Transcription
CltiBE AWARE & TAKE CARE:Talk to your pharmacist!C A L I F O R N IA S TAT E B OA R D O F P H A R M A C YSummer 2016Board of Pharmacy Launches Redesigned Website'/\'etcom. to e Califse Boa0 ' PhrrnacvIn This IssueThe Board of Pharmacy has a newlook online! The redesigned website waslaunched in June with a clean layout anduser-friendly tools for finding news andinformation about the board as well aslinks to other agencies and organizations.The home page features new tabsto access the Consumers, Applicants,Licensees and About Us landing pages.A search box in the top right corner takesvisitors to specific topics quickly. Aspecial new feature provided by Googlecan now translate the full site into almost100 different languages.Board members Deborah Vealeand Dr. Ramón Castellblanch workedwith webmaster Victor Perez to developthe new design. Check it out at www.pharmacy.ca.gov.Board of Pharmacy Launches Redesigned Website.Front PagePresident’s Message.Page 2Upcoming Board and Committee Meetings .Page 3Pharmacists Expanding Public Access to Naloxone .Page 4Experts Warn Opioid Abusers Turning to Loperamide .Page 5Notice to Consumers Available in Print, Video Formats.Page 5Accessible Labels for Blind, Visually Impaired, Elderly .Page 6Valerie Muñoz Appointed to Board.Page 7Ramón Castellblanch Leaves the Board .Page 7NABP Honors Stan Weisser for Distinguished Service.Page 7Board Re-elects All 3 Officers .Page 7Did You Know?.Page 8Board Honors Pharmacists Active for 50 Years.Page 8New Master Formula Document Requirements.Page 9Preparing for Sterile Compounding Inspection .Page 10Explanation of Disciplinary Terms .Page 11Disciplinary Actions .Page 11
Summer 2016BOARD OF PHARMACY2regulations creating stateprotocols so that pharmacists may provide nicotinereplacement products andself-administered hormonalcontraception to patientsunder their own authority.Regulations were recentlyapproved that provide pharmacists with greater autonomy to vaccinate patientsunder the education andskills they have obtainedas licensed pharmacistsunder the state protocol. Inaddition, the first of two advanced practice pharmacist(APP) regulations was alsorecently approved, pavingthe way for communitybased pharmacist trainingas a route for APP qualification.patient-specific prescription dispensing history for Schedule II-IVdrugs from all California-licensedpharmacies. This access helps identify patients at risk and is a criticaltool for pharmacists who dispensecontrolled substance prescriptions.President’s MessageBy Amy Gutierrez, PharmDPresident, Board of PharmacyDrug overdoses have becomeone of the leading causes of accidental death in the United States,with opioid addiction driving thisepidemic. According to the CDC,over 259 million prescriptions werewritten for opioids in 2012 - morethan enough to give every American his or her own bottle of pills.Earlier this year, the CDC issued new prescribing guidelinesfor the use of opioids in chronicpain, focusing on the use of nonopioid therapy for chronic pain andpromoting the use of lower opioidtreatment doses to reduce risk. Aspharmacists, we play an importantrole in promoting the safe prescribing of opioids and promotingcommunication to the healthcarecommunity and our patients of theinherent risks associated with thelong-term use of opioids.One of the available tools toidentify patients who may be at riskis California’s prescription drugmonitoring program - CURES. TheCURES system is readily available to all pharmacists who haveregistered, allowing for review ofRecent legislation required thatall pharmacists with active licensesapply for registration in CURESby July 1, 2016. Through statewideefforts to maximize awareness,education and active participationby pharmacists, almost 95 percentof all California licensed pharmacists were registered to access theCURES program by this past July.Not only are pharmacists registered- we are using the CURES system,with almost 500,000 patient activity reports accessed monthly bypharmacists.Active access to CURESreports for applicable patients isencouraged for all pharmacists,as is integration of CURES reportreview into daily pharmacy practice. The CURES reporting processis intuitive, and information onthe use of CURES is available vialink from the board’s website. Theboard has posted a “Red Flags”video to assist pharmacists in providing appropriate review of opioidprescriptions. Every pharmacist isencouraged to watch this video andwalk through the various patientvignettes presented. Under final administrationreview are additional SB493 regulations that allowpharmacists to provideservices for travel medications and another regulation outlining qualification requirements for thenew licensure category ofadvanced practice. Both ofthese are at the final stageof administration approval,with our hope that theseregulations are approvedand in place in the next fewmonths.Over the last few years, theboard has been working to developand implement multiple majorregulations that are providing California the ability to lead the nationin promoting pharmacy practice.Much of this work is nearingcompletion, as highlighted below: The board is nearingcompletion of its work ona major overhaul of compounding regulations forgeneral and sterile compounding. The implementation of these regulationswill represent a major effortfor the board and com- The board has securedSee President’s Message Page 3
Summer 2016BOARD OF PHARMACY3President’s MessageContinued from Page 2options for consumers whodesire to remove unwantedmedications from theirhomes.pounding community andhospital pharmacies. The board is also nearingcompletion of work forrequirements for pharmacies to provide drugtake-back services for thepublic, a rulemaking theboard hopes to have inplace by the end of 2016.This regulation relies uponthe federal Drug Enforcement Administration’s drugtake-back requirements andestablishes parameters forcollection receptacles inpharmacies, hospitals andskilled-nursing facilitiesas well as the use of mailback envelopes to provide The board’s Communication and Public EducationCommittee recently beganexamining the AffordableCare Act’s requirementsfor pharmacy translationsand interpreters for patientsin 15 languages. Section1557 of the AffordableCare Act forbids discrimination in health carebecause of race, color, national origin, age, disabilityand sex. This section ofthe act took effect July 18,2016, and will likely resultin impact to multiple current state pharmacy regulations.Thank you to every stakeholderwho took the time to attend a boardmeeting or submit public commentsfor the multiple pending regulationsthat have either been approvedor are pending final approval.Your participation and voice haveresulted in our ability to finalizemeaningful regulations that willdirectly affect the provision of safecare for the consumers who rely onour pharmacies.If you have not already doneso, I encourage you to attend aboard meeting and provide a voiceon the future of your profession.Mark Your Calendar for Upcoming Board,Committee Meetings; CE Credit AvailableFor Pharmacists, Pharmacy TechniciansInformation regarding locations and agendas for all board and committee meetings is posted at the board’s website,www.pharmacy.ca.gov, at least 10 days before each meeting.Packets of background material with information for agenda items are available for download from the website aboutfive days before each meeting. The agenda and meeting materials are available on the board’s website.For most meetings, pharmacists and pharmacy technicians who attend in person may be awarded six CE hours.Signing in and out on the day of the meeting will be required for CE credit.Meetings of the California State Board of Pharmacy in 2016 are scheduled for September 22, 2016, in SouthernCalifornia and October 26-27, 2016, in San Jose. Board meetings are webcast, when feasible.Upcoming meetings of committees for 2016 are: Communication and Public Education Committee: December 1, 2016 Licensing Committee: September 27, 2016As additional meetings are scheduled, they will be posted on the board’s website. Minutes of meetings also are postedonline.
Summer 2016BOARD OF PHARMACY4Protocol Enables Pharmacists to ExpandPublic Access to Antidote for Opioid Overdosetheir doctors to also prescribe naloxone.Alternatively, pharmacists may ontheir own suggest that patients fillingprescriptions for opioid medications alsoobtain naloxone.California pharmacists aretaking a more active role in efforts toprevent deaths from opioid overdosesby increasing access to naloxonehydrochloride, a medication that reversesopioid overdose.Authority for pharmacists to furnishnaloxone was established by AB 1535(Bloom), which was passed in 2014. Thelaw authorized the furnishing of naloxonepursuant to a protocol developed by theBoard of Pharmacy and approved bythe Medical Board of California. Themedication may be administered byintramuscular injection, intranasal sprayor auto-injector.The protocol, in California Codeof Regulations Title 16, section 1746.3,lays out specific requirements forpharmacists to screen potential recipientsand to provide training in preventing,recognizing and responding to opioidoverdose and in administering naloxone.In addition, the protocol requirespharmacists to complete at least one hourof approved continuing education trainingon all forms of naloxone hydrochloridebefore furnishing the medication.The protocol requires pharmacists todetermine whether the potential recipient(A) uses illicit or prescription opioidsor (B) “is in contact” with anyone whouses illicit or prescription opioids. Thepharmacist also must determine whetherthe person to whom the drug would beadministered has a known sensitivity tonaloxone; if so, the pharmacist may notprovide the drug.Translated screening questions forpotential recipients of naloxone whoseprimary language is traditional Chinese,Korean, Russian, Spanish, Tagalog orVietnamese are available on the Boardof Pharmacy website at http://www.pharmacy.ca.gov/licensees/naloxone info.shtml.The protocol also requirespharmacists to counsel and providerecipients with information aboutthe medication, including “dosing,effectiveness, adverse effects, storageconditions, shelf-life, and safety.” Therecipient is not permitted to waive therequired consultation. The pharmacist alsomust provide any available informationor referrals to appropriate resources toany recipient who “indicates interest inaddiction treatment, recovery services,or medication disposal resources at thistime.”As members of a health care team,pharmacists may recommend that patientsfilling prescriptions for opioids askIf the recipient is also the personto whom the naloxone would beadministered, the recipient is considereda patient for purposes of the protocol. Ifthe patient consents, section 1746.3(c)(7) requires the pharmacist to “notify thepatient’s primary care provider of anydrug(s) and/or device(s) furnished, orto enter the appropriate information ina patient record system shared with theprimary care provider, as permitted by thepatient and the primary care provider.”If the patient does not have a primarycare provider or does not consent tonotification, section 1746.3(c)(7) requiresthe pharmacist to “provide a writtenrecord of the drug(s) and/or devices(s)furnished and advise the patient to consultan appropriate health care provider of thepatient’s choice.”The full text of California Code ofRegulations section 1746.3 is available athttp://www.pharmacy.ca.gov/publications/naloxone protocol.pdf.A fact sheet about naloxone isavailable on the Board of Pharmacy website at http://www.pharmacy.ca.gov/publications/naloxone fact sheet.pdf.The Board of Pharmacy PrescriptionDrug Abuse Prevention page, includingpublic service announcement videos, isavailable at http://www.pharmacy.ca.gov/consumers/rx abuse prevention.shtml.
Summer 2016BOARD OF PHARMACY5Experts Warn Opioid Abusers Are TurningTo Common Anti-Diarrhea Drug Loperamideloperamide is “safe in therapeutic dosesbut extremely dangerous in high doses.”In June, the U.S. Food and Drug Administration warned that taking excessiveamounts of loperamide can cause seriousproblems with heart rhythm and lead todeath. Out of 48 cases of serious heartproblems associated with loperamide thatthe FDA received between 1976 and 2015,more than half were reported after 2010.As efforts to halt opioid abuse continue, experts warn that a growing number ofpeople who abuse painkillers are turningto an unlikely alternative: loperamide, ananti-diarrhea medicine that is widely soldover the counter as Imodium and otherbrands. For some who take massive dosesto ease withdrawal symptoms or get high,the results can fatal.A recent report in the Annals ofEmergency Medicine studied two cases ofsubstance abusers in New York who overdosed on loperamide and died. A statementissued with the report by the AmericanCollege of Emergency Physicians said thatAlthough the active ingredient inloperamide is an opioid, the medicationhas been approved by the FDA since 1976to help control diarrhea. The maximumapproved daily dose is 8 milligrams forover-the-counter use and 16 milligrams forprescription use.But in a 2012 study of almost 1,300loperamide abusers who posted in onlineforums, some reported taking 70 to 100milligrams a day. Seventy percent reportedtaking “megadoses” to alleviate opioidwithdrawal symptoms, while 25 percentsaid they did so in an effort to produceeuphoria.Researchers say the fatal overdoses inNew York reflect a broader and growingtrend of loperamide abuse. The AmericanCollege of Emergency Physicians saidthe Upstate New York Poison Center hada seven-fold increase in calls regardingabuse or misuse of loperamide from 2011to 2015. Meanwhile, national poison callcenters reported a 71 percent increase inloperamide cases from 2011 to 2014.“Loperamide’s accessibility, low cost,over-the-counter legal status and lack ofsocial stigma all contribute to its potential for abuse,” said William Eggleston, adoctor of pharmacy and lead author of theAnnals of Emergency Medicine study.“Our nation’s growing population ofopioid-addicted patients is seeking alternative drug sources with prescription opioidmedication abuse being limited by newlegislation and regulations,” Dr. Egglestonsaid. “Health care providers must be awareof increasing loperamide abuse and itsunder-recognized cardiac toxicity. This isanother reminder that all drugs, includingthose sold without a prescription, can bedangerous when not used as directed.”“Notice to Consumers” Available in Various FormatsCalifornia Code of Regulations section 1707.6 requirespharmacies to display a Notice to Consumers as specified insubsection (b). Full-size posters in English and Spanish areavailable to be ordered at the board’s website. Smaller versionsChinese, Korean, Russian, Spanish, Tagalog and Vietnamese maybe printed or ordered at the board’s website.As an alternative to a printed format, Section 1707.6 allowspharmacies to display the Notice to Consumers on a videoscreen. The Notice to Consumers is available in video format inEnglish and Spanish at the Board of Pharmacy’s website under“Publications for Applicants and Licensees.” Both versions canbe downloaded as PowerPoint presentations.A pharmacy also may seek approval of another format ordisplay methodology from the Board of Pharmacy’s ExecutiveOfficer.Section 1707.6 (a)(1)-(4) lists specific requirements fordisplaying the Notice to Consumers on a video screeninstead of in printed form. The section requires:(1)The video screen is at least 24 inches, measureddiagonally;(2)The pharmacy utilizes the video image noticeprovided by the Board of Pharmacy;(3)The text of the notice remains on the screen for aminimum of 60 seconds; and(4)No more than five minutes elapses between displaysof any notice on the screen, as measured between thetime that a one-screen notice or the final screen of amulti-screen notice ceases to display and the time thatthe first or only page of that notice re-displays.
Summer 2016BOARD OF PHARMACY6Federal Group Recommends Best PracticesFor Making Prescription Drug Labels AccessibleTo Blind, Visually Impaired, Elderly PatientsRecommendations of the federalworking group include: Encourage patients tocommunicate their needs topharmacists. Follow universal patient-centeredprescription drug container labelstandards. Make container labels availablein audible, braille and large-printformats. Explain the choices andprovide the format selected bythe patient. Ensure that duplicate accessiblelabels preserve the integrity ofthe print prescription label. Federal best practices for prescriptiondrug containers have been developed tomake it easier for people who are blind,visually impaired or elderly to access labelinformation.The recommended best practiceswere developed by a working group ofconsumer and drug industry advocatesconvened by the United States AccessBoard under the Food and DrugAdministration Safety and Innovation Act(Public Law 112-144, 126 Stat. 993).The working group stated that peoplewho cannot read printed prescriptionlabels because of visual impairment “alltoo often take the wrong medication,the wrong amount, at the wrong timeand under the wrong instructions.” Thegroup also noted that most people whobecome blind or visually impaired do soafter age 60 – a time when many takemultiple medications and have physicaland cognitive conditions that increasethe need for “safe, consistent, reliableand independent access” to drug labelinformation.Subject accessible prescriptionlabels to the same quality controlprocesses used for print labelsto ensure accuracy and patientsafety. Maintain patient privacy (HIPPArules) when preparing accessibledrug labels. Keep a sufficient inventory ofsupplies to provide accessiblelabels. Provide drugs with an accessiblelabel within the same time frameas would be provided to patientswithout visual impairments. Don’t impose an extra fee tocover the cost of providing anaccessible drug label. Ensure durability of accessiblelabel formats until theprescription expiration date. Select a container that bestsupports the type of accessiblelabel provided. Ensure all required informationcontained on the printprescription drug label isprovided in the same sequence onthe accessible label. Include in accessible labels theinformation on warning labelsadded to the container at thepharmacist’s discretion.A variety of methods and technologiesexist to enable blind, visually impaired andelderly people to access information onprescription labels, including: Hard copy labels printed in largetype or braille. Digital voice or text-to-speechrecorders – “Talking bottles”that use a small electronic deviceattached to a drug container toread the label information aloud. Radio Frequency IdentificationDevice (RFID) tags – AttachingRFID tags to drug containers thatenable a dedicated device used bythe patient to read the label aloud. Smart devices and computersequipped with electronic braille,large text and audio technology toaccess electronic text.A brochure listing the best practiceswas issued in June 2016 by the NationalCouncil on Disability. The brochure isavailable at http://www.ncd.gov/sites/default/files/ADLP 508.pdf.Additional information about therecommended best practices and a linkto the working group’s full report isavailable at labels.
Summer 2016BOARD OF PHARMACYValerie Muñoz Appointed to BoardValerie Muñoz of La Puente was appointed in July as apublic member of the Board of Pharmacy by the Senate RulesCommittee.Ms. Muñoz is mayor of La Puente and has served on theCity Council since 2014. She is a delegate to the CaliforniaContract Cities Association and an alternate to the League ofCalifornia Cities and the Foothill Transit Authority board.She works as a practice and human resources managerfor an optometry business. She earned a master’s degree inleadership and organizational studies and a bachelor’s degree in organizational studiesfrom Azusa Pacific University.Ramón Castellblanch LeavesAfter 2 Terms as Public MemberBoard of Pharmacy member Ramón Castellblanch, Ph.D.,is leaving after two terms as a public member of the board.Dr. Castellblanch was appointed to the board by theSenate Rules Committee in 2009 and was reappointed in2012. He served most recently on board’s Communicationand Public Education Committee and the Legislationand Regulation Committee. Dr. Castellblanch previouslyserved as the Chairperson on the Prescription Drug AbuseSubcommittee. Dr. Castellblanch was a supporter of patientcentered prescription labels, translation and interpreterservices for pharmacy patients, prescription drug abuse awareness and education as wellas consumer health education.7Board Re-electsAll 3 OfficersBoard of Pharmacy PresidentAmy Gutierrez, Vice PresidentDeborah Veale and Treasurer VictorLaw were re-elected as officers at aboard meeting on April 27.Dr. Gutierrez joined the board in2012. She worked at the Los AngelesCounty Department of Health Servicessince 1984 and has served as chiefpharmacy officer and director ofpharmacy since 2006. Dr. Gutierrezearned a doctorate in pharmacy fromthe University of Southern California,School of Pharmacy.Ms. Veale has served on the boardsince 2010. She has been director ofpayer relations for CVS Pharmacysince 2006 and previously served inseveral positions with Albertsons/Sav-On Drugs. She earned a pharmacydegree from the University of Iowa,College of Pharmacy.Mr. Law has been a boardmember since 2012. He has servedas chief pharmacist and president atAlpha Medical Pharmacy Inc. since1987. He earned a bachelor’s degreein pharmacy from the University ofOklahoma in 1976.NABP Honors Stanley C. WeisserWith Top Award for Distinguished ServiceThe National Association of Boardsof Pharmacy (NABP) has presentedits highest honor, the Lester E. HostoDistinguished Service Award, toCalifornia State Board of PharmacyMember Stanley C. Weisser.Mr. Weisser was honored for“his strong commitment to protectingthe public health and his successfuladvancement of higher standards andstronger oversight for sterile compoundingpharmacies,” the NABP said in a writtenstatement. The award was presented at theNABP’s 112th Annual Meeting May 1417, 2016, in San Diego.A memberof the CaliforniaState Boardof Pharmacysince 2007, Mr.Weisser servedas presidentfrom 2010to 2015. Aschairman ofthe SB 493 Implementation Committee,he led efforts to specify requirements forlicensing advanced practice pharmacistsin California and to develop three stateprotocols and two additional regulationsto implement extended care requirements.He is an associate clinical professorat Loma Linda University School ofPharmacy and serves on the executivecommittee of Redlands CommunityHospital and the Board of Trustees ofUniversity of Redlands.The Lester B. Hosto DistinguishedService Award recognizes individualswhose efforts to protect the public healthgreatly further the goals and objectivesof the NABP. The award is named inmemory of former NABP PresidentLester E. Hosto, whose contributions tothe pharmacy practice were recognizedby practitioners in his state, pharmacyleaders across the nation and former U.S.President Bill Clinton.
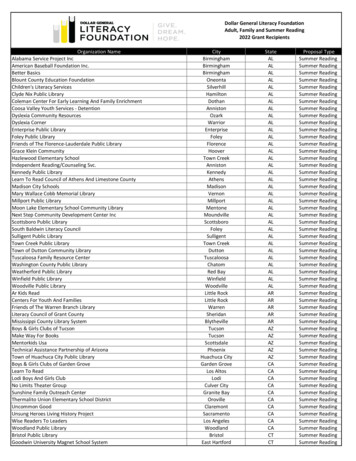
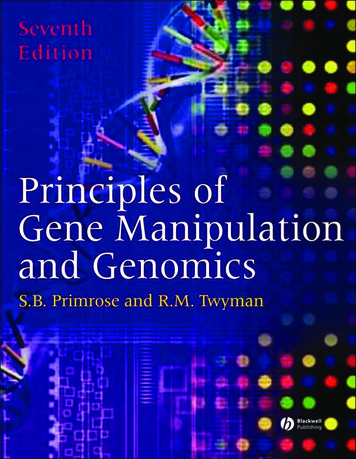
Summer 2016BOARD OF PHARMACYDid You Know?Almost six of every 10 licensed pharmacists in Californiaare women. According to the California State Board ofPharmacy, 58 percent of the 35,526 registered pharmacistswith California addresses on file are women, compared with 42percent who are men.CaHf,orn·ia .Pha1rma c sts, by Gandc r1 8Board RecognizesRegistered PharmacistsFor 50 Years of ServiceThe Board of Pharmacy pays tribute to those who havebeen registered California pharmacists on active status forat least 50 years. The board recognizes these individuals andgratefully acknowledges their years of contribution to thepharmacy profession. These pharmacists may take great pride inbeing part of such an honorable profession for so long.Pharmacists who recently received a certificatecommemorating 50 years of service and were invited to attendBoard meetings to be publicly honored are:The California numbers reflect a national trend. A 2014National Pharmacist Workforce Study issued by the AmericanAssociation of Colleges of Pharmacy reported that women madeup 57.1 percent of actively practicing pharmacists in the UnitedStates.In addition, female pharmacists in California are mostlyyounger than their male colleagues. More than half – 51 percent– of licensed female pharmacists who are California residentsare between the ages of 30 and 44. Meanwhile, 53 percent oflicensed male pharmacists who live in the state are 50 or older.Cal tfom a Ph;nmac·1m by Age Grcmp., byG@ndE!!rFreeman, Lary E.Blair, William J.Chaplain, Raymond MilesGerome, Norman LouisHeincy, Charles DanielHill, Archie RichardHorowitz, Kenneth N.Hutchison, Loyal DwayneLyons, Noel E.Mariottini, Raymond E.Marotto, Ronald RaymondPetroni, Frank GarySiu, KienkiSiu, KingmunSudalter, LawrenceTaj, Patricia KawaseZingarelli, Robert N.Incline Village, NVSanta Ana, CASan Clemente, CACalabasas, CAGranite Bay, CASanta Rosa, CAHermosa Beach, CAStockton, CAChico, CAHollister, CAGoleta, CAAtascadero, CAFort Jones, CAAlameda, CASanta Clara, CASan Ramon, CAFresno, CAThe following pharmacists were honored for being licensedfor 50 years at a previous Board meeting:- I :g . IPhillip E. GraussC.,.,. I JIAs of June 15, 2016, a total of 41,586 pharmacists werelicensed by the Board of Pharmacy with active licenses. Thetotal includes 5,947 pharmacists with addresses in other statesand an additional 113 with addresses outside the United States.Loyal D. Hutchison Kingman Siu
Summer 2016BOARD OF PHARMACY9New Compounding Regulation Will ChangeElements For Master Formula DocumentsA master formula documentis the specific recipe written by apharmacy before it compounds apreparation. The requirements fora master formula will change on1/1/17, pending approval of theboard’s compounding regulations.Assuming the regulations areadopted, the required elements ofthe master formula will change andmust appear in a cohesive document. As with prior regulations, themaster formula must be preparedbefore compounding begins.As proposed, California Codeof Regulations, Title 16, section1735.2, subsection (e), will require:A drug preparation shall notbe compounded until thepharmacy has first prepared awritten master formula document that includes at least thefollowing elements:(1) Active ingredients to beused.each step in preparation of thedrug.(7) Post-compounding processor procedures required, if any.(8) Instructions for storageand handling of the compounded drug preparation.Here are some examples ofwhat you might expect the masterformula document to provide foreach of the above elements:(1) Active ingredients tobe used – For example, wemight expect to see the activeproduct(s), active pharmaceutical ingredient(s) (API), oractive bulk substance.(2) Equipment to be used –For example, the master formula document might reflectthe hood(s), repeater pumps,scales or other equipment.(3) The maximum allowablebeyond use date for the preparation, and the rationale orreference source justifying itsdetermination.(3) The maximum allowablebeyond use date (BUD) forthe preparation, and therationale or reference sourcejustifying its determination– For example, the rationaleor reference source justifyinghow the BUD is determinedmight include:(4) Inactive ingredients to beused. For a compounded preparation – stability studies.(5) Specific and essentialcompounding steps used toprepare the drug. For a compounded sterile preparation – methodsuitability test, containerclosure integrity tests, and/or stability studies and/orsterility study.(2) Equipment to be used.(6) Quality reviews required at(4) Inactive ingredients to beused – For example, the master formula document mightreflect the inactive product(s)or bulk substance(s) includedin the preparation: for example, normal saline (NS),5% dextrose in normal saline(D5W).(5) Specific and essentialcompounding steps usedto prepare the drug – Forexample, the master formuladocument might reflect a narrative of the physical processes: which ingredients, in whatform, what strengths/volumesare mixed first, under whatcircumstances, held underwhat conditions for how long,in what environment, etc.(6) Quality reviews requiredat each step in preparation of the drug – We mightexpect to see a description ofeach quality review in eachspecific and essential compounding step. For example,the master formula documentmight reflect that compounding staff will: Check that all powder is inthe solution for a reconstituted product. Check that no powder/ liquid left the neck of the vialor ampule. Check for correct coloring.See Master Formula Documents Page 10
Summer 2016BOARD OF PHARMACY10Master Formula DocumentsContinued from Page 9- document PSI, compare with manufacturersallowances. Check for coring of the stopper. Check for precipitates. Check for correct coloring. Check for leaks.(7) Post-compounding process or proceduresrequired, if any – For example, the master formula document might reflect that compoundingstaff will: Check for coring of the stopper. Check for precipitates. Check for leaks. Place [specified ingredient or preparation] in adefined quarantine area. Only dispense preparation after all processes orprocedures above are completed. Send [X] number of samples out for sterilityand endotoxin testing.(8) Instructions for stor
skilled-nursing facilities as well as the use of mail-back envelopes to provide . Meetings of the California State Board of Pharmacy in 2016 are scheduled for September 22, 2016, in Southern California and October 26-27, 2016, in San Jose. Board meetings are webcast, when feasible. Upcoming meetings of committees for 2016 are: