, and48 cases averted.14
Working with community partners: rotations at WIC,Head Start, and Mobile Van- understanding the socialdeterminants of health15
PNPs with Pediatric Dentist colleaguesat IOCP Value IPE experience: additional learning Champion oral health in Primary Care16
PNPs (RNs) Student FeedbackImmediately incorporate new evidence into practice First lecture by a Dentist – value IPE First time students learned of “white spots” – or knew to look Misconceptions/outdated information about oral preventive health practices Not aware of 2014 ADA, AAPD, AAP 8 changes and recommendations Work in Hospitals & other community clinics (Current PT work environment formany students) Notice poor quality toothbrushes and lack of oral care began examining teeth and finding problems, educating caregivers aboutoral health practices (sippy cups; bottles; juice/snack consumption, etc.) Clinical PNP Experience Barriers: No/Few Primary Care sites supply/apply fluoride varnish17
Implications – Care DeliveryDespite USPSTF 5 recommendation and state reimbursement, fewprimary care practices incorporate fluoride varnish application. Need to increase skills for existing & train more PCPs Caries Risk Assessment Fluoride varnish Preventive practices Expand training to PHN nurses (home visiting) – Low income groups Expand training to medical students, other medical residents(Family Physicians) & Advance Practice Registered Nurses (APRNs)18
SPICE PD EvaluationProgramDevelopmentKnowledge &Skills gainedProfessionalChoices19
Evaluation data collection methodsYear-end surveyAlumni InterviewsBoard Exam ResultsAlumni SurveyEnrollment records (MedHubresidency mgmt.)Clinical Data (EDR/EHR QualityImprovement)20
Agreement of MDs, PNPs, & general dental residents(AEGDs/GPRs) with the following statements:SPICE-PD program has prepared me well toaddress the oral health needs of special needs& vulnerable populationsSPICE-PD faculty provided importantperspectives on oral health that I did notreceive elsewhere in my graduate education25%17%My experience in SPICE-PD has positivelyinfluenced my professional practice as regards 10%oral health.(N 92)Neutral39%43%53%Agree32%31%33%Strongly Agree21
Agreement of MDs & PNPs with the followingstatements: SPICE-PD has Primary care professionals should incorporateoral health in routine patient care.100%improved my skills to screen for EarlyChildhood Caries100%improved my skills to apply Fluoride varnish90%increased my sense of responsibility to applyFluoride varnish90%(N 30)Agreed or Strongly Agreed22
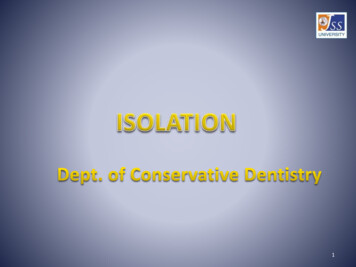
Agreement of general dental residents (AEGDs/GPRs)with the following statements: SPICE-PD has has increased my appreciation of theimportance of providing preventive oral healtheducation to parentshas increased my intention to perform awritten caries risk assessmenthas increased my comfort with seeing infants& toddlers in my practice(N 41)73%9%20%24%NeutralAgree17%66%10%61%7%Strongly Agree23
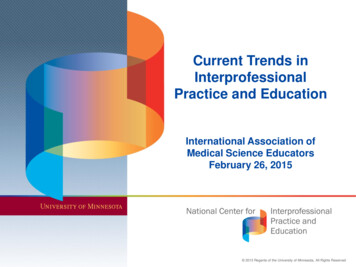
SPICE-PD # of Participants 2015-2020: 319 (est.)706050403020100SPICE YEAR 12016/0217SPICE YEAR 22016/2017SPICE YEAR 32017/2018SPICE YEAR 42018/2019SPICE YEAR 52019/2020Pediatric medical residents1726312626PNPs1513151515AEGDs/ GPRs2424242424Total (*est.)566370656524
Conclusions:1.2.3.Broad dissemination of interprofessionaltraining in preventive oral health may helpdecrease the overall burden of childhoodcariesAn oral health curriculum that capitalizes onopportunities in interprofessionalcollaboration can improve confidence andpractice in the prevention and managementof childhood caries.Medical/dental integrated community settingsespecially in underserved communities is thefuture for childhood caries prevention.25
AcknowledgementsInterprofessional Training Grant D88HP20129For more information:SPICE-PD website http://www.uclachatpd.orgDr. Ramos-Gomezfrg@dentistry.ucla.eduHamida Askaryar MPH, RDHhaskaryar@dentistry.ucla.eduSPICE-PDUCLA School of Dentistry10833 Le Conte Ave.Room 23-020Los Angeles, CA 9009526
References1.World Health Organization. (2012). Oral Health Fact Sheet . Available 18/en/2.Folayan, M. (2014). Early Childhood Caries as a global epidemic in developed and developing countries, slide 6 [Powerpointslides]. Retrieved from:https://www.researchgate.net/profile/Morenike Folayan/publication/270271412 Early Childhood Caries as a Global Epidemic in developed and developing countries/links/54a3cf5b0cf267bdb90450d13.Dental Health Foundation. (2016). "Mommy, it hurts to chew" The California Smile Survey. An Oral Health Assessment ofCalifornia's Kindergarten and 3rd Grade Children.4.Haber J, Hartnett E, Allen K, Hallas D, Dorsen C, Lange-Kessler J, Lloyd M, Thomas E, Wholihan D. (2015). Putting the mouthback in the head: HEENT to HEENOT. Am J Public Health, 105(3), 437-41.5.Moyer VA. (2014). US Preventive Services Task Force. Prevention of dental caries in children from birth through age 5years: US Preventive Services Task Force recommendation statement. Pediatrics, 133 (6), ng6.Smiles for Life: A National Oral Health Curriculum. 3rd Edition. Society of Teachers of Family Medicine. Available -Gomez F, Ng MW (2011).Into the future: keeping healthy teeth caries free: pediatric CAMBRA protocols. J CalifDent Assoc, 39 (10), 723-33.8.American Academy of Pediatrics. Section on Oral Health. (2014). Maintaining and improving the oral health of youngchildren. Pediatrics, 134 (6), 1224-9. 6/12249.American Academy of Pediatrics. Oral Health Risk Assessment Tool. Available 20Documents/OralHealthRiskAssessmentTool.pdf10. American Academy of Pediatrics. Recommendations for Preventive Pediatric Health Care Bright Futures/American Academy ofPediatrics. February 2017. Available at: https://www.aap.org/en-us/Documents/periodicity schedule.pdf27
Assessment Tool 8 Reviewing videos/cases studies . Training scheduling issues- align schedules of MDs, RNs, pediatric & general dental residents (AEGDs/GPRs) 13 A: Smiles for Life App & . 2016/0217 SPICE YEAR 2 2016/2017 SPICE YEAR 3 2017/2018 SPICE YEAR 4 2018/2019 SPICE YEAR 5 2019/2020