Transcription
BARIATRICSURGERYREGISTRY2019/2020ANNUAL REPORT
StatementThis publication was produced by the Bariatric Surgery RegistrySuggested CitationBackman B, Brown D, Cottrell J, Campbell A, Clancy W, Halim Shah Y J, ChadwickC, Budin A, MacCormick A, Caterson I and Brown W. The Bariatric Surgery RegistryAnnual Report, 2020. Monash University, Department of Epidemiology and PreventiveMedicine. August 2020, Report No. 8Data AnalysisMs. Dianne Brown (Team Lead)Mr. Angus Brian CampbellMr. William ClancyDr. Yazmin Johari Halim Shah (EWL and TWL calculations)GraphicsMonash Print (Data Visualisation)Ms. Hayley Cottrell (Funders, Registry Timeline, Figure 2 Hospital Sites and SurgeonsRepresented in the Registry)EnquiriesAny enquiries or comments regarding this publication should be directed to:Bariatric Surgery RegistryMonash UniversityLevel 6, The Alfred Centre99 Commercial Road, Melbourne 3004Phone: 61 3 9903 0725Fax: 61 3 9903 0717med-bsr@monash.eduThe contents of this report may not be published or used without permission.Data PeriodThe data contained in this document was extracted from the Bariatric SurgeryRegistry as at 22 July 2020 but pertains to procedures that have occurred up to30 June 2020. As the Registry does not capture data in real time, there may bea lag period between the occurrence of an event and its capture in the Registry’sdatabase, BSR-i.Original release December 2020.Amended May 2021.
CONTENTSWHO WE AREPurposeBenefitsFundersData CustodianAcknowledgement Of Country444455PATIENT REPORTED OUTCOME MEASURES (PROMs)Progress to DateFuture R’S REPORT6COMMITTEES AND STAFF51EXECUTIVE NTRODUCTION8LIST OF TABLES54LIST OF FIGURES55APPENDIX 1: DATA ELEMENTS CAPTURED56APPENDIX 2: DATA COMPLETENESS57Registry TimelineGovernanceEthical ReviewData Reporting891010DATA CAPTURE AND QUALITY11Eligibility Of ParticipantsData CaptureData ValidationMissing Data11111111APPENDIX 3: LIST OF HOSPITAL SITESREPRESENTED IN THIS REPORT5812APPENDIX 4: LIST OF HOSPITAL SITESWITH ETHICS APPROVAL59REGISTRY OVERVIEWSite And Surgeon AccrualEnrolment In The RegistryAUSTRALIA ANALYSISEnrolment In The RegistryDemographicsProcedures Captured By The RegistrySafety ReportingPeri-Operative Defined Adverse Events And ComplicationsDeathsWeight OutcomesDiabetes OutcomesFollow UpNEW ZEALAND ANALYSISEnrolment In The RegistryDemographicsProcedures Captured By The RegistrySafety ReportingPeri-Operative Defined Adverse Events And ComplicationsWeight OutcomesDiabetes OutcomesFollow liaNew ZealandAustraliaNew Zealand58585959APPENDIX 5: REGISTRY’S PUBLICATIONS,PRESENTATIONS AND APPENDIX 6: REFERENCES6060606061
WHO WE AREPurposeWithin the remit of a clinical quality registry, the Bariatric Surgery Registry seeks to answer the following:a.Is bariatric surgery safe? andb.Is bariatric surgery effective?To ensure that these questions can be addressed, the Registry has been designed with the underlying principle to provide datathat is accurate, complete and valuable. Accuracy and completeness is controlled by the definition, collection, verification,storage, and analysis and reporting as outlined in the Registry’s Data Governance Framework.BenefitsThe Registry continues to encourage high-level stakeholder engagement and facilitates collaborations with governments,surgeons, private health groups, individual hospitals, medical technology and device industries, private health insurers andmedical defence organisations to ensure that the data remains valuable.Most importantly, the Registry engages with participants to address how the Registry can aid in decision-making, assessment ofrisk and on-going journey of treatment. The involvement of the participants is paramount in regard to the data collection whichthe Registry strives to achieve, especially the annual follow up data.FUNDING PARTNERSThe Bariatric Surgery Registry received funding in the last 12 months from the Commonwealth Government of Australiaand the following supporters:The Registry would like to acknowledge and thank Medtronic for providing the start-up funding required for the New Zealandarm of the Registry.The Registry also looks forward to welcoming Johnson & Johnson in the 2020/2021 financial year as Platinum Sponsors.4Bariatric Surgery Registry Eighth Annual Report: 2019/20
DATA CUSTODIANThe Registry Custodian is the School of Public Health and PreventiveMedicine (SPHPM) within the Faculty of Medicine, Nursing and HealthSciences at Monash University.ACKNOWLEDGEMENT OF COUNTRYThe Bariatric Surgery Registry acknowledges the Traditional LandCustodians of Australia and we pay our respects to ancestorsand Elders, past, present and future for the Aboriginal and Torres StraitIslander peoples of Australia. We welcome all Aboriginaland Torres Strait Islander peoples to our Registry.In recognition that we are a bi-national registry, the Bariatric SurgeryRegistry acknowledges Māori as Tangata Whenua of Aotearoa NewZealand and as Treaty partners with the Crown.The Registry collects, stores and uses health data of Indigenousparticipants with the upmost respect and integrity.
CHAIR’S REPORTPROFESSOR IAN CATERSONThis is the eighth report of the Bariatric Surgery Registry (BSR). It continues to grow at a rapid pace and we now have surpassed90,000 participants. For the reporting year, we present a total of 90,457 participants and 197 surgeons and 133 hospitals arerepresented in this report.We continue our success in data collection from New Zealand, with the inclusion of 1,519 participants since May 2018. Over thenext 12 months, we need to continue our focus on strengthening this activity and ensure the continuing contribution to the Registry.We are really grateful for the ongoing work carried out daily by the staff in the Registry, by surgeons, by the staff in their rooms andin theatres, their hard work, expertise and continuing interest. The Registry can only be as good as the data it gets.We are committed to getting good long-term follow-up. Please, continue to help us to get this data.There continues to be interest in our Registry, its data and potential. This interest ranges from government to internationalcollaborators and because we have made as sure as we can that the data is collected properly, that we do have involved surgeonsand staff, we are seen as trustworthy and our data output useful.We look forward to the next 12 months with the focus on producing outputs on the effectiveness of bariatric surgery in ourcountries. We are happy to receive research proposals for use of de-identified data and we have established a process for dealingwith these requests.Once again, we must thank the staff of the BSR – they continue to deal with problem issues calmly and efficiently, they are reallyinvolved and so helpful.Thank you all.Professor Ian D CatersonDirector, Boden Institute, Charles Perkins Centre, University of SydneyDirector, Charles Perkins Centre Royal Prince Alfred ClinicPast-President, World Obesity Federation6Bariatric Surgery Registry Eighth Annual Report: 2019/20
EXECUTIVE SUMMARYThe Bariatric Surgery Registry (BSR) is proud to present the Eighth Annual Report as at 30 June 2020.Within the latter half of this reporting year, bariatric surgery was greatly affected by contingencies put in place in response to theCOVID19 pandemic. This was true for both Australia and New Zealand and we observed a period of no bariatric proceduresperformed, unless in emergency cases. During this period, the Registry reached out to surgeons and their staff to help facilitatedata entry, reviewing outstanding operations and follow up for resolution and entry and providing data for review and/or researchwhere approved.During this period, the Registry also commenced additional data reviews and focused on validating participant reported data toensure that information housed within the Registry was both accurate and clinically relevant.The first portion of this report presents the Registry overall, exploring the Registry’s hospital site and surgeon coveragebinationally, as well as the overall total number of participants as at 30 June 2020. Following the overall presentation, the Registryhas reported Australia and New Zealand analysis results individually, for the first time. In addition to the individual countrypresentation, the Registry also presents data specific to the common procedure types collected by the Registry: laparoscopicadjustable gastric banding (LAGB), laparoscopic sleeve gastrectomies (LSG) and bypasses (one anastomosis gastric bypass(OAGB) and Roux-en-Y gastric bypass (RYGB)).Despite the presentation of country specific results, the Registry has observed similar trends to what it has reported in previousyears: The new cohort of participants remains predominately female; Over 90% of primary procedures occur in private hospitals in Australia and over 70% of primary procedures in privatehospitals in New Zealand; During the FY19/20 period in Australia, 2.1% of primary procedures and 7.6% of revision procedures had a definedadverse event. For New Zealand, 9.9% of primary procedures and 22.6% of revision procedures had a definedadverse event; and A significant shift in diabetes status from baseline to 1-year post-operative was observed for both Australia and NewZealand. There was also a large reduction in treatment rates at 12 months after surgery to that recorded at baseline.In addition to the noted trends above, the Registry has had a very successful reporting period, where milestones were activelyachieved, namely: A total of 90,457 participants as at 30 June 2020 including the addition of 19,489 new participants in the past year; 197 surgeons from 134 hospitals are represented in this reporting period; 70% MBS capture achieved so far for the FY19/20 period; Commenced the Patient Reported Outcome Measures (PROMs) project; and Supported the continued growth in participation of hospital sites and surgeons from Australia and New Zealand.ACKNOWLEDGEMENTThe Bariatric Surgery Registry recognises the commitment of its participating surgeons. Their involvement demonstrates the veryessence of being a health professional with their commitment to integrity, a high standard of performance, and the public whomthey serve. These surgeons and their dedicated support teams make time to regularly submit vital information to this study,willingly sharing their successes and the management of their patients’ complications.With their data, the Registry is able to offer the confidence necessary for making decisions about the provision of bariatricsurgery in Australia and New Zealand to the benefit of all stakeholders, but most importantly for those afflicted with obesity whomay be considering their treatment options. By taking part in the Bariatric Surgery Registry, participating surgeons are ensuringa high standard of care for bariatric patients. They are owed a debt of sincere gratitude.Bariatric Surgery Registry Eighth Annual Report: 2019/207
INTRODUCTIONRegistry Timeline2009With recommendations featured in the GeorganasReport, OZZANZ (now ANZMOSS) identified theneed for a Registry to track outcomes of bariatricsurgery.2010Monash University was announced as the partnerand Registry custodian for the Bariatric SurgeryRegistry in Australia and New Zealand.2012The Registry commenced as a pilot project withinVictoria. Seed funding was provided by OZZANZ aswell as industry partners Applied Medical, AllerganHealth, Johnson & Johnson and GORE.A governing Steering Committee with anIndependent Chair was formed with a wide rangeof representation.2014After the success of the pilot project, funding wassecured from the Commonwealth’s Department ofHealth to roll out the Registry nationwide with 118surgeons registering their interest to participate. Atthe end of 2014 there were 42 surgeons from 33hospitals actively contributing to the Registry.2016The Registry successfully operates in VIC, NSW,QLD, SA, WA and TAS.The New Zealand arm of the Registry commenceswith the support of funding provided by industry.20172018With the ongoing, and valued funding support ofthe Registry’s industry partners, the first participantis successfully enrolled into the Registry in NewZealand and active data collection commences.The Registry celebrates surpassing 50,000participants enrolled in the project.2019By mid-2020, the Registry successfully surpassed90,000 participants while continuing to providereporting and feedback on the safety, quality andefficacy of bariatric surgery in Australiaand New Zealand.The ongoing and invaluable support continues fromthe Commonwealth's Department of Health,ANZMOSS and industry partners Applied Medical,Medtronic, GORE, Johnson & Johnson and AVANT.8The Registry successfully secured a 5 year fundingagreement with the Commonwealth’s Departmentof Health to continue the success of the project inAustralia.Bariatric Surgery Registry Eighth Annual Report: 2019/202020The Registry successfully surpassed the enrollmentof 80,000 participants by the end of 2019 with 216surgeons having contributed from 134 hospitalsacross Australia and New Zealand. The project nowcovers all states and territories across Australia.A project focused on Patient Reported OutcomeMeasures (PROMs) commences within the Registrywith intentions to standardise questions for futureroutine collection.
GovernanceThe Registry aligns with the fundamentals detailed in the ‘Operating Principles and Technical Standards for Australian Clinical QualityRegistries 2008’ and the ‘Framework for Australian Clinical Registries 2014’ as published by ACSQHC. This is to ensure that, as aRegistry, it aligns and complies with the national standard and provides assurance to all stakeholders.The Registry is governed by the Steering Committee and this has convened since 2012, chaired by an independent obesity expert,Professor Ian Caterson. The Committee meets on a quarterly basis to advise the Registry on matters such as strategic direction,financial budget, data access, clinical quality and safety, quality development and operations. The BSR Programme Manager,in consultation with the Clinical Director for Australia, Professor Wendy Brown and the Clinical Lead for New Zealand, AssociateProfessor Andrew MacCormick, oversee the day-to-day operations of the Registry.Current membership includes representatives from the following organisations and/or societies: Monash University Australian and New Zealand Metabolic and Obesity Surgery Society (ANZMOSS) Royal Australasian College of Surgeons (RACS) Australia and New Zealand Gastro-Oesophageal Surgical Association (ANZGOSA) University of Auckland Medical Technology Association of Australia (MTAA) Australian Commonwealth Department of Health Community RepresentationOne of the key achievements of the Steering Committee has been the establishment of the Data Governance Framework and theassociated policies and processes that underpin the Registry including:Study ProtocolData DictionaryOutlier Policy (currently under development)BSR-i Business RulesPrivacy PolicyData Element Variation ProcessesGrievance & Complaint PolicyData Capture Variation ProcessesCall Centre Protocol & ScriptsBSR-i System Change Request ProcessesData Access & Reporting PolicyReporting TemplatesMONASHPUBLIC HEALTHAND PREVENTIVEMEDICINEBariatric Surgery Registry Eighth Annual Report: 2019/209
Ethical ReviewThe Bariatric Surgery Registry was established for the purpose of improving the quality and safety of bariatric surgery and it isconsidered to be in the public’s interest.To function as a clinical quality registry, the Bariatric Surgery Registry collects, stores, and uses identifiable, personal and sensitivehealth information about bariatric patients for research into the quality, safety and effectiveness of bariatric surgery as treatment forobesity.To date, 40 Australian human research ethics committees (HRECs) have approved the study and certified that it meets therequirements of the National Statement on Ethical Conduct in Human Research (2007). New Zealand’s Southern Health andDisability Ethics Committee approved the study in accordance with the requirements of the Ethical Guidelines for ObservationalStudies: Observational Research, Audits and Related Activities (2012). Amongst the 157 hospital sites across Australia and NewZealand which had been approved as at 30 June 2020 to participate in the Registry, 133 are represented in this report.Data ReportingThe Registry follows a reporting cycle throughout the year to provide valuable data back to the key stakeholders. These reports include:Released to:Report TypeReportingPublicAnnual ReportAs at 30 June each yearPublicSemi-Annual UpdateAs at 31 December each yearSurgeonIndividual Surgeon ReportsAs at 30 September each yearDevice Manufacturer (Funder)Individual Industry ReportsAs at 31 March each yearHospital Group (Participant)Hospital Group ReportsAs at 31 March each yearThe Registry also publishes a quarterly newsletter that is distributed to all internal and external stakeholders, hospitals and surgeonsas well as potential new hospitals and surgeons that the Registry will seek to recruit. This newsletter is also published on the Registry’swebsite for participants to access.10Bariatric Surgery Registry Eighth Annual Report: 2019/20
DATA CAPTURE AND QUALITYEligibility of ParticipantsAnyone who undergoes bariatric surgery for the treatment for obesity in Australia or New Zealand is eligible for inclusion in theBariatric Surgery Registry.Data CaptureSurgeons or hospital data collectors provide data about the patients and their procedures using one of the following options: Web browser with secure authorised entry using the Registry Interface (BSR-i); or Paper based data forms (secure fax or posted)Upon receipt of this information, the Registry sends the bariatric patients a Participant Fact Sheet that details the Registry and whatparticipation entails. The patient has a two-week period to opt-out of the Registry by calling a Free-call 1800- number. Patients havethe option to completely opt-out, meaning that no data is held in the Registry other than that needed to identify them in the futureshould they have another procedure, or partial opt-out, meaning that they will allow their data to be held in the Registry but they donot wish to be called or contacted by the Registry. Participants have the right to opt-out at any stage during the follow-up period.To ensure that all bariatric procedures are captured, the Registry engages with the Hospital Information Services (HIS) at eachhospital site to provide regular ICD-10 coding (ACHI codes) reports for bariatric procedures performed by surgeons who participatein the Registry. These reports are used to verify data submitted by surgeons/ hospital data collectors and are used as the primarysource of data if the surgeon and/or hospital has not previously provided information.Surgeons or public hospital clinics provide follow-up data, either by return of a paper form or through submission on the BSR-i. Ifsurgeons and/or public data collectors indicate they have not seen the participant, the Registry’s Call Centre will attempt to contactthe participant.Data ValidationData validations and quality checks are performed on a monthly and quarterly basis to ensure the timely review and correction ofdata if required. These processes are to ensure information received is clinically correct and is recorded correctly in the BSR-i.Data validation processes include cross checking with hospitals, surgeons and/or participants to ensure that the Registry maintainsthe highest level of data integrity.Missing DataThe need for near complete data capture is required to ensure the reliability of the Registry. The collected data provides informationon the patient (to allow tracking and to identify risk factors), the patient’s weight and BMI, the patient’s health (diabetes status andtreatment), the type of surgery undertaken, whether a concurrent liver or renal transplant took place, the device utilised, the need forrevision or repeat surgery, unplanned admissions to ICU or readmissions to hospital as well as mortality.Missing data for most of the data elements collected is kept to a minimum. The Registry periodically validates and cleans theinformation submitted to ensure that data verification is complete and the data collated is accurate in nature.The minimum data set can be reviewed in Appendix 1. A data completeness report of the minimum data set is presented inAppendix 2 of this report.Bariatric Surgery Registry Eighth Annual Report: 2019/2011
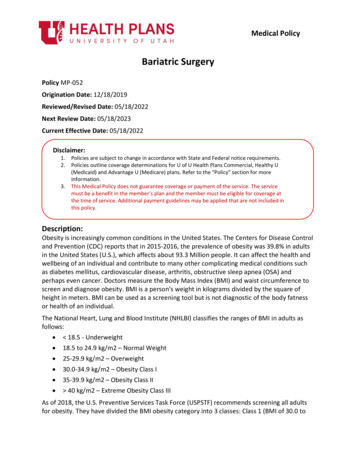
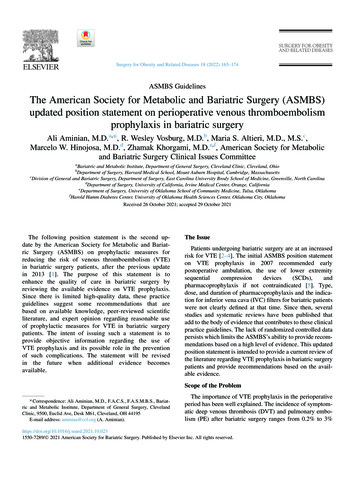
REGISTRY OVERVIEWSite and Surgeon AccrualThe pilot registry commenced in 2012 at three sites in Victoria. Since that time, the Registry has grown to include 184 surgeonsin Australia and 13 in New Zealand actively contributing.Figure 1 illustrates this growth across Australia and New Zealand since the commencement of the Registry. Over the past 12months, there has been an 13.6% increase in hospital site representation across Australia and New Zealand to 133 alongside197 surgeons represented.FIGURE 1 – SURGEONS AND HOSPITAL SITES REPRESENTED IN THE REGISTRY PER FINANCIAL 69810095982016/20172017/2018735550229012Prior to 20142014/20152015/2016Bariatric Surgery Registry Eighth Annual Report: 2019/202018/20192019/2020
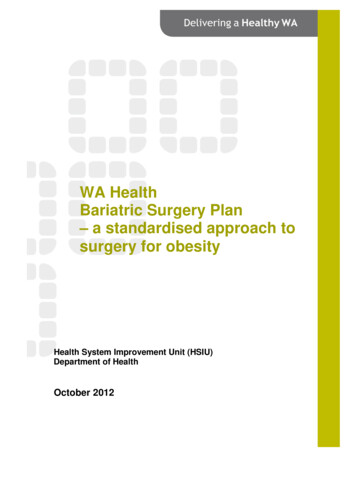
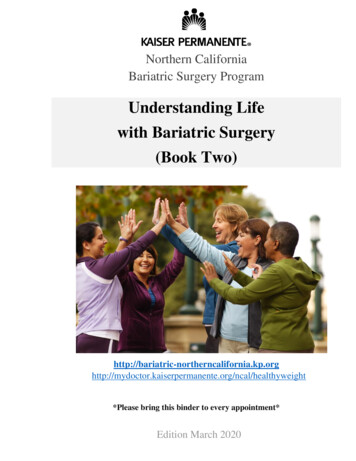
FIGURE 2 – NUMBER OF HOSPITAL SITES AND NUMBER OF SURGEONS PER STATE CONTRIBUTING TO THE REGISTRY FOR FY 4289553951463334461237101117613608* Please note there are 5 surgeons in Australia that contribute to the Registry in multiple states.** South Australia and Northern Territory as well as New South Wales and the Australia Capital Territory are displayed as combined totals in Figure 2.Bariatric Surgery Registry Eighth Annual Report: 2019/2013
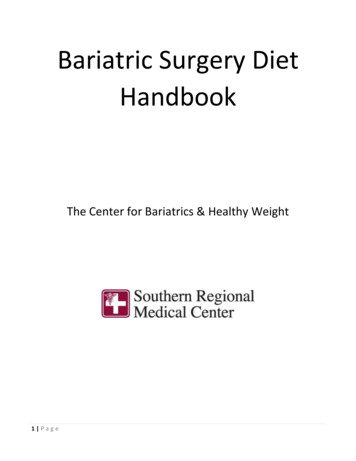
Enrolment in the RegistryRecruitment commenced as of February 2012 in Australia and May 2018 for New Zealand. For a patient to receive a ParticipantFact Sheet, they must have had their procedure on or before 30 June 2020.As at 30 June 2020, the Registry confirmed the participation of 90,457 bariatric patients and their data and it is from this cohortthe report is derived. A further 2,533 bariatric patients (2.72%) have chosen to opt out and are not represented in this report.Table 1 demonstrates the growth of the Registry from 1 February 2012 to 30 June 2020. In the past financial year, there was a27.4% increase in the number of participants reported and the Registry continues to maintain an opt out rate of below 4%.TABLE 1 – CUMULATIVE PATIENT PARTICIPATION IN THE REGISTRY SINCE COMMENCEMENT IN FEBRUARY 2012ParticipatingOpt OutOpt Out RateAs at30 June 2015As at30 June 2016As at30 June 2017As at 30June 2018As at 30June 2019 As at 30June 2020 982,3402,5333.5%3.4%3.8%3.77%3.16%2.72%* includes 223 participants who only had an abandoned procedure includes Australia and New Zealand participantsThere have been some notable trends observed since the national roll out in 2014 including steep uptake of sleeve gastrectomyprocedures that continues to increase as well as the emergence of bypass procedures. Figure 3 illustrates the accumulation rate ofparticipants in the Registry by type during this period.FIGURE 3 – ACCUMULATION RATE OF PARTICIPANTS IN THE REGISTRY BY PATIENT TYPE FROM FEBRUARY 2012 TO 30 JUNE 202010000090000800007000060000LEGACY PARTICIPANTPRIMARY PARTICIPANT WITH 'OTHER' PROCEDURE50000PRIMARY PARTICIPANT WITH BYPASSPRIMARY PARTICIPANT WITH SLEEVEPRIMARY PARTICIPANT WITH iatric Surgery Registry Eighth Annual Report: 2019/202017201820192020
AUSTRALIAANALYSISBariatric Surgery Registry Eighth Annual Report: 2019/2015
Enrolment in the RegistryRecruitment commenced in Australia as of February 2012 and has continued to increase each reporting period.As at 30 June 2020, the Registry confirmed the participation of 88,938 bariatric patients in Australia and it is from this cohort thereport is derived. A further 2,518 bariatric patients (2.75%) have chosen to opt out and are not represented in this report.TABLE 2 – PATIENT PARTICIPATION FOR AUSTRALIA AS AT 30 JUNE 2020As at 30 June 2020 Participating88,938*Opt Out2,518Opt Out Rate2.75%* includes 104 participants who only had an abandoned procedureDemographicsAs consistently reported by the Registry, bariatric procedures are performed predominantly on female participants in private hospitalsin Australia.The distribution of sex in primary and revision procedures also shows a similar trend where females account for 78.0% of all primaryprocedures and 84.0% of revision procedures, males account for 22.0% of primary procedures and 16.0% of revision procedures.Table 3 demonstrates the key demographic indicators of participants enrolled in the Registry who have had a primary procedurein the last financial year (2019/20), with comparisons between primary procedures types as well as private and public hospitalprocedures.The mean age for primary procedures was 42.4 years old with females (41.8), on average, slightly younger than male (44.3)participants with primary procedures.TABLE 3 DEMOGRAPHICS OF PRIMARY PARTICIPANTS AT THEIR PRIMARY PROCEDURE IN AUSTRALIA (FY19/20)All PrimaryProceduresPublic PrivateMALEFEMALEALLProcedureNumber757Band PrimaryProceduresAll12,962 13,719Public PrivateSleeve PrimaryProceduresAllPublic Private4422727154410,677 11,221Public PrivateAll1662,0012,167FemaleUndergoingProcedure %78.6%78.1%MaleUndergoingProcedure %21.3%21.8%Min Age at Mean Age at Max Age at Min Age at Mean Age at Max Age at Min Age at Mean Age at Max Age at * p-value 0.001 (Two-sample t-test) statistically significant difference in mean age at operation between males and females** Bypass includes both Roux-en-Y gastric bypass and one anastomosis gastric bypass procedures16AllBypass PrimaryProcedures**Bariatric Surgery Registry Eighth Annual Report: 2019/20
TABLE 4 – PERCENTAGE OF FEMALE VS. MALE PARTICIPANTS HAVING A REVISION PROCEDURE IN AUSTRALIA (FY19/20)All Revision ProceduresPublicPrivateAll34534653810Female Undergoing Procedure %81.4%84.3%84.0%Male Undergoing Procedure %18.6%15.7%16.0%Procedure NumberFigure 4 and 5 illustrate the age range of both primary and revision participants at the time of procedure during the last financial year(2019/20)FIGURE 4 PARTICIPANTS’ AGE DISTRIBUTION AT TIME OF PRIMARY PROCEDURE IN AUSTRALIA 0.1%Male20-243.0%5.1%FemaleUnder200.6%1.0%75 0.1%FIGURE 5: PARTICIPANTS’ AGE DISTRIBUTION AT TIME OF REVISION PROCEDURE IN AUSTRALIA 92.3%3.7%Female45-4950-5455-5960-6465-6970-7475 Bariatric Surgery Registry Eighth Annual Report: 2019/2017
Procedures Captured by the RegistryOverviewFigure 6 maps out the weight distribution of both primary and revision participants at the time of surgery. Whilst primary participantsdo make up the majority of the cohort captured by the Registry, they also typically have a higher weight at operation than thoseparticipants undergoing a revision procedure.FIGURE 6 PARTICIPANTS’ WEIGHT AT TIME OF PROCEDURE IN AUSTRALIA (FY19/20)Weight 0.0%0.0%240-2490.0%0.0%250-2590.0%0.0%260 0.5%In total, the Registry has captured 97,007 procedures completed on 88,938 participants in Australia, however this excludes 104participants who have only had an abandoned procedure. The Registry has captured a total of 222 abandoned procedures from104 participants since February 2012. 32 of those abandoned procedures occurred in the last FY19/20.Table 5 demonstrates the total capture of procedures by the Registry as at 30 June 2020 and the FY19/20. The Registrysuccessfully captured 14,869 of the 21,315 procedures recorded by the MBS. The Registry has camptured 70% of bariatricprocedures as recorded by the data for the FY19/20.TABLE 5 PROCEDURES PERFORMED BY TYPE IN AUSTRALIATotal BSR(Feb 2012 to 30 June 2020)Gastric Band (LAGB)Sleeve gastrectomy (LSG)BSR FY 19/20(1 July 2019 to 30 June 2020)PrimaryRevisionTotalPrimaryRevisionTotal(Est of % collectedin 2,95711,22162211,843Roux-en-Y Gastric Bypass (RYGB)45934687928010519321983One anastomosis gastric bypass 120102222161632Surgical Reversals of BandsOther ProceduresTotal Procedures (excl Abandon)Abandoned Procedures*MBS data includes only LAGB, LSG, RYGB and OAGB procedures in private hospitals18MBS Data*FY 19/20Bariatric Surgery Registry Eighth Annual Report: 2019/2079.7%NA
The types of
Bariatric Surgery Registry Eighth Annual Report: 2019/20 7 EXECUTIVE SUMMARY The Bariatric Surgery Registry (BSR) is proud to present the Eighth Annual Report as at 30 June 2020. Within the latter half of this reporting year, bariatric surgery was greatly affected by contingencies put in place in response to the COVID19 pandemic.