Transcription
The SpirometryHandbook forprimary careA guide to performing and interpretingspirometry for primary care healthprofessionals
The spirometry handbook for primary careAbout this handbookThe spirometry handbook for primary care is intendedas a guide for health professionals performing andinterpreting spirometry in clinical practice, to ensurethat high-quality testing is available and accessiblefor those with respiratory conditions.It was developed by an expert working group ofnurses, doctors and respiratory scientists convenedby National Asthma Council Australia.A quick reference guide accompanies this handbook(available at: www.nationalasthma.org.au)AcknowledgementsWorking group 2020 editionMs Marg Gordon (Chair), RN, asthma andrespiratory educatorDr Ian Almond, general practitionerMs Kim Bridges, respiratory scientistMs Pauline Hughes, respiratory nurse practitionerDr Celia Lanteri, respiratory physicianDr Leanne Rodwell, respiratory scientistMs Judi Wicking, RN, asthma and respiratory educatorOther acknowledgementsThe first edition of this handbook (1995) wascommissioned by the Thoracic Society of Australia andNew Zealand (TSANZ) and was written by ProfessorRob Pierce MD, FRACP, Director, Respiratory Medicineand Sleep Disorders, Austin and Repatriation MedicalCentre, Victoria, and Associate Professor DavidP Johns PhD, CRFS, FANZSRS, Adjunct PrincipleResearch Fellow, School of Medicine, University ofTasmania. It was revised by Professor Johns for theJuly 2004 and March 2008 editions published byNational Asthma Council Australia.National Asthma Council Australia thanks ProfessorJohns for reviewing the 2008 edition in preparationfor the current edition, Eleonora (Nory) Del Colle forproviding data for Figure 4, and Queensland HealthSpirometry Training Program for permission to adaptits interpretation algorithm (Figure 11).Recommended citationNational Asthma Council Australia. The spirometryhandbook for primary care. Melbourne; NationalAsthma Council Australia: 2020. 2020 National Asthma Council AustraliaA guide to performing and interpreting spirometryfor primary care health professionalsEndorsed by the Thoracic Societyof Australia and New Zealand
ContentsIntroduction5Spirometric indices7Spirometer specifications9Spirometry reference values10Safety11Pre-appointment instructions for patients14Preparing the spirometer16Preparing the patient to perform the test17Performing the test18Acceptability and repeatability19Completing the testing session26Selecting results to record27Assessing bronchodilator responsiveness testing (‘reversibility’)28Identifying abnormal ventilatory patterns30Clinical interpretation of spirometry35Quality assurance36Appendix: Medicare item numbers for office-based spirometry38More information38References39
The spirometry handbook for primary care4A guide to performing and interpreting spirometryfor primary care health professionals
Spirometry is an objective physiologicaltest of lung function and is essential inthe management of respiratory disease.A spirometer measures how much, and howquickly, air can be exhaled in a single blow fromfull lungs. Some spirometers also measureairflow during inspiration. Results are availableimmediately.Spirometry performance requirementsi and testingmethods are standardised.1, 2 Lung function isassessed by comparing the individual’s results withnormal reference values and with previous results,if available.Correct spirometry technique is crucial toobtaining reliable results for making a diagnosisor monitoring management of respiratoryconditions. The test requires effort by the patient,so there must be cooperation between the operatorand the patient, and continual coaching by theoperator during the test.With appropriate coaching, almost all adults andmost children aged 6 years and older attendinggeneral practice can correctly perform thespirometry test.The operator is responsible for determining whichresults are suitable for clinical interpretation. It isessential to meet acceptability and repeatibilitycriteria for each test performed, before using theresults to make clinical assessments.Clinical roles of spirometryAirflow during forced expiration is affected by theelastic recoil of lung tissue, resistance of upstreamairways, and the strength of respiratory muscles.Expiratory flow can be reduced by narrowingof the airway lumen or thickening of the airwaywall. Abnormal inspiratory flow (if measured)in the presence of otherwise normal spirometryis a feature of upper airway dysfunction, whichrequires specialist investigation.The spirometry handbook for primary careIntroductionSpirometry is used in the investigation ofrespiratory symptoms, in the diagnosis ofrespiratory conditions such as chronic obstructivepulmonary disease (COPD) and asthma (Table 1),in monitoring the treatment of respiratory diseases,in case-finding among asymptomatic patients(e.g. smokers at risk of COPD), in the assessmentof preoperative risk, in monitoring lung health inworkers occupationally exposed to respiratoryirritants or allergens, in disability/impairmentevaluations performed for occupational,recreational or insurance purposes, and inclinical and population research.The main purpose of this guide is to ensure thatall patients with asthma or other respiratoryconditions have access to high-quality spirometry.i The 2019 joint official statement on the standardisation of spirometry by the American Thoracic Society (ATS) and EuropeanRespiratory Society (ERS)2 introduced new requirements for the manufacture of spirometers. These performance standards applyto new spirometers, but are not met by all spirometers in use in Australia. During this transition, all spirometers used in clinicalpractice must meet the ATS/ERS 2005 standard1 or the 2019 standard.2A guide to performing and interpreting spirometryfor primary care health professionals5
The spirometry handbook for primary careTable 1. Recommendations for spirometry in nationalclinical guidelines for asthma and COPDAsthma3COPD4Any patient with suspected asthmaInvestigation of:Making the diagnosis of asthma*— unexplained breathlessnessConfirming a past diagnosis— cough that is chronic (daily for 2 months),intermittent, unusualAssessing risk of flare-upsInvestigating recent worsening of asthma controlMonitoring response to a change in treatmentPeriodically reviewing asthma (e.g. every1–2 years)At every visit for patients with severe asthmaor patients with poor perception of airflowlimitation (e.g. those who do not feel any differentwith a 15% decrease or increase in FEV1)— frequent or unusual sputum production— relapsing acute infective bronchitisCase-finding in people exposed to tobaccosmoke or occupational dusts and chemicals,or patients with a strong family history of COPDMaking the diagnosis of COPD†Reviewing treatment response and diseaseprogression in people with COPD* Spirometric criteria in combination with clinical findings; the diagnosis of asthma cannot be made solely on the basis of spirometryfindings, but also depends on clinical findings including symptoms and exclusion of alternative diagnoses.† Spirometric assessment is essential to the diagnosis.6A guide to performing and interpreting spirometryfor primary care health professionals
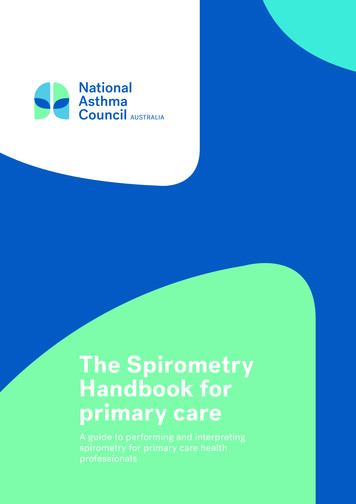
The key indices measured by a spirometer(Figure 1) are forced vital capacity (FVC), forcedexpiratory volume in 1 second (FEV1), peakexpiratory flow (PEF), and the ratio of FEV1 to FVC(FEV1/FVC ratio). If inspiratory airflow is assessed,forced inspiratory vital capacity (FIVC) is alsomeasured (Table 2).Additional measuresof lung functionAdditional (including non-spirometric)measures of lung function are sometimesperformed in lung function laboratories,if required in the further investigation oflung conditions.Other indices, such as forced expiratory flowbetween 25% and 75% of FVC (FEF25–75% ) andforced expiratory volume in 6 seconds (FEV6 ),are not commonly used as they have limitedclinical value.These include residual volume (the volumeremaining in the lung after a maximalexhalation), functional residual capacity (thevolume of air present in the lungs at the endof passive expiration), total lung capacity(the maximum volume of air that can becontained in the lungs), and gas transfer(the ability to transfer gas from the lungsto the blood).Figure 1. Idealised spirometry tracings froma healthy individual showing measurementof indicesA. Normal volume–time curve(spirogram)The spirometry handbook for primary careSpirometric indicesB. N ormal flow–volume curve(‘loop’ if includes inspiratory curve)PEFExpirationVolumeFlowFEF 25%FEF 75%FVCFEV1VolumeFVC01InspirationTime (seconds)FEV1: forced expiratory volume in one second; FVC: forced vital capacity; FEF25%: forced expiratory flow at the point where 25% ofFVC has been expired; FEF75%: forced expiratory flow at the point where 75% of FVC has been expiredA guide to performing and interpreting spirometryfor primary care health professionals7
The spirometry handbook for primary careTable 2. Spirometric indicesAbbreviation (units)NameDefinitionNotesFVC (litres)Forced vital capacityThe maximum volume ofair that can be expiredduring a single expiratorymanoeuvre using maximaleffort initiated followinga full inspirationIndicates lung capacityFEV1 (litres)Forced expiratory volumein 1 secondThe volume of air forcefullyexpired from full lungsduring the first second ofan expiratory manoeuvreIndicates how quickly fulllungs can be emptied,reflecting airway calibreFEV1/FVC (ratio)Ratio of forced expiratoryvolume in 1 second toforced vital capacityFEV1 expressed as afraction or percentage ofFVCIndicates whether expiratoryairflow obstruction is presentPEF (litres/second orlitres/minute)Peak expiratory flowThe maximal expiratoryflow achieved during themanoeuvreUsed for assessing effortFIVC (litres)Forced inspiratoryvital capacityThe maximum volume ofair that can be inspiredduring a single inspiratorymanoeuvre using maximaleffort following a forcedexpiratory manoeuvreComparison of FIVC and FVChelps determine whetherthe patient began the forcedexpiration from full inflationKey indicesLimited clinical applicationAll volumes and flows are reported at body temperature and pressure saturated with water vapour (BTPS)8A guide to performing and interpreting spirometryfor primary care health professionals
Almost all spirometers currently used in Australia are flow spirometers. Flow spirometers use a sensor tomeasure flow and calculate volume electronically or digitally. The most commonly used sensors detectflow by measuring the pressure drop across resistance, electronically counting the rotation of a turbineblade, or by ultrasound.The spirometry handbook for primary careSpirometerspecificationsThe volume-displacement spirometer is an older type that is now rarely used in general practice. Volumedisplacement spirometers usually provide a direct measure of respired volume from the displacement of apiston (rolling seal) or bellows (e.g. wedge bellows).All spirometers used in clinical practice or research should meet performance criteria developed by theAmerican Thoracic Society (ATS) and European Respiratory Society (ERS).ii These criteria were updated in2019 (Table 3).2Table 3. ATS/ERS spirometer performance criteria2The current standard includes the following:— The spirometry system meets International Organization for Standardization (ISO) Standard 26782.*— Volume–time and flow–volume curves are displayed in real time.— The volume–time curve shows exhalation from point of maximal inspiration or 1 second beforetime zero# (whichever occurs first), and up to either the end of the plateau or the beginning of nextinspiration (depending on whether the inspiratory manoeuvre is being measured).— Aspect ratio is 2:1 for printed volume–time curves.* Exception: maximal permissible error of 2.5% for spirometer when volume accuracy tested with a 3-litre syringe, for whichpermissible error is 0.5%; total permissible error is 3.0%#See Definition of start timeiiSpirometers manufactured before introduction of the current standard2 should meet the 2005 standard.1A guide to performing and interpreting spirometryfor primary care health professionals9
The spirometry handbook for primary careSpirometryreference valuesAn individual’s spirometry results are comparedwith reference values obtained from a well-definedpopulation of normal subjects matched for sex,age, height and ethnic origin and using similar testprotocols with carefully calibrated and validatedinstruments.1The lower limit of normal (LLN) is usually definedas the cut-point for the bottom 5% of normaldistribution (i.e. only 5% of the normal healthypopulation fall below this value). Comparisonwith LLN is useful for clinical interpretation.An individual’s results should also be comparedover time with their ‘personal best’, because serialtrends provide a better indication of change in lungfunction than predicted values.SexWhen adjusted for height and age:5— FEV1, FVC, FEF25–75% and PEF are higherin males than in females— FEV1/FVC ratio is slightly lower in males thanin females.AgeDuring adulthood there is a gradual fall in FEV1,FVC, FEF25–75% and PEF.5FEV1/FVC also decreases with age in adults,because FEV1 declines more over time than FVC.5Ethnic originCompared with Caucasians, FEV1 and FVC valuesare lower in ethnic groups whose thorax is shorterrelative to their height.6 However, there is littledifference in FEV1/FVC ratio or PEF betweenethnic groups.5When adjusted for age and height:— Caucasians are among the ethnic groups withthe largest FEV1 and FVC values6— South-East Asians (including southern Indians),Sub-Saharan Africans and African-Americanshave FEV1 and FVC values lower than thoseof Caucasians5, 6— Aboriginal and Torres Strait Islander peoplehave FEV1 and FVC values lower than those ofCaucasians but higher than those of African‐American people, based on findings in childrenand young adults aged 3–25 years.7Choice of reference valuesMultiple sets of reference values are available.The Global Lung Initiative (GLI) 2012 referencedataset5 is recommended for use in Australia andNew Zealand.8 It includes values for age ranges3–95 years and for relevant ethnic groups.The GLI-2012 category ‘other/mixed’ shouldbe selected when performing spirometry forAboriginal and/or Torres Strait Islander people.7, 8HeightAll indices except FEV1/FVC increase withstanding height.10A guide to performing and interpreting spirometryfor primary care health professionalsNOTE: The use of reference values obtainedfrom the third US National Health and NutritionExamination Survey (NHANES III) 9 is no longerrecommended.
Risks associated with the forcedexpiratory manoeuvrePeople are unlikely to achieve optimal or repeatableresults if they have:10Spirometry is generally safe. However, it requiresmaximal effort, which could result in transientbreathlessness, cough, syncope, chest pain, oxygendesaturation or incontinence.— an acute respiratory tract infection(e.g. cold or flu)In patients with poorly controlled asthma, theforced manoeuvre can also induce bronchospasm.These people may show progressive decreasein FEV1 with successive blows.Spirometry should not be performed in patientsat risk of complications due to high thoracic,abdominal, intracranial and intraocular pressuresgenerated by the forced expiratory manoeuvre(Table 4).2 When there is doubt about the safety ofperforming spirometry, the operator should consultthe referring clinician or a specialist, as required.A guide to performing and interpreting spirometryfor primary care health professionalsThe spirometry handbook for primary careSafety— chest or abdominal pain of any cause— nausea— diarrhoea— oral or facial pain exacerbated by a mouthpiece— stress incontinence— dementia.11
The spirometry handbook for primary careTable 4. Relative contraindications for spirometry2Risk considerationCondition(s)Increase in myocardialdemand or blood pressureAcute myocardial infarction within 1 weekSystemic hypotension or severe hypertensionSignificant atrial/ventricular arrhythmiaUncompensated heart failureUncontrolled pulmonary hypertensionAcute cor pulmonaleClinically unstable pulmonary embolismHistory of syncope related to forced expiration/coughIncrease in intracranialor intraocular pressureCerebral aneurysmBrain surgery within 4 weeksRecent concussion with continuing symptomsEye surgery within 1 weekIncreases in sinus andmiddle ear pressureSinus surgery within 1 weekIncrease in intrathoracicand intra-abdominalpressurePresence of pneumothoraxMiddle ear surgery or infection within 1 weekThoracic surgery within 4 weeksAbdominal surgery within 4 weeksLate-term pregnancyInfection controlActive or suspected transmissible respiratoryor systemic infection (e.g. tuberculosis)Conditions predisposing to transmissionof infection (e.g. hemoptysis)Significant secretionsOral lesions or oral bleeding12A guide to performing and interpreting spirometryfor primary care health professionals
Cleaning and disinfectionAlthough few cases of infection transmission viaspirometers have been documented, spirometryequipment has the potential to transmit pathogensthrough mouthpieces, valves and tubing, eitherthrough direct contact with bodily fluids or throughdroplet infection.2Regardless of the filter or mouthpiece used,the spirometer should be cleaned and disinfectedperiodically (weekly or monthly) according tothe manufacturer’s instructions.Infection risk can be minimised by the routine useof infection control measures (Table 5). Theseinclude the use of disposable mouthpieces,mouthpiece valves and in-line filters, and cleaningand disinfection, in addition to general hygienesuch as handwashing.Disposable mouthpiecesMost spirometers use a single-use (disposable)sensor or mouthpiece.Reusable mouthpieces must be cleaned,disinfected and dried after each patient. Theseare now rarely used and are not recommended.Mouthpiece valvesOther devices use disposable mouthpiecescontaining a one-way valve to prevent inspirationthrough equipment. Only expiratory spirometrycan be performed when these are used.In-line filtersThe usual way to prevent contamination of theinterior surfaces of the spirometer is to use adisposable, low-resistance micro-aerosol filterinserted between the patient and spirometer.These in-line filters appear to be effective inreducing the risk of bacterial cross infectionduring inspiration,11 but the use of filters does noteliminate the need for cleaning and disinfection.10A guide to performing and interpreting spirometryfor primary care health professionalsIf disassembling the spirometer for cleaning,it is essential to:— thoroughly dry the components beforereassemblingThe spirometry handbook for primary careInfection risk— check the spirometer for correct operation— recalibrate, if necessary.Table 5. Summary of infectioncontrol measuresHandwashing between patients and afterhandling the spirometerSingle-use mouthpieces or sensorsViral/bacterial filtersAutoclaving or disposal of spacersFollowing manufacturer’s recommendationsfor cleaning and disinfectionUse of personal protective equipment(e.g. gloves) as neededAvoiding spirometry in patients with potentiallytransmissible diseasesAvoiding standing directly in front ofcoughing patient13
The spirometry handbook for primary carePre-appointmentinstructions forpatientsGeneral instructionsWithholding bronchodilatorsPatients should be advised to avoid:2When spirometry is performed as a diagnostic test,inhaled bronchodilators should be withheld beforethe test (Table 6). However, patients who use shortacting beta2 agonists (e.g. for asthma or COPD) forsymptom relief should still use these if needed.3— smoking (including the use of electroniccigarettes or water pipe) for at least1 hour before the test, to prevent acutebronchoconstriction— consuming alcohol or other intoxicants forat least 8 hours before the test, to preventproblems with coordination, physicalperformance or comprehension— exercising vigorously for at least 1 hour beforethe test, to prevent potential exercise-inducedbronchoconstriction.It is also helpful to advise patients to wear looseclothing that does not restrict the chest orabdomen2 and empty their bladder before thetesting session.Patients who use a short-acting beta2 agonistinhaler (e.g. those with asthma or COPD), shouldbe asked to bring their own inhaler and spacerto use when testing bronchodilator responsiveness.14A guide to performing and interpreting spirometryfor primary care health professionalsPatients who take regular long-actingbeta2 agonists in combination with inhaledcorticosteroids for asthma should not be advisedto withhold their medication before spirometryunless they are undergoing medically supervisedwithdrawal for the purpose of confirming thediagnosis.3The operator should document whether theperson has taken any bronchodilator on the dayof spirometry, including the dose and time taken.
Short-acting beta2 agonists (SABAs)The spirometry handbook for primary careTable 6. Recommended minimal bronchodilator withholding times4 hoursSalbutamol (e.g. Asmol, Ventolin)Terbutaline (e.g. Bricanyl)Short-acting muscarinic antagonists (SAMAs)12 hoursIpratropium (e.g. Atrovent)Long-acting beta2 agonists (LABAs)with twice-daily dosing24 hoursFormoterol (e.g. DuoResp Spiromax, Flutiform,Oxis, Symbicort)Salmeterol (e.g. Fluticasone and salmeterol Cipla,Serevent, Seretide)Long-acting beta2 agonists (LABAs)with once-daily dosing36 hoursIndacaterol (e.g. Onbrez, Ultibro)Olodaterol (e.g. Spiolto)Vilanterol (e.g. Anoro, Breo, Trelegy)Long-acting muscarinic antagonists (LAMAs)Aclidinium (e.g. Bretaris, Brimica)Glycopyrronium (e.g. Seebri, Ultibro)Tiotropium (e.g. Braltus, Spiriva, Spiolto)Umeclidinium (e.g. Anoro, Incruse, Trelegy)Withholding times apply when spirometry is performed as a diagnostictest (not for monitoring response to treatment). For combination therapiescontaining more than one listed medicine, use the longer withholding time.A guide to performing and interpreting spirometryfor primary care health professionals15
The spirometry handbook for primary carePreparing thespirometerBefore a testing session, the spirometer shouldbe prepared by following the manufacturer’sinstructions.This includes determining the zero flow levelfor the spirometry system (with the spirometerblocked), if required for the device.Setting upThe operator should check that the spirometerhas been correctly set up and configured, whichincludes ensuring that the correct reference valueshave been selected and the LLN value calculationfunction has been enabled.Calibration or an accuracy check (verification)should be performed.A new disposable filter/mouthpiece mustbe attached for each patient.Room temperature and pressureIdeally, the spirometer should be allowed toacclimatise to the ambient conditions of thetesting environment before use.Some spirometers automatically measure andrecord ambient temperature and barometricpressure, while others require the operatorto enter the data.Patient dataThe patient’s information should be added:— heightiii without shoes (record in cm to onedecimal place)— weight without shoes (record to nearest 0.5 kg)— age (record birth date)— sex at birth— ethnicity (ask patient to identify)— smoking status.Height and weight should be measured every timebefore the test. The operator should not rely ondata provided by the patient.12If the patient has used an inhaled bronchodilatoron the day of the test (or within the recommendedwithholding period), record the dose and timelast taken.Weight is not essential for obtaining thecorrect predicted values, but can be usefulfor interpretation.Record the date of the session.The flows and volumes measured at ambientconditions (i.e. the room temperature andbarometric pressure on the day of the test)are converted to the flow and volume at theconditions within the lungs (i.e. body temperatureand pressure saturated [BTPS] conditions).All electronic spirometers calculate and applythe BTPS correction factor automatically.iii When measuring height the head should be in the Frankfurt Plane – eyes looking straight ahead and in line with the top of the ear.16A guide to performing and interpreting spirometryfor primary care health professionals
Before starting the testing session,the operator should:The spirometry handbook for primary carePreparing the patientto perform the test— explain to the patient that they will need tobreathe in until they have completely filledtheir lungs, then blow out as hard and fast asthey can into the mouthpiece until the lungsare completely empty. This could take a fewseconds longer than feels comfortable.— demonstrate the correct posture and theamount of force needed when exhaling.— explain that this process will be repeatedat least three times, and that several moreattempts may be needed to get reliable results.— advise the patient that doing the test properly(maximal effort) is hard work and theymay become light-headed while blowingout, but they will be given a chance to restbetween attempts. They should stop if theybecome excessively dizzy or if they havesignificant pain.During the test, the operator should provide simple,clear instructions.A guide to performing and interpreting spirometryfor primary care health professionals17
The spirometry handbook for primary carePerformingthe testThe operator must wash their hands before and after the test, and weargloves as needed.Coaching and verbal encouragement during forced exhalation is essentialto achieve maximal effort and complete exhalation.The use of a nose clip is recommended for forced manoeuvres, but is notessential if only performing expiratory manoeuvres.The sitting position is recommended to avoid falling due to syncope.2Reference values are derived from data obtained with spirometry fromseated volunteers. The chair should have arms and not move on the floor.2Upright posture is essential during the test.Closed-circuit method(measuring expiratory and inspiratory flow)Open-circuit method(measuring expiratory flow only)The patient should:The patient should:1. sit upright with their legs uncrossed and theirfeet flat on the floor, without leaning forward1. sit upright with their legs uncrossed and theirfeet flat on the floor, without leaning forward2. place the mouthpiece in their mouth and closetheir lips to form a tight seal2. breathe in rapidly and deeply until their lungsare completely full3. breathe normally for 2–3 breaths3. immediately place the mouthpiece in theirmouth and close their lips to form a tight seal4. breathe in rapidly and deeply until their lungsare completely full5. without pausing for more than 2 seconds,blast air out as hard and fast as possible andfor as long as possible, until their lungs arecompletely empty or they cannot possibly blowout any longeriv4. without pausing for more than 2 seconds,blast air out as hard and fast as possible andfor as long as possible, until their lungs arecompletely empty or they cannot possibly blowout any longer.5. remove the mouthpiece and breathe normally.6. keeping a tight seal on the mouthpiece, breathein again as forcefully and fully as possible7. remove the mouthpiece and breathe normally.iv Under the ATS/ERS 2019 standard2 the spirometry system must signal the operator when a plateau (flow 0.125 litres/min)has been reached or forced expiratory time reaches 15 seconds.18A guide to performing and interpreting spirometryfor primary care health professionals
— meet objective criteria for determining thatmaximal effort was achieved and acceptableFEV1 and/or FVC measurements were obtained(usually termed ‘acceptability’)— meet criteria for consistency across multiplemanoeuvres (usually termed ‘repeatability’).However, occasionally FEV1 or FVC measurementsmay be clinically usable even if they are nottechnically acceptable.2Acceptability of a single manoeuvre (blow)The patient must achieve both maximal inspirationand maximal expiration with a rapid start to themanoeuvre (blow).The operator should visually inspect theperformance of each manoeuvre to check if itmeets acceptability criteria before proceeding withanother manoeuvre.2A manoeuvre is acceptable if:2— it meets criteria for the start of forcedexpiration (see below)Definition of start timeThe start time on the volume–time graph is definedby back-extrapolation from the steepest part ofthe volume–time curve. The line correspondingto this steepest section is extended below thecurve (as though the tracing were linear, notcurved). The point where this line crosses thetime axis is the new time zero (Figure 2).2 Theback-extrapolated volume is the volume at thenew time zero.Most spirometers calculate these valuesautomatically.Figure 2. Back-extrapolation to definethe start time for expirationback-extrapolation lineVolumeSpirometry results are acceptable if the testingsession yields manoeuvres (blows) that:1.0— it meets criteria for the end of forced expirationcriteria (see below)— the operator observed that the patientachieved maximal inhalation and mademaximal expiratory effort— there is no evidence of other faults(see Common faults).A guide to performing and interpreting spirometryfor primary care health professionalsThe spirometry handbook for primary careAcceptability andrepeatabilityextrapolatedvolume00TimezeroTime (seconds)1.019
Figure 3. Rapid versus poor startThe start of the test is acceptable if both of thefollowing are achieved:— the back-extrapolated volume is less than5% of FVC or less than 0.100 L, whicheveris greater— the hesitation time is less than 2 seconds.FlowThe spirometry handbook for primary careCriteria for start of forced expirationPEF should be achieved with a sharp rise andclose to the start of expiration (time zero) onthe displayed flow–volume curve (Figure 3).VolumePoor startRapid startStrong effort by the patient is important for obtaining accurate valu
primary care A guide to performing and interpreting spirometry for primary care health professionals. . Centre, Victoria, and Associate Professor David P Johns PhD, CRFS, FANZSRS, Adjunct Principle . Spirometry Training Program for permission to adapt its interpretation algorithm (Figure 11).