Transcription
G A S T R O E N T E R O L O G Y Inside This Edition1Message from the Chief2Changing the Paradigm: Living-DonorLiver Transplantation4Virtual Patient Software: UntappedTechnology for PracticingGastroenterologists6Robotic Repair of GiantParaesophageal Hernia9News & Updates10Schistosomiasis: Diagnosis andMessage From the ChiefI grow old I grow old I shall wear the bottoms of my trousers rolled.Shall I part my hair behind? Do I dare to eat a peach?I shall wear white flannel trousers, and walk upon the beach.I have heard the mermaids singing, each to each.I do not think that they will sing to me.The Love Song of J. Alfred Prufrock, by T. S. EliotTreatmentCME CreditDisclosures: Drs. Bataller, Behari, Bettner, Dugum,and Klinge have reported no relevant relationships withentities producing health care goods or services.Instructions: To take the CME evaluation and receivecredit, please visit UPMCPhysician Resources.com/GI,and click on Gastroenterology Digest, Spring 2018.Accreditation Statement: The University of PittsburghSchool of Medicine is accredited by the AccreditationCouncil for Continuing Medical Education (ACCME) toprovide continuing medical education for physicians.The University of Pittsburgh School of Medicinedesignates this enduring material for a maximum of.5 AMA PRA Category 1 Credits . Each physicianshould only claim credit commensurate with the extentof their participation in the activity. Other health careprofessionals are awarded .05 continuing education units(CEU), which are equivalent to .5 contact hours.Aging. As expressed so eloquently in this excerpt, aging is replete with “come downs,” including amarked inability to do what you did before — thinning hair, shrinking posture with pants that aretoo long, teeth and musculature that don’t permit the elegant gnashing of a piece of fruit, orruefully and tellingly, the loss of appeal to mermaids.The number of Americans ages 65 and older is projected to more than double from 46 million toover 98 million by 2060. Accompanying the aging of our society will be significant increaseddemand for nursing homes and huge increases in those living with dementia. The AmericanGeriatrics Society estimates we will need about 30,000 geriatricians by 2030, yet there are onlyabout 7,000 currently practicing. Geriatrics is among the lowest paying specialties and isdistinctive in being the only medical specialty I know of which results in a decrement in incomewith more training – geriatricians make on average about 20,000 LESS than internists every year.Why do extra training to earn less? It’s not a model primed for success. The aging of the GI tract isanother mystery. There are certainly no outward manifestations of aging on endoscopicexamination – the 100 year-old colon looks similar to the teenager’s. And, even in function, it’shard to identify a decrement in GI tract function with time.Fortunately, the indignity of aging is counter-balanced by the repose and wisdom that comes withit. Also, there is no doubting that resources and commitment to studying aging will necessarily andrapidly expand in the future. It is my great pleasure to introduce another edition of Digest, whichwe hope will never grow old and will continue to inform and inspire. Thanks again for joining us.To good health,Robert E. Schoen, MD, MPHProfessor of Medicine and EpidemiologyChief, Division of Gastroenterology, Hepatology and NutritionAffiliated with the University of Pittsburgh School of Medicine,UPMC Presbyterian Shadyside is ranked among America’sBest Hospitals by U.S. News & World Report.DIVISION OF GASTROENTEROLOGY, HEPATOLOGY, AND NUTRITIONDIGESTSPRING 2019
Evaluating Potential LivingLiver DonorsCompared to other nations, the United States performs very few living-donor liver transplants and ahigh percentage of deceased-donor transplants. This standard has continued for decades, despite alarge body of evidence that speaks to the benefits of living donation. But as the discrepancy growsbetween the number of patients on the waiting list and the number of available deceased-donorlivers, living donation is a safe and viable way to expand the donor pool.Changing the Paradigm: LivingDonor Liver Transplantation Living donor surgery, just like any surgery,does present some level of risk. This risk,along with certain rare but highlypublicized tragedies, is another reason thatU.S. transplant centers have been slow toadopt living donor transplantation.Minimizing risk for living donors is a keypart of any living donor transplant program,and findings from the National Institutes ofHealth show that living-donor livertransplant outcomes improve with centerexperience. The experience of the UPMCtransplant team has allowed us tosuccessfully pursue living donation whileprotecting donors by investing in a rigorouspre-operation evaluation process.· HIV· Ongoing substance abuse·C ancers or other major health conditionsor diseases that could complicate surgeryWhile the risks for donors are evident, justas they would be in any surgery, it’simportant that we allow our patients todecide how they want to move forward.Rather than eliminating the option ofliving-donor liver transplantation, it’simportant for physicians to decide the bestcourse of action alongside their patient.That’s why, at UPMC, we discuss livingdonor transplantation with every patientwho will benefit from a liver transplant.We hope to change the paradigm in theUnited States, to educate patients andphysicians about pursuing living donortransplantation not as a last resort, but as afirst-line treatment option for every patienton the liver transplant waiting list.For more information about living donationand how to begin the referral process atUPMC, please visit UPMC.com/LiverTransplantReferral. The most impactful benefit for thetransplant community comes from theliving donor themselves. When a livingdonor volunteers to donate to a lovedone, they bring a new liver into the organpool and reduce the demand for deceaseddonor livers.At UPMC, we believe in the power of livingdonation to save lives. Our main criteria fordetermining if a patient should pursue livingdonor transplantation are that they willexperience a greater survival benefit witha liver transplant than any other treatmentand that they have identified a suitable,willing donor.· Heart diseaseD I V I S I O N O F G A S T R O E N T E R O L O G Y, H E PAT O L O G Y, A N D N U T R I T I O NGASTROE NTE ROLOGY DIG ESTAt UPMC, our mission is to offer earlyaccess to transplant for patients on the livertransplant waiting list. We considerliving-donor liver transplantationa first-line option, rather than a last resort,for patients on our liver transplant waitinglist. In both 2017 and 2018, we performedmore than 50 percent of our liver transplantswith living donors.Other benefits include fewer instances ofpostoperative complications, the ability toovercome MELD limitations, and theincredible opportunity for family, friends,and the community to be part of saving alife. In many cases, because a living-donorliver transplant is a non-urgent procedure,the procedure can be scheduled well aheadof time, at the convenience of the patientand the living donor.The primary obstacle to increasing theavailability of living donor transplantation islack of awareness among both patients andphysicians. Many physicians are unfamiliarwith living-donor liver transplant or onlysee it as an option after all other treatmentshave been exhausted. Unfortunately, at thatpoint many patients have a MELD score sohigh that they will not experience the mostsalient benefits of a living donor transplant.· Liver diseaseOur experienced team of transplantsurgeons, hepatologists, nursecoordinators, and social workerscollaborate at every stage of the process toensure optimal outcomes for both patientsand donors. We are dedicated to spreadingawareness of and educating people aboutliving donation. Patients are listed based on their MELDscore, which predicts mortality while on thewait list. However, the MELD score hasseveral limitations. For patients listed witha low MELD score, a living-donor livertransplant may be their best and only option.Due to that shorter wait and the elective,non-emergent nature of a living donortransplant, patients can be transplantedbefore their disease has progressed to amore severe state, leading to improvedpatient and graft survival and reducedrecovery time when compared to deceaseddonor transplantation.Internationally, and especially in East Asiancountries like South Korea, China, andTaiwan, living donor transplantation isthe highest standard of care. But U.S.hospitals have been slow to adopt this,due to a few barriers.Living-liver donors should typically bebetween the ages of 18 and 55, have a BMIof less than 32, and be of generally goodhealth. They should have no history of thefollowing:32Swaytha Ganesh, MD, is the medical directorof the Living Donor Program at UPMC. She isrenowned for her clinical expertise in treatinga wide range of patients with liver diseasewith a specific interest in living-donor livertransplantation. Her areas of research includeevaluating recipients and donors and assessingtheir ability for living donor surgery anddeveloping disease management protocolsin post-liver transplant patients withmetabolic syndrome, hyperlipidemia, andsystemic hypertension.This organ shortage continues to grow.The median waiting time for a patient witha MELD of 29 has gone from 201 days in2014 to 691 days in 2014. Approximately20 percent of the patients on the listsuccumb to their disease prior to receivinga transplant, creating high waiting listmortality.Living-donor liver transplant has severalbenefits, including reduced time on thetransplant waiting list, early access totransplant giving these patients the bestchance of survival, immunologicaladvantages, and a shorter length of stayat the hospital post liver transplant.Why U.S. Hospitals PerformFew Living Donor TransplantsWith decades of experience performingliving-donor liver transplants, the UPMCLiver Transplant Program continues tolead the field by performing a higherpercentage of living-donor liver transplantsthan any other center in the United States.This allows us to address the particularlyacute shortage of deceased-donor liversin our distressed region and to meet theneeds of patients who travel to ourcenter for treatment from all around theUnited States. Abhinav Humar, MD, is the clinical directorof the Thomas E. Starzl Transplantation Instituteand chief of the Division of Transplantation inthe Department of Surgery at UPMC. Hisareas of research include partial liver transplantsand studies of hepatic regeneration, clinicaloutcome studies in kidney, liver and pancreastransplants, cytomegalovirus (CMV) diseasein transplant recipients, outcomes in pediatrickidney and liver transplants and smallbowel transplantation.First performed by Thomas E. Starzl, MD, in1967, liver transplantation offers thousandsof patients in the United States a secondchance at life. Although this is a life-savingprocedure, there is a large discrepancybetween the number of available deceaseddonor organs and the number of people onthe waiting list.Benefits of Living DonationAt UPMC, we believe the safety of livingdonors is of paramount importance. Everypotential donor undergoes a 1.5-dayevaluation including blood work, physicalexamination, psycho social evaluation,EKG, chest x-ray, CT scan, and MRI of theabdomen along with other testing. They areseen and evaluated by a multidisciplinaryteam including a hepatologist, a transplantsurgeon, an independent living donoradvocate, a nutritionist, a social worker anda living donor advocate.UPMC ExpertiseSPRING 2019Changing the Paradigm: Living-DonorLiver Transplantation
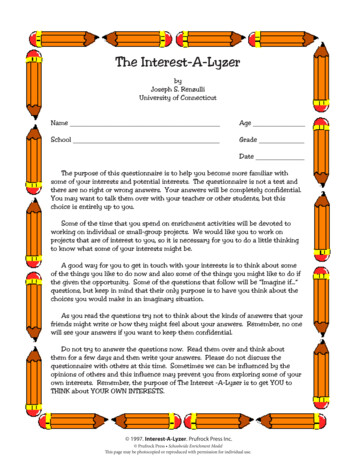
Awarded a Carnegie Science Award in 2018, James B. McGee, MD, has spent more than two decadesdeveloping technology to improve medical education for medical students and to make continuingmedical education more efficient for physicians. One of his most striking technological innovations isvpSim, a virtual patient software that can help medical students and practicing gastroenterologistsdevelop clinical decision-making skills in an engaging clinical context.GASTROE NTE ROLOGY DIG ESTEven early iterations of virtual patientsoftware, like the one developed by Dr.McGee at Harvard Medical School in 1996,displayed clear benefits of the simulatedclinical environment for student learners. Today, because of advancements intechnology, virtual patient software allowsfor even more complex and realistic patientscenarios. Dr. McGee’s most recent iterationof this software is called vpSim, a cloudbased platform that enables custom casesimulations on an easy-to-use interface.This software allows a clinician or medicalstudent to interview a patient virtually, makedecisions about diagnostic tests, determinea diagnosis, treat the patient, and thenJeffrey Dueker, MD, MPH, is a chiefgastroenterology fellow, Year III in theDivision of Gastroenterology, Hepatology,and Nutrition.An 86-year-old male with past medicalhistory for coronary artery disease, COPD,and prior heavy tobacco use presents to theemergency room with dysphagia to solidsand liquids. Further history from the patientis notable for immediate regurgitation of allliquids for the past few days, identifying aconcern for food impaction. He undergoesan esophagogastroduodenoscopy withremoval of a food bolus, followed bycomputed tomography (CT) without IVcontrast. An endoscopic picture from themiddle third of the esophagus after the foodbolus was removed is shown, as well as arelevant axial CT image.What is the explanation for this patient’sfindings? What are the recommendedtreatment strategies?Compare your answer to Dr. Dueker’s on page 11. “Virtual patient software allows a clinicianor a student to develop clinical decisionmaking skills in a safe environment andto get constructive feedback on realisticon-screen patient-management,” saysDr. McGee.Perhaps the most striking features ofcontemporary treatment of GI diseasesis the incredibly wide range of availabletherapies and the diversity of patientresponses to those therapies. For example,Dr. McGee recently treated a patient whowas experiencing severe diarrhea witha celiac disease-like clinical picture. Afterhis examination, Dr. McGee realized thatthis patient was actually suffering froman uncommon but serious side effect ofa particular cholesterol loweringmedication. Virtual patient software can beused to familiarize physicians with suchuncommon occurrences.CASE PRESENTATIOND I V I S I O N O F G A S T R O E N T E R O L O G Y, H E PAT O L O G Y, A N D N U T R I T I O N Seeing similar success with recentimprovements in technology, virtual patientsoftware is being adopted by medicalschools and professional societies aroundthe country, but there are still untappedopportunities to use virtual-patientsoftware in gastroenterology (GI)clinical environments.Virtual Patient Softwareand vpSimWhat Is This? 4In the early 2000s, online medical educationwas still in its infancy when Dr. McGeeestablished and became the first editor foronline education at the AmericanGastroenterology Association (AGA),identifying a need to curate, organize, andcarefully supervise online educationalcontent for gastroenterologists. “Today,online education is virtually taken forgranted, a sign of how successful work inthat area has been,” says Dr. McGee.Opportunities to Use VirtualPatient Software in GI ClinicalEnvironmentWith more dedicated use of virtual patienttraining with branching pathways, clinicianscan fine-tune their clinical decision-makingskills and, in time, may discover linkages tohighly-personalized genetic profiles. Tolearn more about the vpSim and virtualpatient simulation, visit Kynectiv.com.5[an image/screengrab of the software itself]Both the American Academy of Allergy,Asthma, and Immunology and theAmerican College of Physicians use vpSimto test and practice applying the clinicalknowledge of their members and toencourage them to integrate noveltherapies and guidelines into their practice.By situating learning in a patient-centeredcontext, simulation software creates a morerealistic, engaging, and memorableexperience, which physicians preferbecause it helps them to learn at a fasterpace. The addition of branched decisionmaking creates new opportunities for use inthe GI clinical environment.The future growth of virtual patientsoftware may have complementary successwith genetic science and precisionmedicine. It is likely that the patient’smedication reaction was caused byindividual genetic factors. Every year,researchers learn more about how specificgenetic profiles relate to the observedclinical state of a patient. This new geneticdata allows for gastroenterologists toprovide highly-personalized care that couldresult in more effective treatments. James B. McGee, MD, is director of theLaboratory for Educational Technology at theUniversity of Pittsburgh School of Medicine andan associate professor of medicine with theUniversity of Pittsburgh Division ofGastroenterology, Hepatology and Nutrition. Hewas awarded a Carnegie Science Award in 2018for his twenty years of innovative endeavors tobring technology into medical education.receive immediate feedback from a virtualonline expert. The main addition of vpSim tothe area of simulation is branched decisionmaking trees, which allow clinicians toexplore several diagnostic therapeuticpathways and receive feedback on theefficacy of each option relative to othertreatments. This software is now used inmedical schools and professional settingsall around the country because it provides anew way of learning, not through rotememorization and repetition, but bygrounding learning in a clinical, patientfocused context.SPRING 2019Virtual Patient Software: Untapped Technologyfor Practicing Gastroenterologists
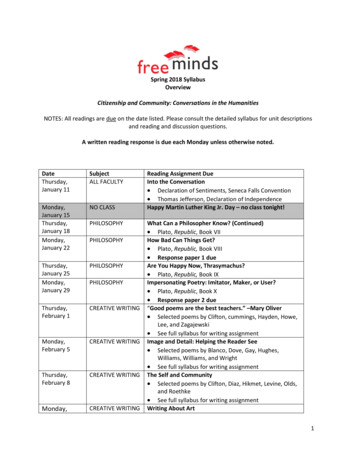
SPRING 2019Robotic Repair of Giant Paraesophageal HerniaHiatal hernias are common in people more than 50 years of age. Most are small and asymptomatic,but approximately 5 percent are giant paraesophageal hernias (GPEH) with migration of thegastroesophageal junction and portions of the stomach into the chest. When a significant volumeof the stomach herniates into the chest space, concerning symptoms such as early satiety,vomiting, and pain cause the patient significant distress and can herald impending emergentobstruction and loss of blood supply to the stomach. D I V I S I O N O F G A S T R O E N T E R O L O G Y, H E PAT O L O G Y, A N D N U T R I T I O NGASTROE NTE ROLOGY DIG ESTWe are now working to further improve onthis standard of care using robotics, whichgive expert surgeons the opportunity towork with an extremely precise tool.Robotic surgery — which is actuallytelemanipulation of an advancedinstrument that the surgeon controlscompletely — has several potentialadvantages over laparoscopy. The surgicalrobot allows for better visualization andgives better control of more dexteroustools (Figure 1). The well-characterizedbenefits of minimally invasive surgery, suchas faster recovery times and fewerpostoperative complications, seem to carryover to minimally invasive robotic surgeries.The surgeon’s experience, expertise, and The current standard of care for GPEH repairis to laparoscopically dissect the hernia sac,reduce the hernia, repair the diaphragmaticcrura, and perform an anti-reflux procedure.To avoid recurrence, high mediastinaldissection to free as much of the esophagusas possible is very important. The hernia sacand stomach must be completely dissectedaway from the mediastinal structures toenable a tension-free reduction back into theabdomen. In the Division of Thoracic andForegut Surgery at UPMC, we tend to avoidthe use of mesh or other prosthetics at thediaphragmatic hiatus through aggressiveand adept dissection in the mediastinum.A short esophagus, if present, must berecognized and managed with a Collisgastroplasty or other esophageallengthening techniques. During the Collisgastroplasty, we tubularize part of thestomach by stapling, so that the esophagusmay be lengthened to reduce tension.To date, surgeons at UPMC have performedmore than 1,000 laparoscopic GPEH repairs.Few centers can match our experience.Recently, an important study from our grouplinked performing GPEH repair in an electivesetting with reduced morbidity (18 vs. 38percent) and mortality (1 vs. 8 percent) ascompared with non-elective GPEH repair.The need to repair asymptomatic orminimally symptomatic GPEH is oftendebated, because balancing the risks ofsurgery with the risks of observation can bedifficult, especially in elderly patients. Ourfindings provide compelling evidence for thebenefits of earlier surgical repair. If a patientis having GPEH symptoms, they should beseen by a surgeon. Patients fare better ifthey are referred for evaluation before theircondition requires urgent care.Benefits of RoboticAssistedGPEH Repair76Treating GPEH by LaparoscopyDr. Luketich was one of the first surgeonsto explore treating GPEH’s laparoscopically.In a landmark, retrospective study of morethan 650 GPEH laparoscopic repairs atUPMC, we found that laparoscopic repairprovided excellent patient satisfaction,symptom improvement, and preservationof quality of life even when performed inpatients with comorbidities. Outcomes werevery similar to the outcomes of opensurgical repair at an experienced center,harkening back to the gold standard at thattime. This new laparoscopic procedureresults in far less morbidity, low mortality( 2 percent), and low rates of recurrence. Inderpal S. Sarkaria, MD, FACS, is vicechairman of Clinical Affairs in the Departmentof Cardiothoracic Surgery and director ofThoracic Robotic Surgery at UPMC. He is athoracic surgeon who specializes in malignantand benign diseases of the chest including thelungs, pleura, esophagus and mediastinum.Some patients present in extremis, when thestomach is under torsion, infarcted, and atrisk of losing its blood supply. This can causedeath of the stomach, which can belife-threatening. Historically, patients withGPEH were referred for surgical repair onlyin the most urgent cases, because there wasa poor perception of the benefits of GPEHrepair as compared with the risks of theprocedure. Pioneering work done at UPMCby James D. Luketich, MD, FACS, and hiscolleagues in the UPMC Department ofSurgery changed this paradigm andestablished laparoscopic GPEH repair as thegold standard approach.1 We are now usingrobot-assisted laparoscopic surgery forGPEH repair in an increasing number ofpatients and have found that this safe andeffective repair results in excellent outcomesand safety.Figure 1. Room setup and patient positioning.Reprinted from Operative Techniques inThoracic and Cardiovascular Surgery, 18(3),204-214. Justin Karush and Inderpal S. Sarkaria,Robotic-Assisted Giant Paraesophageal HerniaRepair and Nissen Fundoplication. Copyright(2013), with permission from Elsevier.Figure 2. Cruroplasty. Reprinted from Operative Techniques in Thoracic and Cardiovascular Surgery,18(3), 204-214. Justin Karush and Inderpal S. Sarkaria, Robotic-Assisted Giant Paraesophageal HerniaRepair and Nissen Fundoplication. Copyright (2013), with permission from Elsevier.Continued.
Luketich JD, Nason KS, Christie NA, et al. Outcomesafter a decade of laparoscopic giant paraesophagealhernia repair. The Journal of Thoracic andCardiovascular Surgery. 2010;139(2):395-404,404 e391.GASTROE NTE ROLOGY DIG EST am V, Luketich JD, Winger DG, et al. Non-ElectiveTParaesophageal Hernia Repair Portends WorseOutcomes in Comparable Patients: a PropensityAdjusted Analysis. Journal of GastrointestinalSurgery: Official Journal of the Society for Surgery ofthe Alimentary Tract. 2017;21(1):137-145. arush J, Sarkaria IS. Robotic-Assisted GiantKParaesophageal Hernia Repair and NissenFundoplication. Operative Techniques in Thoracicand Cardiovascular Surgery. 2013;18:204-214. arkaria IS, Latif MJ, Bianco VJ, et al. Early operativeSoutcomes and learning curve of robotic assistedgiant paraesophageal hernia repair. Int J Med Robot.2017;13(1).Friday, May 10 at 8 a.m. to 4 p.m.The University Club123 University Place, Pittsburgh, PA 15260For more information, please contactSusan Piccirilli at piccirillis@upmc.edu.Ramon Bataller, MD, PhD, and GavinArteel, PhD, FAASLD, Co-Edit February2019 Issue of Journal of Hepatology, aspecial issue on alcoholic hepatitis. Thisissue highlights alcoholic hepatitisadvancements, and the co-editors introducethe issue in a compelling editorialintroduction, “Alcohol-Related Liver Disease:A Time for Action.”Naudia Jonassaint, MD, Appointed asthe Department of Medicine’s First ViceChair for Diversity and Inclusion. Dr.Jonassaint, an assistant professor ofMedicine and a transplant hepatologist,will work to develop new initiatives andprograms to enhance diversity andinclusion across the department.Digestive Diseases Week:We look forward to seeing you at DDW inMay. Stop by the exhibit hall to meet ourexperts and learn more about our program.Saturday, May 18 to Monday, May 20San Diego Convention CenterSan Diego, CAPancreasFest2019:PancreasFest is a meeting of pancreasphysicians and translational researchersduring the last week of July. It is an umbrellaconference that supports multiple smallermeetings with focused goals and anoverarching pragmatic purpose: facilitatingmulticenter research.[dates for PancreasFest]William Pitt Union3959 Fifth AvenuePittsburgh, PA 15213AASLD 2019 Liver Meeting:Please visit our booth at the exhibit hall tomeet our experts and learn more about ourprogram. We look forward to seeing you inNovember.Friday, Nov. 8 to Tuesday, Nov. 12John b. Hynes Memorial Convention CenterBoston, MADavid Binion, MD, Receives Sherman Prizefor his analysis of “Big Data” to betterunderstand IBD and to optimize treatmentstrategies for patients with Crohn’s diseaseand ulcerative colitis. Dr. Binion receivedthis coveted award from the ShermanFoundation during the national Advances inInflammatory Bowel Disease meeting inDecember 2018.Randi Sigal and Pamela Wein-LevyHonored at Crohn’s & Colitis AnnualLuncheon, by the WPA/WV chapter of theCrohn’s & Colitis Foundation for theiroutstanding support of IBD patients andpatient advocacy, especially for theirfounding of UPMC’s IBD Connect. For more information, contact Joy Merusiat joj2@pitt.edu.James B. McGee, MD, Selected as The2018 Recipient of The Carnegie ScienceAward, in the University/Post-SecondaryEducator award category in May 2018. Thisaward was presented by the CarnegieScience Center in recognition of Dr.McGee’s excellent work and dedication inscience and technology teaching. Dr.McGee is an associate professor of medicinewith the University of Pittsburgh Division ofGastroenterology, Hepatology and Nutrition.He also serves as the assistant dean ofMedical Education Technology and directsthe Lab for Educational Technology for theUniversity of Pittsburgh School of Medicine.Eva Szigethy, MD, PhD, Will Be thePrinciple Investigator for a 6.3 MillionPCORI (Patient-Centered OutcomesResearch Institute) Grant, “SpecialtyMedical Homes to Improve Outcomes forPatients with Inflammatory Bowel Disease(IBD) and Behaviroal Health Conditions.”Dr. Szigethy submitted this grant incollaboration with the UPMC Center forHigh Value Health Care. She is a professorof Psychiatry, Medicine and Pediatrics and afaculty member with the Division ofGastroenterology, Hepatology and Nutrition,where she directs Total Care-IBD and theUPMC IBD medical home. She is thefounder of the Division’s VisceralInflammation & Pain (VIP) Center.D I V I S I O N O F G A S T R O E N T E R O L O G Y, H E PAT O L O G Y, A N D N U T R I T I O NNason KS, Luketich JD, Qureshi I, et al. Laparoscopicrepair of giant paraesophageal hernia results inlong-term patient satisfaction and a durable repair.Journal of Gastrointestinal Surgery: Official Journalof the Society for Surgery of the Alimentary Tract.2008;12(12):2066-2075; discussion 2075-2077.This conference will provide health careprofessionals with an overview of currenttrends, management techniques, andupdates on various topics, including livingdonor transplants, trends in organ allocation,and caring for patients with end-stage liverand kidney disease. At UPMC, we have developed advancedstapling techniques using the roboticplatform to enable the surgeon to “selfassist.” Because the robotic machine hasmore than two arms, a single surgeon canplace more than two tools at the same time.The surgeon can set instruments forretraction and exposure, and thenmanipulate the robotic stapler. Smallchanges in instrument position can bedifficult for a bedside assistant to avoidduring traditional minimally invasive surgery.In contrast, the robotic arms are very stable.The robotic stapler is immobile once it isapplied, resulting in a better staple line withless bleeding. Additionally, the surgeon canfocus more thoroughly on the operation,because he or she does not have to “think”for another set of hands and then relay thoseexpectations to the assistant.References2019 Update in AbdominalTransplantation Medicine and Surgery:98Robotic GPEH repair can be safely adoptedwith comparable results by surgeonsfamiliar with minimally invasive repair ofparaesophageal hernias.Experts at the UPMC Department ofCardiothoracic Surgery, are spearheadingpioneering advancements in robotic thoracicsurgery, and robotic laparoscopic GPEHrepair is an excellent application of thistechnology. The surgeon can “self-assist”through every step of the operation withexcellent visualization in the tight spaces ofthe patient’s anatomy. Further assessmentof robotic GPEH repair is ongoing. As withany complex procedure, we are exploringinnovative ways to achieve improvedoutcomes.Join the Division ofGastroenterology,Hepatology, and Nutritionat Upcoming Meetings andNational Conferences The procedures required during GPEH repair(i.e., gastropexy or gastroplasty, herniarepair, and fund
UPMC Presbyterian Shadyside is ranked among America's Best Hospitals by . U.S. News & World Report. SPRING 2019. Inside This Edition. 1. essage from the Chief M. 2. hanging the Paradigm: Living-Donor C Liver Transplantation irtual Patient Software: Untapped V Technology for Practicing . Gastroenterologists . 6. obotic Repair of Giant R .