Transcription
Esthetic DentistryCase selection for porcelain veneersChing Chiat Lim*The options for correction of unesthetic teeth are numerotis: among these treatments,porcelain veneers have received substantial attention from the profession and patients.The increase in dental health awareness and advances in dental materials and technology,such as the acid-etching technique, improved physical properties of composite luting resin,and the use of silane coupling agents, have contributed to the success ceramic veneersenjoy today. However, no single material or technique is ivlthout its limitations. Thisarticle therefore aims to review the criteria for case selection and the limitations ofporcelain veneers in restorative dentistry. (Quintessence Int 1995:26:311-3¡5.)IntroductionPatients often request cosmetic improvements in theirteeth. Frequently, such an improvement also improvesthe patients' sense of well being and self-esteem. Howwell an individual looks is often a contributory factorto success or failure in life in today's highly competitivesocieties.A porcelain veneer is a thin facing, about 0.5 to0.7 mm thick,'- covering the labial aspects of anteriorteeth and the buccal aspects of some premoiar teeth.Veneers can be fabricated from traditional feldspathicporcelain or other ceramic materials, such as castableor machinable glass ceramics. The veneer is thenbonded to the enamel surface by mechanical andchemical means. The mechanical attachment is achievedby etching the enamel and the porcelain. The resincomposite is then allowed to form a strong micromechanical bond similar to that achieved with enamel. An additional chemical attachment to the porcelaininterface is accomplished by silane bonding.* Studieshave shown that etching the porcelain surface is ofgreater importance to overall bond strength than isusing a silane coupling agent alone. Lecturer. DepartmenlofRestorative Dentistry. National University ofSingapore, Faculty of Denlistij. Singapore.Reprint requests: Dr Ching Chiat Lim. Lecturer, Department ofRestorative Dentistry, National University of Singapore, Faculty ofDentistry. 5 Lower Kent Ridge Road. Singapore 0511, Singapore.QuinWásence InternationalVolume 2s. Number 5/1995Uses of porcelain veneersManagement of noncarious surface defectsPorcelain veneers can be used for the management ofnoncarious defects, such as localized enamel malformations and hypoplasia. Porcelain veneers have beensuggested for the treatment of eroded teeth andenamel hypocaicification.' However, bonding ofveneers to poor-quality enamel might lead to marginalleakage and the eventual failure ofthe restorations.Masking of discolorationDiscoloration arising from fluorosis, tetracycline staining, or necrosis can be treated with porcelain veneers,provided that the stains are not too dark. Limitationsshould always be recognized. Staining arising fromfluorosis can usually be treated successfully withceramic veneers when the surface enamel is removedduring tooth preparation (Figs I to 3).Repair of structural defeetsHorn* suggested the use of porcelain veneers to repairfractured incisai edges, to correct mild malalignment ofteeth, to achieve closure of diastemas, and to restorepeg-shaped lateral incisors. It is the author's opinionthat resin composite may be a better materiai for casesthat require only minimal replacement of tooth structure. This is because a tooth preparation of some kindis required for a porceiain veneer, no matter how smallthe tooth preparation, to allow enough bulk ofporcelain at the margin for strength. On the other311
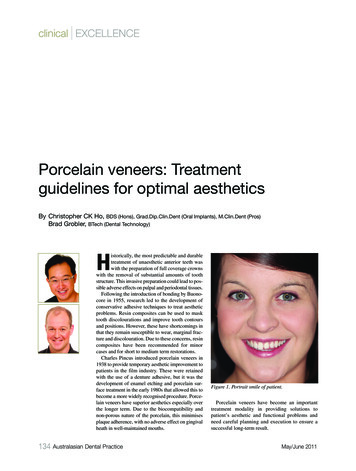
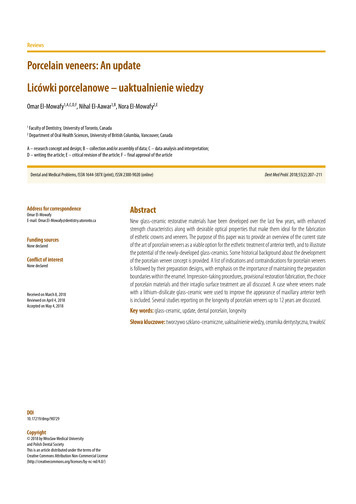
Esthetic DentistryFtg 1 Severe tluorosis ¡s evident on the maxillary anteriorteeth.Fig 2 The dark discoloration has been removed alterintraenamei preparation for porcelain veneers was completed.is required but placement of a post core is contraindicated.Repair offractured porcelain facings onfixedprosthesesMillar' suggested the use of porcelain vetieers to repairfractured porcelain facings on fixed partial dentures.This is only possible if the other aspects of theprosthesis are satisfactory and otily the porcelainfacing requires replacement. Otherwise, it is better toreplace the whole prosthesis.Fig 3Six maxillary anterior porcelain veneers are cemented.hand, replacement of tooth structure with direct resincomposite can easily be achieved without any toothpreparation, making the procedure more conservative.Tooth preparation is necessary for porcelain veneersbecause it provides the ceramist with a definite marginfor finishing. However, when a few teeth are siightlytnalaligned, involving full labial buildup, porcelainveneers involving some tooth preparation may be moreesthetic and durable than direct resin compositeveneers, which consume more clinical time.Porcelain veneers can also be used for the correction of cosmetic or minor functional needs in adolescent's teeth. Crown preparations on adolescent teethare difficult because ofthe risk of infringement on thelarge, immature pulp by too deep a shoulder preparation, Porcelain veneers are also indicated in endodontieally treated teeth in which esthetic improvement312Replacement of old resin composite veneersPorcelain veneers are frequently indicated for thereplacement of old resin composite veneers, withstaining and wear being the most common complaintsfrom patients.Orthodontic retainersPorcelain veneers have also been used as orthodondicretainers to close postorthodontic diastemas."*" Thisworks by maintaining tooth contact with the adjacenttooth, thus preventing the reappearance of spaces. Thelong-term stability of this form of retention is unknown. Applications of this new concept are extensive, but care must be taken to evaluate the hmits of thistechnique with adequate long-term chnical studies.Clinical observations have also confirmed thatetched porcelain veneers are ideally suitable fortnandibular incisors if adequate interincisal spaceexists and the correct tooth preparation design ischosen for the required occlusion.' Criteria for case .selectionPatients who are selected to receive porcelain veneersor any other restorative work, should have good oralQuintessence '"'"mntinnnl Vnlritmhnr.i'ijor.
Esthetic Dentistryhygiene, healthy gingival tissue, and no occlusaldisharmony.'-' The placement of porcelain veneers isan irreversible procedure because ofthe neccessity fortooth preparation. Therefore, the criteria for porcelainveneers must be carefully reviewed before the procedure is undertaken.Síi7í/f and dynamic occlusal relationshipLong-term studies have indicated that porcelain veneers seldom delaminate.' ''' The usual mode of failureis fracture of comers; this frequently happens at theincisai edges. It is therefore important to analyze thestatic and dynamic occlusion before tooth preparation.The occlusion will dictate the choice of tooth preparation design (not discussed in this article). The incisaiporcelain finishing line is determined by the contactrelationships between the incisors and canines incentric and eccentric positions."" The margins shouldbe placed so they do not contact the opposing dentitionduring the rest position.' Ideally, occlusal contactsduring centric occlusion and lateral excursion should beon porcelain or tooth strucmre completely. Occlusalinterferences and parafunctional habits are contraindications for porcelain veneers, because they will result incrack formation and eventualfractureofthe restoration,Periodontal and oral health stattisA healthy periodontium fonns a strong foundation onwhich all restorative work will rest. It also facilitatesease of impression taking, cementation, and futuremaintenance. It is therefore important to assess thepatient's overall periodontal and oral health statusbefore the procedure is begun, Mouthbreathers whohave poor gingival health are poor candidates forporcelain veneers.Condition of toothDegree of discolorationIf the tooth is grossly discolored, it maybe necessary tobleach the tooth before the veneer is placed. However,the unpredictable stability of bleaching poses theproblem of the return of discoloration beneath theporcelain veneers once they have been cemented.Usually, the discolorarion in tetracycline stainingbecomes more severe as the enamel is reduced. Suchcases may require masking of areas of marked discoloration with opaque glass-ionomer cement or opaqueporcelain. In either case, the parient should be warnedofthe compromised esthetics whereby the veneers mayappear opaque. Because the bond strength betweenglass-ionomer cement and resin composite is not aspredictable as that between etched enamel and resinQ ui ntessefloerlniemQttonoiNumber 5/1995composite, it is preferable to mask areas of markeddiscoloration with opaque or intensive porcelain (VitaAlpha porcelain. Vita Zahnfabrik). Precise instructions to the laboratory technician regarding areas ofmarked discoloration are therefore crucial. A photograph of the prepared tooth is usually helpfiil if anin-house technician is not available. The use of resincomposite to mask marked discoloration is usuallyinadequate, because the resin is usually too translucentto have any masking effect.Extent of cariesCaries, if present, should be minimal. If little or noenamel is left after caries removal, placement of aporcelain veneer is usually contraindicated, Tiiis isbecause tbe thin veneer is strengthened by bondingwith the underlying etched enamel. The veneer-toothcomplex is weakened when the surface area of enamelavailable for bonding is decreased by 50%,' Extent of restorationA restoration, if present, should be smail enough thatthe area for bonding with enamel is not compromised.The cavity design of the restoration should incindemargins that end in enamel, where possible. The oldrestorations should be replaced if the underlying cariesstatus is questionable.Quality' of toothIf the amount of enamel for bending is compromiseddue to any ofthe factors above, a veneer shell crown orconventional crown may be indicated instead of aveneer facing.Structural defects, such as amelogenesis imperfectaand dentinogenesis imperfecta, that leave insufHicientenamel and tooth structure for bonding are a definitecontraindication for veneer.Teeth with iarge areas of exposed dentin areunsuitable for porcelain veneers. However, small areasof exposed dentin may be treated with dentinalbonding agents or glass-ionomer cements.Patients motivation to tnaintainThe patient's attitude toward dental health care shouldbe assessed before porcelain veneers are attempted. Avigilant home care program and regular recalls areimportant to maintain the longevity ofthe restoration.Patient's expectationsThe patient's expectations should be realistic. Adiagnostic waxup may be required to demonstrateareas of limitations when porcelain veneers are to beused for correction of mild malalignment.313
Esthetic DentistryOrai habitsTlie presence of oral habits, such as nail or pencilbiting, is a contraindication for veneers because theshearing stress may be too great for the ceramics towithstand.'*Advantages of porcelain veneersThe porcelain veneer is usually fabricated in tht;laboratory. It therefore utilizes the ceramist's expertisein creating a lifelike restoration, and relies less on theartistic skill ofthe dentist to individualize and characterize the veneers, as is required with direct resincomposite veneers." Compared with the resin laminateveneer, the porcelain laminate veneer also has thefollowing advantages:*1. Color stability and lifelike appearance2. Maintenance of luster3. Higher resistance to abrasion, staining, and thedeleterious effects of alcohol, medications, andother solvents4. Biocompatibility with gingival tissue5. Increased chemica! and mechanical bonding toresin composite6. Less clinical chairside timeWhen two or more veneers are indicated, directresin composite veneer may be more lime consumingto fabricate. It would be more eificient to indicateporcelain veneers for such cases, provided that theother criteria are met.Limitations of porcelain veneers1. Changes in the color, length, contour, and contactareas of porcelain veneers fabricated by therefractory die or platinum foii technique arelimited,* because no reglazing or firing is possiblewith either technique. Tlie veneers have to beremade or modified with ctalored luting cementswhen the shade is incorrect, and the success ofshade modification with luting cement is highlyquestionable. However, when the veneers arefabricated with the castable DICOR (Dentsply)leucite-reinforced ceramic press system (IPS Empress. Ivoclar} or the copy milling system (Celay,Mikronat), postadjustment staining and reglazingare possible.2. Stabilization at try-in stage is difficuh becausethere is no tensofrictional grip." However, thisdifficulty can be overcome by making a defhiiteincisai step on the labial surface of the veneer314preparation (Ironside JG. personal communication, 1992) or dimples in the cenicr of thepreparation.'*3. The dental laboratory costs involved may makethe restoration more expensive to produce andthus less appealing to the patients."4. Margina! adaptation of most veneers is about 1Ü0 im or more. ' '' Very lew with a marginal accuracyof less than 20 \xm have been achieved.'5. Thin sections of porcelain tend to be monochromatic and lack the break up of color present innatural teeth. Ifthe veneer is too translucent, areasof marked discoloration may show through;however, a more opaque porcelain buiidup mayproduce a high-Vaiue, monochromatic veneer,lacking in transiucency and dentinal contrast. 6. It is ven,' difficult to match the shade of a singleporcelain veneer to the rest of the dentition. Insuch a case, a direct resin composite veneer maybe preferred to the porcelain veneer.7. The bonding procedure is very technique sensitiveand time consuming.8. Diagnosis of caries underneath cemented porcelain veneers is difficult (Wlson NHF, personalcommunication, 1994).9. It is difficuh to replace and repair porcelainveneers when they fail (Wilson NHF. personalcommunication, 1994).10. Acidulated phosphate fluoride and stannoiisfluoride should be avoided on porcelain veneersbecause both the porcelain and resin compositesilica may be affected.-'ConclusionsThe success of porcelain veneers depends very muchon the method of fabrication and, most importantly,case selection. Because some of the research in thisfield has been based on personal preference andanecdotal information, more objective research isrequired so that porcelain veneers will become fullyaccepted by both the profession and the public as analternative treatment in the field of conservativedentistry.References1. Millar BJ. Porcelain venoms. Dent update. l937:Nov:331-390.2. Faunce VR. StmcttJred ceramics for laminate veneers, CDS Rev3. Clyde JS. Cilmour A. Porcelain veneers: A preliminary review BrDent J 19SS:i64;9-l4.Quintessence InternationalVolume 26, Number 5/1995
Esthetic Dentistry4. Quinn F, McConnell RJ, Byrne D. Porceiain laminate; A review. BrDentJ I985;i6l:61-6.í.5. CalaniLa JR. Simonsen RJ. EfTect of coupling agents on bondstrength oietciied porcelain abstract 79]. J Dent Res Í984;o.l: 179.6. Reid JS, Simpson MS. Taylor GS. Using porcelain veneers to treateroded teeth. Dent Abstr Í99I:36:255-2S6.David KorsonAesthetic Designfor Ceramic Restorations7. BoksmanL, Jordan RE. Suzuid M, Gahl KA, Burgoyne AR. Etchtdporceiain labial veneers. Ont Dent I985;62; 1I-Í9.S. Horn HR. Porcelain laminate veneers bunded to etched onam«!Dent Ciin North Atii Í98.1;27:671-6a4.9- McLean JW. The science and art of denta! ceramics. Opcr Dent199l;t6:t49-i56.10. Hunt NP. Hypodontia-problems of pertiianent space dosure Br JOrthod Í983;I2:I49-Í52.11. Reid JS, Stirrups DR. A new solution to a dlíTicult problem oforthodontic retention Br J Ortho l9S7;i4:28t-283.t2. Freedman G, Ibsen R. Nixon R. Cosmetic roundtable: When to prepor not to prep: Three costnetic dentists debate. Dent Todayi989;S:22,24,26-27 passitn.13. Reid JS, Murray MC. Powers SM. Porcelain venccrs-A fuur yearfollow up. Rest Dent 19KS.4:6Ü-66.t4. Caiamia JR. Clinical evalgatioti of etciied porcelain vcnccrs. Am JDent 1939:2:9-15.15. Gougouiakis A. Murrranr WH, Barbakow I-. Lutz F. Retention rateand margin adaption of Cerec veneers ir vitro. In; Mörmann WH(ed). Proceedings of an International Symposium on ComputerRestorations: State of the Art of the CEREC Method. Chicago;Quintessence, 199L:537-545.16. Heyde JB, Cammarato VT A restorative system for repair of defectsin anterior teeth: The laminate veneers Dent Ciin North Amt98l;25:337-345.17. Greggs T. Laboratory procedures [n: Garber DA. Goldstein RE,Feinnian RA eds¡. Porceiain Laminate Veneers. Chicago: Quintessence. l9R8:fiO-KI.The mostiiLittiral,esthetic resultsin (ientalceramics canbe achieve(]with contemporaty techniques—atid rhis book describeshow. Investigated are the characteristics ofnatural dentition, tissue tnanagement, impressions, occlusal records, waxino- techniques,color, and kboratoty technit ues, includingmethods for an aesthetic ceramic margin,opalescence, and development ofthe dentinetnamelon. Klled with practical tips, this bookis ideal for dentists and technicians.US 78159 pages; 292 color tllus; ISBN I-B5097-034-3iS. Dicor Clinical Instruction Manual. York, PA: Dentsply, 1984.Í9. Tay WM. Lynch E, Auger D. Effects of some finishing techniques oncervicai margins of porcelain laminates. Quintessence Int1987;i8:599-602.20. Cerutti A. Marginai adaption ofCerec veneers in vivo. In- MörmannWH (ed). Proceedings of an international Symposium on ComputerRestorations: State of the An of the CEREC Method. Chicago:Quititessence, 199t:5í3-557.1\. Essig ME. IsenbergBP. Leinfelder KF. Liu PR In vitro evalution ofCerec veneers utilizing standardized preparation template. In:Mörmann WH (cd). Proceedings of an International Symposium onComputer Restorations: State ofthe An ofthe CEREC Method.Chicago: Quintessence, 1991:547-552.22. Harasani MH. Isidor F. Kaaber S. Marginal fit of porcelain andindirect composite laminate veneers under in vitro conditions. ScandJ Dent Res 1991 99:262-268.23. SorensenJA,Stmt?:JM,AveraSP, Materdomini D. Marginal ñdelityand microleakage of porcelain veneers made by two techniques. JProsthelDent I992;67.16-22.Contents1 Studies nl Natural Denticinn2 Dcnrisr-lcchmciati-Paticnt Communication3 Tissue Management for Aestheticand Biological Harmony4 Impressions and Occlusal Records5 Aesthetic Wax Diagnostic Control6 Accurate Registration and Communicationof Colour Characteristics7 Advanced Laboratory' Techniques8 Case Studies24. Sim C, Ibbetson RJ. Comparison of Tit porcelain veneers fabricatedusing different techniques. Int J Prosthodont i993;6;.í6-42.25. LitiiCC, Ironside JG. An in vitro study of the marginal adaptationof two ccraniic veneer systems labstract 74 . J Dent Resi994;73:746.26. Lim CC. The Marginal Adaption of 3 Ceramic Veneer TechniquesIMDS thesisl- Sydney. Australia: Univ of Sydney. 1993.27. Yaffe A, Zalkind M. The effect of topical appiicatjon of" fluoride oncomposite restorations. J Prosthet Dent i981:45:59-62.pbooh/Order NowToll free 1-800-621-0387Fax 708 682-3288Quintessence Publishing Co, IncQuintessLlptamatioñal—Vsltamo
intraenamei preparation for porcelain veneers was com-pleted. Fig 3 Six maxillary anterior porcelain veneers are cemented. hand, replacement of tooth structure with direct resin composite can easily be achieved without any tooth preparation, making the procedure more conservative. Tooth preparation is necessary for porcelain veneers