Transcription
10/16/2014Brinton Clark, MD, MPHDepartment of Medical EducationProvidence Portland Medical CenterOctober 25th, 2014Oregon Society of Physician Assistants Fall Conference 45 yo woman with BMI 40kg/m2 (weight278#)Diabetes on 55 units of lantus, 15 units oflispro QAC, exanitide, metformin.Hemoglobin A1C 9.2%Hypertension, hyperlipidemia, physicallyinactive with worsening back and leg pain.Obesity TrendsReview of Bariatric ProceduresIndications for Bariatric SurgeryMedical Outcomes of Bariatric SurgeryComplicationsMedical Management of Patients after SurgeryLocal Resources1
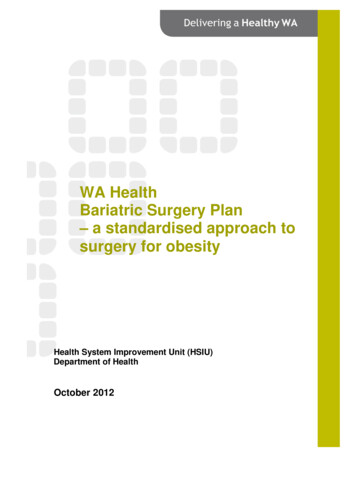
10/16/2014 Normal Weight: BMI 18.5-24.9Overweight: BMI 25Obese: BMI 30Morbidly Obese: BMI 40 or 35 with 2comorbiditiesObesity Trends* Among U.S. AdultsBRFSS, 1990, 2000, 2010(*BMI 30, or about 30 lbs. overweight for 5’4” person)200019902010No Data 10%10%–14%15%–19%20%–24%25%–29% 30%More than 1/3 of all US adults are obese14.5% of US adults have BMI 35, 7% BMI 40Estimated annual medical costs of obesity 150-200 billionMedical costs 1500-2700 higher per yearfor obese patients2
10/16/2014 Increased Mortality Cancer (endometrial, breast,prostate, colon)Diabetes Gallbladder diseaseHypertension GERDDyslipidemiaCoronary Heart Disease NASH OsteoarthritisCongestive Heart FailureThromboembolic Stroke Stress Incontinence Menstrual Irregularities andSleep ApneaRestrictive Lung Disease InfertilityChronic Kidney Disease PsychosocialApproximately 200,000 surgeries/year in USMost common procedures are: Roux-en-Y Gastric Bypass (RYGB) Sleeve Gastrectomy (SG) Adjustable Gastric Banding (AGB)DeMaria EJ. NEJM 2007; 356:217621833
10/16/2014DeMaria EJ. NEJM 2007; 356:21762183DeMaria EJ. NEJM 2007; 356:21762183 Body Mass Index (BMI) 40 kg/m2BMI 35 kg/m2 with 1 serious comorbidity Diabetes Obstructive sleep apnea or obesityhypoventilation Hypertension Hyperlipidemia Non-alcoholic fatty liver disease orsteatohepatitis Debilitating arthritis AsthmaMechanick JI. Obesity 2013; 21:S1.4
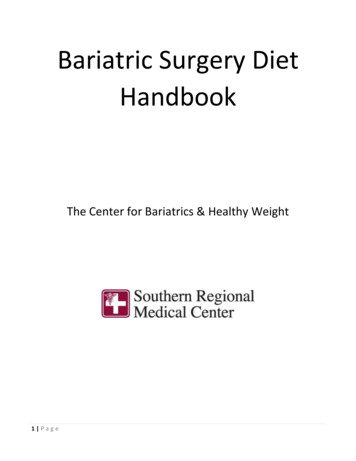
10/16/2014 Excess body weight (EBW) weight aboveideal body weight at BMI of 25kg/M2RYGB: Approximately 60-80% EBWSG: 60-70% Excess Body WeightAGB: 40-60% Excess Body WeightPuzziferri et al. JAMA. 2014; 312:934-42. ity of Life5
10/16/2014 Randomized, single center, non-blinded trial150 patients with uncontrolled diabetesBaseline A1C 9.3%, avg diabetes for 8.3 yearsAverage BMI 36 (included BMI 27-43)3 year follow up of 137 patients (91%)Primary endpoint A1C of 6.0%Schauer PR et al. NEJM; onlineMarch 31, 2014 Randomized, 4 centers (US, Taiwan), unblindedtrial of 120 patients with diabetes Baseline A1C 9.6%, avg diabetes for 9 years Average BMI 34 kg/m2 (30-39.9) 12 months follow up 114 patients (95%) Primary endpoint composite of A1C 7%, LDLcholesterol 100mg/dL, SBP 130mmHGIkramuddin S. JAMA. 2013; 309:2240-22496
10/16/2014 Systematic Review of 6 studies: RYGB diabetes remission rate 66.7% AGB diabetes remission rate 28.6% Swedish Obesity Subjects Trial (prospectivecontrolled trial) of subjects without diabetes:Diabetes developed in 6.8 cases per 1000person-years vs 28.4 (adjusted hazard ratio0.17)31. Puzziferri N. JAMA. 2014;312:934-42. 2. Carlsson L. NEJM.2012;367: 695-704. Schauer 3 year RCT: Non significant differencein BP but significant reduction in # of medsneeded2LABS Consortium Observational Cohort Study:Hypertension remission 38% RYBG, 17% ABG31. Ikramuddin S. JAMA. 2013;309: 2240-2249 2. Schauer PR etal. NEJM. 2014; 370: 2002-31. 3.Courcoulas AP. JAMA 2013;310:2146-24257
10/16/2014 Systematic review – 3 studies. Remission ofhyperlipidemia 60.4% after RYGB, 22.7% after AGB1. Schauer PR et al. NEJM. 2014;370: 2002-31 2. Puzziferri N etal. JAMA. 2014; 312:934-42 Meta-analysis RCTs (3 studies, 41 pts)showed remission of OSA in 95% of pts withRYGBMeta-analysis observations trials (29 studies,9844 pts) showed remission of OSA in 95%RYGB, 71% AGB, 91% SGChang S-H. JAMA Surg; publishedonline Dec 18, 2013. SOS Prospective Controlled Trial4047 obese subjects followed on average10.9 years, vital status known on all but 3Unadjusted HR for death 0.76 (surg vscontrol)Adjusted HR 0.71Death from MI 13 vs 25Death from cancer 29 vs 47Sjostrom L. NEJM 2007; 357:741528
10/16/2014 Perioperative mortality 0.1-0.3%Pulmonary embolism, anastomotic leaksWound infections, bleeding, incisional andinternal hernias, SBO, ulcers, stricturesNausea and vomitting after restrictiveprocedures (50%)Dumping syndromeVitamin deficienciesDietary changesNutritional deficienciesMedicationsContraception9
10/16/2014 Often start on full liquid diet in initial dayswith adequate protein.Diet gradually advanced to small, soft meals.Eat slowly and chew thoroughly. Stop eatingonce satiety reached.Gradually re-introduce regular foods in smallamounts. Avoid a lot of liquid calories.Ideal protein intake 1-1.5g/kg ideal weightdaily.Multivitamin with minerals to supplementvitamin A, B1, E, K, iron, folic acid, zinc,copper, selenium, biotinCalcium citrate 1200-1500mg/dayVitamin D3 800 units/dayIron supplement (beyond MVI) if deficientVitamin B12 500-1000mcg dailyMonitor progress with weight loss and anycomplications each visitLabs 3, 6 and 12 months then annuallyCBC, BMP, LFTs, Iron studies, B12, folate,Lipids, vitamin D 25-OH, PTHThiamine, zinc, copper, selenium withspecific findings24 hour urine calcium at 6 mo and 1 yearBone density at 2 years10
10/16/2014 Diabetes: rapid changes in insulin/diabetesmedication requirements. Require frequentmonitoring and adjustment of meds.Adjust doses of anti-hypertensivesConsider stopping medications for GERDAvoid enteric-coated or controlled-releasemedications (esp RYGB)Avoid NSAIDs post-operativelyFertility often increases after bariatric surgeryWomen counseled to delay pregnancy for 1218 months (during period of rapid weightloss)Malabsorption of oral contraceptives mayreduce efficacy: non-oral formsrecommendedEvaluate for nutritional deficiencies beforepregnancyEconomic modeling using insurancedatabases and clinical studiesMatched cohorts look at health careutilization for groups that undergo weightloss surgery vs medical interventionsIncremental cost-effectiveness ratios (ICER) –cost per QALY11
10/16/2014 British NHS: 20 year economic model predicts 2000-4000 per QALY gained ( 3300-6600). US economic model based on 5 year post-opinsurance data: 25,000 cost for bariatric surgery (2 mo post-op) Cost savings begin 3 months post-op Total surgery costs fully recovered by 53 months Australian Trial of diabetic patients - 1775lifetime savings, 1.2 QALYs gained (3)1. Picot J et al. Health TechAssessment. 2009; 13. 2.Cremieux PY et al. Am J ManagedCare. 2008; 14. 3. Keating C etal. Diabetes Care 2009; 32. Legacy Weight and Diabetes InstituteOHSU Bariatric Surgery ProgramSalem Hospital Bariatric Surgery CenterOregon Bariatric Center – PeaceHealth, EugeneInitial education sessionEvaluation by multi-disciplinary team (surgeon,dietician, physical therapist, psychologist, NP/PA)Typically process takes 2-6 monthsFollow up visits post surgery: 4-6 in first yearthen annually thereafter45 yo woman with BMI 40kg/m2 (weight278#)Diabetes on 55 units of lantus, 15 units oflispro QAC, exanitide, metformin.Hemoglobin A1C 9.2%Hypertension, hyperlipidemia, physicallyinactive with worsening back and leg pain.12
10/16/2014 Underwent RYGB March 2013.Weight 278 209 over first year. BMI now 30.Diabetes – Lantus down to 30 units andlispro 5 units QAC, off exanitide. A1C 7.7%(down 1.5%).Blood pressure under better control, 1 fewermedicationLess pain, more physically active, now able totake foster children into her home.Thank you for your attention!13
OHSU Bariatric Surgery Program Salem Hospital Bariatric Surgery Center Oregon Bariatric Center -PeaceHealth, Eugene Initial education session Evaluation by multi-disciplinary team (surgeon, dietician, physical therapist, psychologist, NP/PA) Typically process takes 2-6 months Follow up visits post surgery: 4-6 in first year then annually .