Transcription
Joint Commission Webinar:Safer Pain Assessment andManagement in Acute CareHospitals9-10 am (PT)10-11 am (MT)11 am-12 pm (CT)12-1 pm (ET)January 15, 2019
Safer Pain Assessment and Management in Acute CareHospitalsDuring this session, the following topics will bediscussed: Safer pain management, including non-opioidapproaches (Pain Management Stewardship) Decreasing new chronic opioid starts (Altmedications & non pharmacologic therapy) Treating opioid use disorder (Ensuring continuity) Overdose prevention & naloxone distribution Collaboration with outside community resources2 2018 The Joint Commission. All Rights Reserved.
Safer Pain Assessment and Management in Acute CareHospitalsSlides are available for download now! See the GoToWebinar“Handouts” Section Click the arrow to openthe Handouts list,select the slides fortoday’s session, anddownload.3 2018 The Joint Commission. All Rights Reserved.
Safer Pain Assessment and Management in Acute CareHospitalsThis program is designed to be interactive. All participants are connected inlisten-only mode; we are not usingthe raised hands feature Ask questions through theQuestions function in theDashboard Visit any links or resources notedin the slides Download the slides and sharethe recording4 2018 The Joint Commission. All Rights Reserved.
Safer Pain Assessment and Management in Acute CareHospitals The webinar recording and slide deckfor this session will be accessible onThe Joint Commission website within afew weeks of this session. When they are available, all registrantswill receive an email with the location.5 2018 The Joint Commission. All Rights Reserved.
Safer Pain Assessment and Management in Acute CareHospitalsDisclosure StatementThese staff and speakers have disclosed that neither they nor theirspouses/partners have any financial arrangements or affiliations with corporateorganizations that either provide educational grants to this program or may bereferenced in this activity: Andrew C. Bland, MD, MBA, FAAP, FACP, Medical Director, JointCommission Hannah Snyder, MD, Zuckerberg San Francisco GeneralHospital Casey Grover, MD, Community Hospital of the MontereyPeninsula6 2018 The Joint Commission. All Rights Reserved.
PresentationsDr. GroverDr. Snyder7 2018 The Joint Commission. All Rights Reserved.
Hannah Snyder, MDClinical Assistant ProfessorUCSF at Zuckerberg San Francisco GeneralCo-Principal Investigator, California BridgeProjectCasey Grover, MDChair, Emergency MedicineCommunity Hospital of the Monterey PeninsulaMonterey County Prescribe Safe Initiative
The Opioid EpidemicAn Acute Care ApproachH
Why treating addiction matters Rehabilitate people with addiction “They call it recovery because you get your life back” Prevent overdose deaths, and morbidity from non-fatal overdose Reduce the impact of drug use on the community Infection Costs of health care Assault/accidentsH
H
A three pronged approach Avoid starting patients on chronic opioids for non-terminal conditions Treat addiction when present Prevent overdoseC
Avoid new chronic opioid startsC
A Case Study: Joseph Joseph was an 18 year old male bullrider in Salinas, CA He injured his ribs at age 18, and was prescribed Norco After several weeks of Norco, the Norco stopped working and he was“upgraded” to Percocet Six weeks after his injury, Joseph was told that his ribs were cured andthat he no longer needed his medications, and his prescription endedC
Improving pain management withoutusing opioids Doctors do the right thing when it’s easyC
Less expensive optionsC
Improving pain management withoutusing opioids Options for the Emergency Department IV lidocaineIV ketamineNitrous oxideTopical non-opioid medicationsNerve blocksOsteopathic manipulative medicinePhysical therapyTENS units Multi-modal therapy is great!C
C
Reducing the number of pills given Prescribing for surgeons Engaging the dentistsC
Nuances of Chronic Opioids Some situations are higher risk 90 MME Coprescribed benzos Prior overdose, use disorder Risks of discontinuation Key is preventing startC
Treat Addiction When PresentC
The Case Continues: Joseph The prescriber overlooked the fact that Joseph had been on opioidsfor several weeks, and the inevitability of withdrawal Joseph, suffering withdrawal, sought additional pain prescriptions Multiple ER visits to try to obtain opiates Eventually he found that heroin was easier to getC
OUD Impacts HospitalsH
OUD Complicates InpatientTreatment 25-30% of admitted patients leave AMA Craving Fear of mistreatment Financial and social pressures Withdrawal Reduced adherence Increased readmissionH
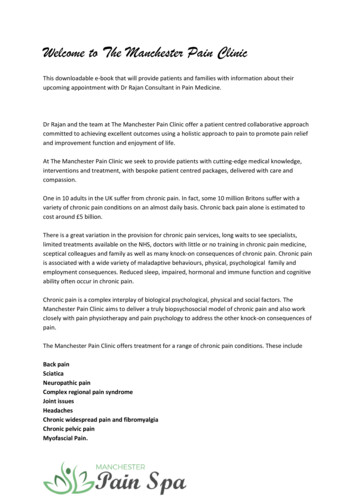
Drug Related Death Rateper 1000 Post Discharge40.31.730.20.10.0.14.92No hospital admission28 days after dischargeH10.61-3 months3 months-1 year
Detox Doesn’t LastHChutuape, M et al. One-, three-, and six-month outcomes after brief inpatient opioid detoxification. The American Journal of Drug and Alcohol Abuse. Vol 27:1, 2001.
Medication Addiction Treatment:Buprenorphine & Methadone Eliminate withdrawal Reduce cravings If a slip happens, don’t feel effects Proper dosing no euphoria, no sedation Physical dependence without addictionH
Prevents Morbidity, Promotes Recovery Reduce injection and illicit drug use Reduce HIV and HCV transmission Reduce bacterial infections Reduce criminal behavior Promotes return to work and familyobligationsH
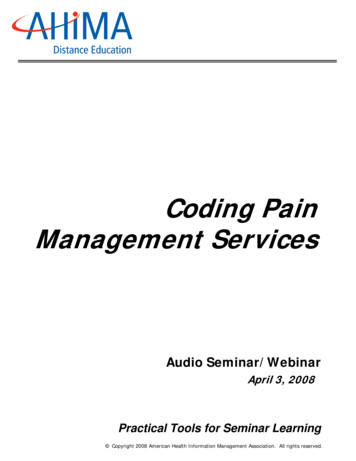
Decreased MortalityAll cause mortality per 1000 person years40.30.20.10.0.In methadoneOut of methadoneIn buprenorphineOut of buprenorphineHSordo Luis, Barrio Gregorio, Bravo Maria J, Indave B Iciar, Degenhardt Louisa, Wiessing Lucas et al. Mortality risk during and after opioid substitution treatment: systematicreview and meta-analysis of cohort studies BMJ 2017; 357 :j1550
Methadone vs. Buprenorphine Methadone Full opioid agonist Long half life Only available in specialty clinic Buprenorphine Partial opioid agonist Ceiling effect on sedation, respiratory depression Available from any provider with X waiverH
Treatment Starts HereAcute Care Medication TreatmentH
Why Start in the ED? Treating emergency ofwithdrawal Frequent site of care forpatients with OUD Often otherwise not engagedin care May be requesting help Buprenorphine onlyH
ED Initiation of Buprenorphine% in care at 30 daysDays illicit opioid use/weekBriefinterventionBrief hine020406080100H00.511.522.53
Why Start in the Hospital? 67% of hospitalized people who use drugs state that they wouldlike to cut back or quit Fear of bad outcomes Forced abstinence allows time for thinking Respect and kindness from providers Treat withdrawal, prevent AMA, linking to care Often not seeking help Methadone or buprenorphineEnglander et al. J Hosp Med. 2017 May; 12(5): 339–342H
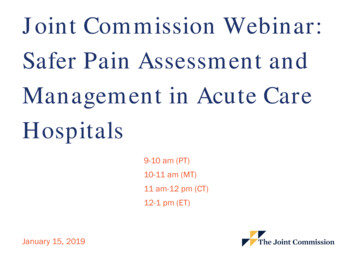
Hospital Initiation of Buprenorphine% Patients6072Detox806570605040200403012Received MAT in 6 mo afterdischarge7Days in MAT over 6 monthsLiebschutz et al. Buprenorphine Treatment for Hospitalized, Opioid-Dependent Patients. JAMA Intern Med. 2014 Aug; 174(8): 1369–1376.H20100Number of Days80Linkage
The Case Continues: Joseph Joseph continued to use heroin for SIX YEARS, stating that he couldnot tolerate opiate withdrawal His words “It wasn’t about getting high, I just didn’t want to get sick”C
The Case Continues: Joseph Issues for Joseph that made getting treatment so challenging: Joseph is from a rural county that did not have a treatment program He was treated as “one of those people with addiction” when seeking care inEmergency Departments He ultimately was referred for treatment in a neighboring county, where hewas treated with MAT He has been been sober since, and spoke as an expert about opiateaddiction with me at town halls and medical Grand RoundsC
Making it HappenBreaking down barriersH
DEA Regulations If patient is admitted for a medical or surgical reasonother than opioid dependency: Methadone and buprenorphine can be administeredto maintain or detoxify Including new starts If the patient presents to ED or urgent care inwithdrawal: Legal to administer 72 hours of methadone orbuprenorphine to treat withdrawal On discharge, regular rules applyH
Acute Care g:Obstetrics:Clinical Lead(phone), t)Emergency Department:Clinical Lead (phone), Trained ProvidersHBridge NavigatorPsychiatry:
Acute Care Structure—Unfunded Buprenorphine and methadone on formulary Hospital orderset or guideline Agreement with community clinic Start prescribing!H
Early Success: Rural EDMarshall Medical CenterPlacerville, CA Unfunded, no linkage navigator Standing appointment slots at local FQHC 35 out of the 38 patients presented to the clinic in follow-up for treatment Out of the 35 patients to follow-up, 26 are still in treatment68% patients are still in treatmentH
Early Success: Urban EDHighland HospitalOakland, CA Linkage navigator, on site bridge clinic 209 patients contacted in ED by navigator 110 patients received buprenorphine 90 patients linked to care82% linked to careH
Prevent Overdose DeathsH
Worst Case ScenarioReturn to use after methadone/buprenorphine Death rate is likely reduced because tolerance has not been lost Prior quit attempts predict future success Positive experience with the health care system—connectionsmatterH
Stop Overdose Deaths Universal naloxone prescribing Opioid use disorder Chronic opioids (esp 90 MME,coprescribed benzos) Any illicit drugs Partner with local syringeexchange/harm reductionH
Naloxone Evidence Does it get used? San Francisco Distribution: 1942 trained individuals, 331 successful reversalsDoes it work? Meta-Analysis: bystander administered naloxone odds of survivingincrease 8x San Francisco Primary Care: patients who received naloxone 63% fewer EDvisits in next yearH
Naloxone Payment Often covered by insurance, including MediCare and MediCaid If insured, 76% have copay of 10 for intranasal Available without a prescription from pharmacist—but costly Intranasal can be expensive—can use atomizer, injectionwww.prescribetoprevent.orgH
C
Key Points Avoid starting patients on opioids for non-terminalconditions Treat addiction when present Prevent overdoseC
The California Bridge Project In California: Clinician champions, linkage navigators, bridge clinics Statewide trainings, site visits, grand rounds National: Guidelines, ordersets, P&T monographs, etc Inpatient, ED, OBH
Office hours 3 days a ridge.org
The Substance Use Warmline Monday-Friday, 9am-8pm ET (855) 300-3595 ance-usemanagement/H
rgC
Safer Pain Assessment and Management in AcuteCare Hospitals Please submit questionsnow. Click the arrow next to“Questions” in the righthand navigation to expandthe Questions pane. Include your name andorganization with yourquestion.8 2018 The Joint Commission. All Rights Reserved.
Safer Pain Assessment and Management in Acute CareHospitalsReminder – Slides are available for download now! See the GoToWebinar“Handouts” Section Click the arrow to openthe Handouts list,select the slides fortoday’s session, anddownload.9 2018 The Joint Commission. All Rights Reserved.
Unanswered Questions We will review all unansweredquestions and draft a Q&Adocument for this session.10 2018 The Joint Commission. All Rights Reserved.
Safer Pain Assessment and Management in Acute CareHospitalsAdditional Resources https://www.jointcommission.org/webinar establishing an opioid stewardship program in your health system october 10 2018/11 2018 The Joint Commission. All Rights Reserved.
Safer Pain Assessment and Management in Acute CareHospitalsSession Evaluation SurveyPlease click on the survey link as youexit GoToWebinar or in the automatedemail you will receive tomorrow. Youwill be directed to an evaluation survey.We use your feedback to inform futurecontent and assess the quality of oursessions.12 2018 The Joint Commission. All Rights Reserved.
Safer Pain Assessment and Management in Acute CareHospitalsThank you for attending this session.13 2018 The Joint Commission. All Rights Reserved.
In methadone Out of methadone In buprenorphine Out of buprenorphine All cause mortality per 1000 person years. H. Sordo Luis, Barrio Gregorio, Bravo Maria J, IndaveB Iciar, Degenhardt Louisa, Wiessing Lucas et al. Mortality risk during and after opioid substitution treatment: systematic review and meta-analysis of cohort studies . BMJ . 2017 .