Transcription
Preceptor Barriers and MotivatorsAnna Jarrett, Marilou Shreve, Audrey WeymillerUniversity of Arkansas Eleanor Mann School of NursingFayetteville, AR United State of AmericaAbstractPreceptors for doctor of nursing practicestudents (DNP) are essential for student andp r o g r a m success. In order to learn the clinicalrole, DNP students m u s t have qualifiedpreceptors. In the United States, students mustcompete with students from multiple programs tosecure their preceptor(s). It is important tounderstand why preceptors agree to do this withoutpay. In order to more efficiently assist studentrecruit preceptors, the Enlisting New Teachers inClinical Environments (ENTICE) survey was usedto discover barrier and motivators for being apreceptor.A beginning and advanced clinicc o u r s e w e r e selected for baseline data in 2015,and compared with 2016 preceptor responses. Next,surveys were compared by student cohortslongitudinally across courses. In these groups ofpreceptorsacrosscoursesandacrossc o h o r t s , ‘giving back to the profession’remained the most important reason thesepreceptors chose to teach students in the clinicalarena while practicing their skills. The mostsignificant barrier for preceptors in both years forboth courses and for preceptors in Cohort 1 a n d 2across courses was ‘decreased productivity’. The‘type of student’ was also important. Thes o l u t i o n to this problem may be ionaleducation,online learningopportunities, standardized student pre-clinicalcompetency validation, and negotiating professionalentrustable acts.1. IntroductionAs the shortage of medical providers increase, thenumber of nurse practitioner students enteringdoctoral level programs also increase.Preceptors for doctorate of nursing practice (DNP)students play a vital role in the education of the nextgeneration of providers [1]. Many providers decide tobe preceptors for DNP students to give back to theirprofession. Preceptors are committed to their role ineducating future practitioners and want the preceptorprocess to be legitimized and recognized by employersand facilities [2]. Preceptors find support from nurseeducators to assist in increasing their awareness andconfidence of the preceptor role.2. Literature ReviewA preceptor is one who teaches, supports, counsels,coaches, evaluates, serves as a role model, and socializesDNP students to their new role as a provider. The roleis essential to help the student assimilate academicknowing into the real work of practice. Students havethe luxury of being a learner by a 1:1 relationship with apracticing provider. It allows time for the student to gainconfidence while perfecting t h e i r a d v a n c e d s k i l l s .Being a good preceptor requires someone who iscompetent in practice and someone who canintuitivelyshift betweencoaching,mentoring,teaching, and role modeling. Students’ objectives foradvanced practice nursing i n c l i n i c a l s e t t i n g s , thefocus is on attainment of pre- determined skill setsappropriate for one’s area of specialty. For example,family nurse practitioners learn skills with patientsacross the lifespan, but adultgeriatricnursepractitioners do not learn specialty skills for pediatricpopulations.In 2015, The University of Arkansas Eleanor MannSchool of Nursing was awarded an Advanced NursingEducation g r a n t supported by the Health Resourcesand Services Administration (HRSA) of the U.S.Department of Health and Human Services (HHS) toimprove the preceptor/student/faculty process.109
This project called, “Mutually Beneficial ClinicalPartnerships” had three major goals with methodsto measure outcomes. One goal was to evaluatethe clinical preceptor process. The instrument wasselected after a careful review of the literature insearch of reliable and valid instruments to measurestudent, preceptor and faculty satisfaction. It wasdiscovered that students evaluate preceptors, facultyevaluate preceptors, and preceptors evaluatestudents, but the only instrument that ‘got at’ thereason preceptors agree to become preceptors wasthe Enlisting New Teachers in ClinicalEnvironments (ENTICE): novel ways to engageclinicians[3].ENTICE was a survey created and piloted byresearchers at Duke University in collaboration withthe Veterans’ Affairs Medical Center located inDurham, North Carolina in 2013 and was pilotedand published in 2014. This group studied incentivesand barriers to being a preceptor for medicalstudents assigned to primary care [3]. However,studies have not examined barriers and motivationfor preceptors working with graduate nursingstudents. From an exhaustive review of literatureand under the guidance of collaborators withexpertise developing surveys, the collaborative teamconstructed a survey comprised of six demographicquestions. Seven questions aimed to determine pastexperience as a preceptor and seven “lookingforward” questions were developed to discoverfuture willingness to precept students.One key question in this area asked preceptors torank from 1 MOST significant to 5 LEASTsignificant barriers to being a preceptor. From theliterature review the following options were given:a) Decreased productivity as a result oftime required to teach studentsb) Inability of learner to write clinic notes inthe electronic medical record due toInstitutional protected healthinformation policiesc) Lack of institution, department,professional recognition for teachingd) Lack of physical spacee) Lack of support among office clinicalcolleaguesf) Lack of teaching skillsg) Patients prefer to see provider withoutstudentsh) Time to teach results in longer work daysi) Type of learner (i.e., MD/NP/PA) determineswillingness to preceptj) OtherBoth survey questions gave an option for ‘other’in order to allow participants to give additional inputor different reasons. The second question was posedsimilarly with 1 MOST significant to 5 LEASTsignificant incentives to being a preceptor. Thefollowing options were given:a)b)c)d)e)f)g)h)i)j)k)Access to online training modulesAdjusted appointment times toincorporate feedback to learnerCertificate or plaque of appreciationfrom facility or academic institutionEnhanced employee benefit packageFaculty appointment with affiliatedacademic departmentMonetary compensationParking passesProtected time to attend preceptoreducationReduced productivity expectations (i.e.,reduced encounters, RVUs)It allows one to give back to professionOtherIn 2013, 180 providers were sent the 20-questionsurvey. The response rate was 50%, with 65% ofthose participants indicating they planned to be apreceptor within the next six months. The overallfindings of this study found time pressure andproductivity demands were the most importantbarriers to being a preceptor [1].Interprofessional education aims to utilizemembers of different professions to learn together,with each other and about each other [4].Standardized assessments are national certificationexaminations taken by students after 500 hours ofclinical practice experiences in the DNP program.DNP students do not receive certification until theygraduate from the DNP program, but they have thecomfort of knowing they meet national minimumrequirements for advanced practice nursing.Competency assessments for students areadministered throughout the program after a skillslaboratory experience. In addition, faculty, andstudents participate in DNP orientation. Facultyme mb e r s provide evaluation oversight and indirectsupervision for DNP students.In 2016, the National Organization for NursePractitioner Faculty (NONPF) and the AmericanAssociation of Colleges of Nursing (AACN) created ajoint National Task Force on Quality NursePractitioner Education whoexaminedcorecompetencies for preceptors.110
These two powerful organizations within this jointtask force for advanced practice nursing addedCriterion IV.B.3.c., which states that preceptors areoriented to program/track requirements andexpectations for oversight and evaluation of NursePractitioner Students. Nursing programs in theUnited States who are accredited institutions must puta mechanism in place to that requires preceptors tohave an orientation to the program where theyprecept prior to being approved as a preceptor [6].Specific preceptor competencies were developedusingthe2016 Interprofessional EducationCollaborativeCore Competencies [4]. Thecompetencies were developed around the four generalcompetencies and sub-competencies sequesteredaround values/ethics for interprofessional practice andcommunication, roles and responsibilities, andteams/teamwork. This is available and distributed tonew preceptors at the time they agree to work as apreceptor (see Table 1).Table 1. DNP preceptor competenciesDNP PRECEPTOR COMPETENCIES1. Maintains skills, certification licensure and uses current practice guidelines as an indicator of competence.2. Conveys one’s limitations in skills, knowledge, and abilities to student and clinical co-preceptor.3. Ensures that student respects the dignity and privacy of patients while maintaining confidentiality.4. Uses knowledge, skills, and abilities of available health professionals and healthcare workers to providecare that is safe, timely, efficient, effective, and equitable.5. Maintains a climate of mutual respect and shared values with student and other professions.6. Prioritizes interests of patients and populations central to interprofessional health care delivery.7. Role models leadership embracing cultural diversity and individual differences to establish a high standardof ethical conduct toward student, patients, families, and other collaborative team members.8. Communicates with student, patients, families, communities, and other health professionals in aresponsive and responsible manner that supports a team approach to maintenance of health and treatmentof disease.9. Explains roles and responsibilities of care providers and how the team works together to execute a treatmentplan.10. Engages self and student to constructively manage disagreements about values, roles, goals, and actionsthat arise among healthcare professionals and with patients and families.11. Encourages student to express knowledge to team members involved in patient care with confidence,clarity, and respect, and work to ensure understanding of information, treatment & care decisions.12. Engages in continuous development and process improvement strategies to increaseeffectiveness of interprofessional teamwork and to enhance team performance appropriate tospecific care situations.13. Provides timely, sensitive, instructive feedback to student and clinical co-preceptor (faculty)about student’s performance.14. Other site specific or skill specific competency111
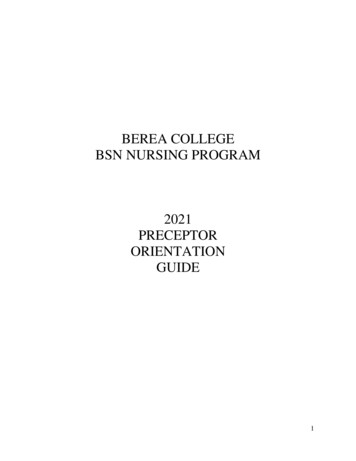
In addition, new preceptors are expected tocomplete an online preceptor orientation coursewhich introduces them to academic expectations,course outcomes, and the evaluation process. As offall 2017, in order to be approved as a preceptor,they must take the online course and pass with atleast 80%. To date, only one preceptor had to repeatthe course. It is construction in three short modules.The first model introduces the Clinical Co-PreceptorModel which aims to improve preceptor, student,and faculty communication. This model incorporatesentrustable professional acts, standardized studentassessment, interprofessional education, andinnovative education practices as outcomes forgraduate doctor of nursing practice (DNP) students[5]. See figure 1.Figure 1. Co-Preceptor modelAs part of program evaluation, the ENTICEsurvey was selected to be administered to currentpreceptors for graduate nursing students acrosscohorts over a 3-year period of time (2015 – 2018).Results are collected, analyzed and disseminated tograduate nursing faculty at the end of eachsemester.Because this instrument was originally designed formedical students, phrases indicating medical studentswere substituted with nurse practitioner and clinicalnurse specialist students. The original study did notattempt to establish initial reliability and validity.112
In addition, because this pilot study has a small n foreach cohort, establishing reliability using measures ofinternal consistency or repeated measures was notcalculated. The original class sizes were small with amean class size of eight students across cohorts, butas the program grows it may be possible to establishinternal consistency of this instrument.Usability was determined by four individualpreceptors’ feedback in a face-to-face meeting attwo institutions. All four preceptors indicated thesurvey was easy to understand and straightforward.They had no additions to either barriers ormotivators.Face and content validity was established by fourfaculty members who have had at least five years’experience in academic teaching, preceptorship, andclinical practice. There was 100% consensus thatitems listed regarding barriers were correct andcomplete. There was 75% consensus among theseexperts about motivators for preceptors. One expertfelt faculty appointment with affiliated academicdepartment should be omitted because it was notpossible to offer this incentive by the academicinstitution per policy.At the end of the first year, responses ofpreceptors for an advanced and beginner clinicalcourse were described and compared. The ENTICEsurvey and study was used with permission andapproved through University IRB and completed bypreceptors for a family nurse practitioner program atthe end of each clinical course. The first and lastclinical skills courses are compared.3. Baseline Advanced course (AC) 2015There were 4 of 7 (57%) preceptors responding tothe initial ENTICE survey. Three preceptors wereAPRNs; 50% were in a specialty practice, 25% inhospitalist roles. The age span was 28 - 49 years ofage; 75% were Caucasian; one preceptor was AfricanAmerican. There was a wide disparity in number ofyears as a preceptor; 50% stated less than one year;50% reported 14-17 years. Surprisingly, 75% reportedthey felt the ideal number of months to be a preceptorwas 5-6 months/year, but only 50% felt they wouldbe a preceptor in the next six months.In addition to basic and specific demographics, thesurvey consisted of two domains: 1) potentialbarriers to decide not to be a preceptor and 2) reasonsone would begin or continue to be a preceptor.Preceptors were asked about potential barriers in theirdecision to consider to precept NP/CNS students andto rank the top 5 reasons why they would not preceptthe students. Responses were ranked as 1 mostsignificant barrier, 2 second most significantbarrier, 3 third most significant barrier, 4 fourthmost significant barrier and 5 least significantbarrier.Decreased productivity of the preceptor(decreased visit volume and RVUs) and the type ofstudent (level of nursing practice, i.e., baccalaureate,masters or doctoral nursing student) tied with a meanscore of 2.5. For these preceptors, this was asignificant barrier and would determine if they wouldcontinue to be a preceptor. The least potentialbarriers included the inability of student to write aclinical note in the electronic health/medical records(M 4.25), lack of department/professionalrecognition for teaching/being a preceptor (M 4.25), lack of physical space (i.e., not enough examrooms) (M 5), and patients prefer to see theprovider without students (M 4.5).Reasons why preceptors were consideringstarting or continuing as a preceptor were posed. Thesame rating scale 1-5 above was used with 1 mostsignificant incentive and 5 least significantincentive. The choices listed for reasons to considerinclude: access to online training modules withCME/Contract hours for provider, adjustedappointment times to incorporate time for feedback tostudent, certificate or plaque of appreciation frominstitution/department, enhances employee benefitpackage, faculty appointment with affiliatedacademic department, monetary compensation,parking passes for school of nursing access forrelated obligations, protected time to attend preceptorspecific workshops or educational sessions, reducedproductivity expectations (i.e., reduction inencounters, visit volume, or RVUs), teaching/beinga preceptor gives the preceptor the opportunity togive something back to the profession.The most significant reason by the preceptors toconsider beginning or continuing to precept is accessto online training modules with continuingeducation/contact hours for providers (M 2.5).Adjustment in appointment times to incorporate timefor feedback to students, monetary compensation, andteaching and being a preceptor give the preceptor theopportunity to give something back to the profession113
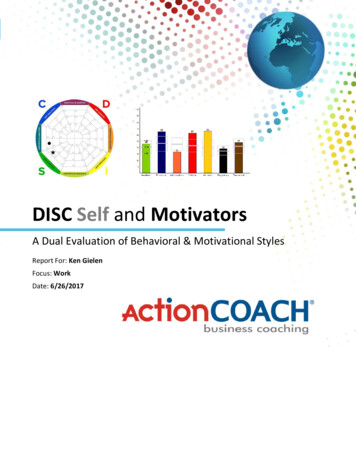
scored second highest (M 2.75). The leastsignificant reason (M 5.0) was parking passesfor campus related obligations.4. Baseline Beginner class (BC) 2015There were 6 of 6 (100 %) preceptorsresponding to the initial ENTICE survey. Fivepreceptors were APRNs; 50% were in familypractice, with 33% in hospitalist roles. The agespan was 44-55 years of age; all six were Caucasian.There was a wide spread in number of years as apreceptor; 50% states less than one year; 25%reported 6-9 years, and 25% had been a preceptorfor 14-17 years. 50% reported they felt the idealnumber of months to be a preceptor was 5-6months/year, and 50% felt they would be apreceptor in the next six months.Decreasing the productivity of the preceptor(decreased visit volume and RVUs) scored low (M 2.33) on a reverse scaled question, which made itthe most significant barrier for these preceptors.Two other selected barriers to being a preceptorfor this course were lack of recognition (departmentand professional) and lack of teaching/preceptorskills (M 3.81). The least potential barriers included lackof physical space (i.e., not enough exam rooms),length of clinical rotation/ hours, and lack ofsupport among office clinical colleagues. (M 4.67). The type of student and teaching/being apreceptor requires an inordinate amount of timewhich results in longer work days were notparticularly significant for this group of preceptors(M 4.17).The most significant reason selected by thepreceptors to consider beginning or continuing topreceptor based teaching/being a preceptor gives thepreceptor the opportunity to give something backto the profession (M 1.83), followed byfaculty appointment with affiliated academicdepartment and access to online training moduleswith continuing education/contact hours forproviders (M 2.83). A desire for adjustedappointment times (M 3.33), and monetarycompensation,certificate o r p l a q u e o fappreciation from institution/department did notseem particularly important to this group ofpreceptors (M 4.0). Teaching and being apreceptor gave the preceptor the opportunity to givesomething back to the profession was a highpriority (M 2.75) for this group. The leastsignificant reason was having parking passes atschool for related obligations (M 4.17).5. FindingsThere was general consensus among thepreceptors from both clinical courses. Overall, thebiggest barrier to being a preceptor wasdecreasing the preceptor’s productivity, whichmay have a financial impact on the preceptor inthe form of reimbursement, b o n u s e s , a n d /ora n n u a l r a i s e s ( M 2.5, 2.33). The two moststated reasons for continuing t o p r e c e p t fromthe groups of current preceptors were to give backto profession (M 2.75, 1.83) and access to onlinecontinuing education with continuing educationor contact hours (M 2.50, 2.83).6. 2015 and 2016 (AC) Preceptor ResponsesResults were analyzed by cohorts once twogroups had completed and evaluated the samecourse for two data points. The same courses wereanalyzed. First, the advance clinical course NURS6244 was compared to the previous year’s findings.Preceptors were not the same individuals, nor werestudents. For the second cohort in 2016 in the sameadvanced course, type of student was the mostsignificant barrier preceptors identified (M 2.00). However, decreased productivity was mostsignificant for the first cohort in this course (M 2.50). The least significant continues to be lack ofphysical space, which speaks well for the clinicalenvironment in which preceptors and studentspractice(M 5.00).See figure 2.Figure 2. 2015 vs. 2016 AC barriersMean scores for all items increased from theadvance course 3.84 to 4.09 from the first andsecond cohorts, which may imply overall lesssignificance to114
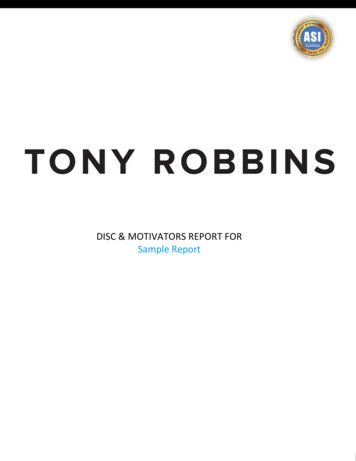
most variables. This may also represent continuedexperience of the preceptors to teach the same courseeach year.Unexpectedly,themosts i g n i f i c a n t motivator for preceptors in thesecond cohort was access to training (M 2.50), butfor the first cohort it was to give back to the profession(M 1.50). The least significant motivator wasparking passes for both cohorts (M 5.0), butreduced productivity and adjusted appointment timeswere less significant to the second cohort, perhapsbecause they are more experienced students, or thetype of clinic and preceptor could possibly accountfor this change (see Figure 3).Figure 3. 2015 vs. 2016 AC motivators7. 2015 and 2016 (BC) Preceptor ResponsesCumulative means across all data points for 20152016 beginner practitioner course show thedecreased productivity on the part of the preceptorswas the most significant barrier (M 2.33, 1.60).Longer work days was the next most significantbarrier for the second cohort (M 3.00). Theremaining variables for both cohorts fell within arange 3.80 – 4.40, which were closer to the high endof the scale, indicating they were not as significant toeither group (see Figure 4).Figure 4. 2015 vs. 2016 BC barriersSignificant motivators across the cohorts in thebeginning clinical course were to give back tothe profession (M 2.70, 1.83) and adjustedappointment times (M 3.50, 3.33). Again,parking passes were not particularly significant (M 5.00, 4.17).A new motivator, Facultyappointments as adjunct faculty became more important with the second cohortduring the second year (M 4.50, 2.83). Parkingpasses (M 5.00, 4/17) and recognition w it h certificate o r p l a q u e ( M 5 . 0 0 , 4 . 0 0 ) was l e s s significant to both groups (see Figure 5).Figure 5. 2015 vs. 2016 BC motivators8. Preceptor Barriers (PB) Across CohortsAfter enough longitudinal data had y submitted to preceptors over theperiod of time from fall 2015 until the beginningof fall 2017, surveys were extracted from the datasource and compared across cohorts.Cohort 1 consisted of students who entered thebeginning clinical course spring 2016 and whohad completed five clinical courses. A goal ofthe Advanced Nursing Education grant was toencourage students to select clinical placements inrural and underserved clinics and facilities and toparticipate in an emersion experience, whichentailed staying in the same site and for mostsemesters to remain with the same preceptor. It isnot possible to match preceptors with courses todetermine if this was the same preceptors, due toIRB restriction of complete anonymity of theparticipants.There were a total of 38 preceptors respondingfor cohort 1 across all courses completed to date,w i t h a range of group mean scores between 2.95and 4.36. Preceptors were115
asked to complete the survey with score of 1 being themost significant, and progressing to 5 being the least significant barrier. Consistent with comparisonsbetween beginner and advanced courses, decreasedproductivity was the most significant barrier to beinga preceptor for this cohort, regardless of where thestudent was in the progression of courses. Responserates appeared to increase over time. The range ofresponses were 26.3% to 69.2%. This can beattributed to preceptors becoming aware of end-ofcourse expectations regarding survey completions. Inaddition to this voluntary survey, p receptors mustcomplete two additional required surveys. Consistentwith previous findings, altruism is evident in theleast significant barrier to being a preceptor acrosscourses was ‘lack of recognition’ (see Figure 6).There were a total of 25 preceptors responding forcohort 2 across courses with a range of group meanscores between 2.96 and 4.44, which comparesclosely with Cohort 1 preceptors. Decreasedproductivity was the most significant barrier tobeing a preceptor for this cohort, and once again,lack of recognition was the least significant barrieraccording to this group of preceptors.This may indicate that the same preceptors were usedfor some students in both cohorts. Students discussquality preceptors and make recommendations tonewer cohorts to direct them in a qualityexperience. Altruistic reasons for being a preceptorcontinues to ring true, with the least significant barrierto being a preceptor across courses were ‘lack ofrecognition’ (see Figure 7).Figure 7. PM Cohort 2 across coursesFigure 6. PB Cohort 1 across coursesCohort 2 consisted of preceptor responses aslongitudinal data collected over the period of timefrom fall 2016 until the beginning of fall 2017. Endof-semester surveys were extracted from the datasource and compared across courses for this cohortas well. Cohort 2 consisted of students who enteredthe first clinical course fall 2016 and who hadcompleted four clinical courses. These students andpreceptors were well versed in the goals of theAdvanced Nursing Education grant and hadembraced emersion experiences.9. Preceptor Motivators (PM) AcrossCohortsResponse rates also increased over time. The rangeof responses were 26.1% to 70.1%. This increase forsecond cohort is likely to be attributable to increasedawareness of the role of preceptors.Using the same procedure for barriers, preceptormotivators were examined across both cohort 1 and2. The scale used reflected 1 as being the mostsignificant, moving to 5 as the least significantmotivator for being a preceptor. Cohort 1 preceptorswere consistent with previous data with the mostsignificant motivator being, ‘to give back to theprofession’. The range of scores were 2.53 to 4.58,with an overall mean score 3.84 (see Figure 8).116
motivators between Cohort 1 and Cohort 2 acrosscourses.10. DiscussionFigure 8. PM Cohort 1 across coursesCohort 2 preceptors had a range of 2.9 - 4.73,with an overall mean score 4.11. These responseswere also consistent with previous baseline data,comparative data between beginning andadvanced courses, and across two cohorts (seeFigure 9).Figure 9. PB Cohort 2 across coursesA one-way between subjects ANOVA wasconducted to compare the effect of cohorts onpreceptor responses. There was no significant effectof cohorts on barriers of being a preceptor at p .05level for three conditions: between groups, withingroups, or total [F (1, 18) 4.41, p 0.68], indicatingstable responses by preceptors between Cohort 1and Cohort 2 across courses.A one-way between subjects ANOVA wasconducted to compare the effect of cohorts onpreceptor responses for motivators. There was nosignificant effect of cohorts on motivators for beinga preceptor at p .05 level for three conditions. [F(1, 20) 4.35, p 0.64], indicating stable responsesby preceptors about barriers andThere appears to be only slight shifts in the toppreceptor barriers and motivators to being apreceptor for DNP students. In these preceptors, inadvanced and beginner courses in 2015 and 2016and in preceptors as they progressed with studentsacross courses in Cohort 1 and Cohort 2, givingback to the profession which is a motivator thatreflects a high degree of professionalism altruismremained the most important reason these preceptorschoose to teach students in the clinical arena whiledoing practicing their skills. A significant barrierfor preceptors in both years for both courses and inboth cohorts longitudinally across courses wasdecreased productivity. The ‘type of student’ wasalso important. Additionally, creating mechanismsto provide continuing education credits forpreceptors may be helpful as a recruitment andretention strategy. This seems logical, becausepractice environments contain productivity and timepressures that equate to monetary reimbursement forpreceptors.One trend that draws particular attention to ourfaculty is that the length of clinical rotations and thenumber of hours a preceptor is expected to have astudent has risen in rank among the barriers to beinga preceptor. Between the first and second cohort,the co-preceptor model has been more fullyimplemented in our clinical sites. The model whenfully implemented calls for an “immersive clinicalexperience.” This reflects a fundamental increase inthe number of hours any one preceptor would beexpected to precept any one student as students staywithin one clinical site. Previously students wouldrotate clinical sites with each clinical course. Furtherattention to mechanisms to provide continuingeducation credits is also warranted.This study will continue to be administered at theend of the spring 2018 semester so strongrelationships between beginning and advancedcourses as well as between student cohorts acrosscourses may be established.Results of the ENTICE survey will continue tobe collected and analyzed by cohorts and bycourses. The survey is approved through theUniversity of Arkansas IRB to be administered117
anonymously, so it will not be possible to identifyindividual preceptor responses to determine howtheir responses change or remain stable over time.However, dissemination of the group data will bebeneficial to nursing programs at all levels who usepreceptors to aid students to learn the role of thedegree/certification which they aspire to gain.preceptors. I will be able to help students matchtheir clinical experiences with consistently excellentpreceptors, and I will be able to assist preceptors toagree to act as preceptor to strong, highly skilledDNP students.”11. Case Report: Application of FindingsPreceptors agree to teach, coach, and mentorDNP
In 2015, The University of Arkansas Eleanor Mann School of Nursing was awarded an Advanced Nursing Education g r a n t supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) to improve the preceptor/student/faculty process. 109