Transcription
Evaluation reportJanuary 2019Southwest Idaho Treatment CenterSouthwest IdahoTreatment CenterOffice of Performance EvaluationsIdaho LegislaturePromoting confidence and accountability in state government
Office of Performance EvaluationsCreated in 1994, the legislative Office of Performance Evaluations(OPE) operates under the authority of Idaho Code §§ 67-457–464.Its mission is to promote confidence and accountability in stategovernment through independent assessment of state programsand policies. The OPE work is guided by professional standardsof evaluation and auditing.Joint Legislative Oversight Committee2017–2018The eight-member, equally bipartisan Joint Legislative OversightCommittee (JLOC) selects evaluation topics; OPE staff conductthe evaluations. Reports are released in a public meeting of thecommittee. The findings, conclusions, and recommendations inOPE reports are not intended to reflect the views of the OversightCommittee or its individual members.SenatorsSenator MarkHarris (R) andRepresentativeMat Erpelding (D)cochair thecommittee.Mark HarrisMichelle StennettCherie Buckner-WebbCaroline Nilsson TroyPaul AmadorElaine SmithRepresentativesMat Erpelding2Dan Johnson
Southwest Idaho Treatment CenterFrom the directorJanuary 16, 2019MembersJoint Legislative Oversight CommitteeIdaho LegislatureThe operational model of the Southwest Idaho Treatment Center(SWITC) is no longer tenable. The center lacks enough clients foreconomies of scale to support the variety of expertise needed. Inaddition, its institutional setting prevents the center fromreplicating community living for individuals with intellectualdisabilities. Often these vulnerable individuals have co-occurringmental illnesses, complex medical and behavioral issues, andhistory of violence or involvement with criminal justice system.Idaho lacks a long-term vision for how to have an effective andefficient system of care for these individuals. This lack of visionhas contributed to a culture of constant crisis at SWITC,resulting in stress, anxiety, and despair on the part of staff andgaps in the quality of care provided to SWITC clients.The Department of Health and Welfare, with policy guidancefrom the Legislature, needs to create a long-term vision for howIdaho is going to serve these individuals in crisis.The department also needs to establish strong leadership andmanagement practices at SWITC, starting with a formal strategicplan and a formal quality improvement system.954 W. Jefferson StreetSuite 202Boise, Idaho 83702Ph. ses fromthe Governor andthe Departmentof Health andWelfare are inthe back of thereport.I want to commend SWITC’s staff and management for theirhard work in difficult circumstances and for the help they gave usduring this evaluation. I would like to thank the clients at SWITCfor letting us into their home.Sincerely,Rakesh Mohan, DirectorOffice of Performance Evaluations3
ContentsPageExecutive summary .51. Introduction .82. Long-term vision .123. Oversight.20Jen Schneider, PhD,Associate Professor atBoise State University4. Management and leadership .29Bob Thomas of Robert C.Thomas and Associates5. Priorities .39Ryan Langrill conductedthis evaluation with theassistance of Casey Petti.Margaret Campbell copyedited and desktoppublished the report.Technical assistance andquality control review wasprovided by twoconsultants:AppendicesHistoric, black and whitephotos were provided bythe Department of Healthand Welfare.4A. Request for evaluation .53B. Evaluation scope .56C. Methods .57D. Other state models .65E. Advisory board bylaws .69F. Caregiver misconduct registry .75Responses to the evaluation .77
Southwest Idaho Treatment CenterExecutive summaryWhy we were asked to do this study.The Southwest Idaho Treatment Center (SWITC) is the highestlevel of residential treatment for Idahoans with intellectualdisabilities. Clients served at SWITC have needs that could not bemet in the community or have been placed by the court into thecustody of the Department of Health and Welfare. In 2017SWITC was thrust into the spotlight after six employees left afterfindings of abuse or neglect, a client committed suicide, andfailed inspections threatened to lose the state 8 million per yearin federal matching funds.What we found.Idaho lacks a coherent vision for services to individualswith intellectual disabilities who are in crisis. Efforts inrecent years have focused on keeping individuals in thecommunity and out of institutions. These efforts havetransformed the role of the state as the provider of last resortwithout a clear focus on the individuals whose needs meet thelevel of care at SWITC. Every client at SWITC has complexbehavioral or medical needs, and many have co-occurring mentalillnesses and a history of assault or self-harm.Management does not have an effective approach tosolving problems. SWITC’s constant focus on putting out fireshas undermined its ability to make progress on long-termobjectives. Management’s decisions lack buy in from staff, andchanges are made without effective follow-through andmonitoring.SWITC exhibits symptoms of organizationaltrauma. Attitudes and practices developed for survival in timesof crisis have become normalized and are passed on to new staff.Many in leadership and clinical positions came during crisis, did5
not have effective training, and have struggled to understandtheir role.Staff trauma and injury is significant. For the first half of2018, one in ten staff days was spent out on injury; on one shiftthat number was one in five. Injuries also lead to medical layoffsor staff quitting for fear of further injury. Staff are frequentlyassaulted, sustaining both severe and chronic injuries. Whilephysical injuries are addressed, psychological trauma remains,and staff lack adequate tools for self-care. These unaddressedneeds lead to dysfunctional relationships with clients.Understaffing has continued to get worse. For six of thefirst nine months in 2018, SWITC lost more staff than it hired.Understaffing threatens client and staff safety, in turn worseningturnover and putting clients at risk of abuse and neglect.The approach to treatment is reactive rather thanproactive. Exacerbated by understaffing and a crisis mentality,direct care staff are often described as babysitters waiting for thenext behavioral crisis. As new staff are hired into an environmentwhere being reactive is the norm, efforts to encourage proactivesolutions get more difficult.SWITC has made significant changes in the past twoyears. However, much more needs to be done. Staff caredeeply for clients and the organization. They have great energyand ideas. After the traumatic events of 2017, SWITC madechanges to address gaps in management, staffing, and training.SWITC hired a program manager from out-of-state, implementeda two-week staff training program, and significantly increasedpay for new hires and existing staff. Other efforts includeimproved relationships with adult protective services andtrainings for investigative staff.The department acknowledged SWITC’s obsolescence in its planto sell the campus and build a new facility elsewhere. The planwas abandoned due to barriers selling the land, not changes inthe state’s needs. In the meantime, expectations that SWITC’sfacilities were to be demolished had discouraged thedepartment’s long-term investment in maintenance andimprovement.6
Southwest Idaho Treatment CenterWhat to do next.We made recommendations to address system-wide issues andissues with SWITC’s operations and treatment standards. Thekey to making long-term progress rests with two corerecommendations:We recommend that the Department of Health andWelfare develop a strategic plan and a formal qualityimprovement process at SWITC. This process should bedone in a way to ingrain staff buy in, accountability, and formalevaluation of efforts into SWITC’s organizational culture.Priorities for program improvement include addressing stafftrauma and injury, understaffing, gaps in training andsupervision, a reactive approach to treatment, and problems withthe discharge process. Improvements in SWITC’s leadership andmanagement are necessary. We recommend that the departmentpresent the strategic plan and updates on its qualityimprovement process to the legislative Health and Welfarecommittees at the start of the 2020 legislative session.We recommend the Legislature direct the Departmentof Health and Welfare to develop a long-term vision forIdaho’s system of crisis care and its role as provider of last resortfor those with intellectual disabilities. The Legislature shouldprovide policy guidance for this vision. Stakeholders and otherstates should be included as appropriate.In addition to these two core recommendations, we recommendthe following:SWITC should ensure that it conforms to requirements for adultprotection and child protection when it conductspreinvestigations of allegations of abuse and neglect.The Legislature should consider establishing a registry ofperpetrators of abuse or neglect of vulnerable adults to excludeperpetrators from working as a caregiver.The Legislature should also consider supporting SWITC’s effortsto improve staff recruitment and retention by making earlyretirement available for staff, in recognition of their high rate ofinjury.7
IntroductionLegislative interestIn March 2018 the Joint Legislative Oversight Committee askedus to evaluate the Southwest Idaho Treatment Center (SWITC).SWITC is overseen by the Department of Health and Welfare. Itonly serves Idahoans with intellectual disabilities who have beencommitted to the department by the courts or who are in crisisand cannot be served in a less restrictive setting.In 2017 SWITC failed a recertification survey and a subsequentfollow-up conducted by the department’s Bureau of FacilityStandards. If SWITC were to lose certification, the state wouldlose almost 8 million per year in federal matching funds.SWITC passed a second follow-up survey, but legislators whorequested this evaluation reported that complaints about seriousnoncompliance continued to persist. Their request letter is inappendix A.In August 2017 a client was found dead of apparent suicide. Thecoroner reported that the client had been dead for six or sevenhours, despite staff documenting that they had checked on himevery 30 minutes. Reports surfaced throughout the summer of2017 about an internal department investigation that led to theinvoluntary termination of six staff for abuse or neglect.SWITC’s secure treatment facility, which the Legislatureauthorized in 2017 but has yet to open, does not have federaloversight, unlike much of SWITC’s operations. Somestakeholders suggested that the configuration of state oversightby the department may not be sufficiently independent.8
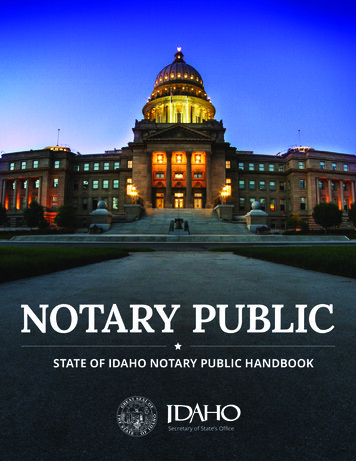
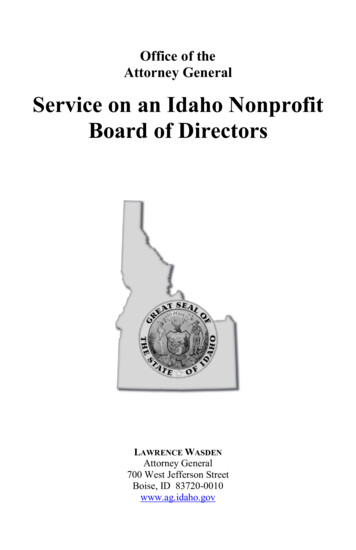
Southwest Idaho Treatment CenterTransformationsIn the past, across the country, state-operated institutions servedas long-term homes for individuals with intellectual disabilities,isolating them from the wider community. Today, states focus onproviding services to individuals with intellectual disabilities inthe community. As services in the community have becomeavailable, fewer individuals are served in institutions. In 1977more than 155,000 individuals with an intellectual disabilitylived in state-operated institutions. That number declined to56,000 in 2003 and 31,500 in 2015.In Idaho, SWITC’s population has declined more dramatically, asshown in exhibit 1. With the decline in the number of individualsliving in institutions, the purpose of institutions has changed.Rather than serving anyone with an intellectual disability,institutions tend to serve only those with complex medical orbehavioral needs, who are difficult to serve in the community.In 2015 the Department of Health and Welfare adopted astrategic initiative to “develop a therapeutic stabilization andtransition center for clients” with an intellectual disability. Theinitiative noted that “the department does not currently have theproper facilities or services to adequately care for or treat”individuals who have an intellectual disability and who are athreat to themselves or others.The Legislature established the Idaho StateSanitarium in 1911. White Hall, the firstresidential building and today the administrationbuilding, was completed in Nampa in 1918 bystate penitentiary prisoners. At its peak, thecampus was a long-term home to almost 1,000 residents withdisabilities.Today SWITC offers short-term crisis care for individuals withcomplex behavioral or medical needs. Its mission is to “support individuals in crisis to become stable, develop skills, andsuccessfully transition to the community.”The 600-acre campus is owned by the state. More than 500 acresare leased for two golf courses, a work release center, job corps,and a juvenile corrections facility.9
Exhibit 1In its 100-year history, the Southwest Idaho Treatment Center hasundergone several name changes.The population has varied greatly though the location has stayed the same.Nampa State School1955: almost 1,000 clients1,000 clientsIdaho State School and Hospital1965: almost 800 clients500 clientsIdaho State School and Colony1927: almost 400 clientsIdaho State Sanitarium1918: 165 clientsSouthwest IdahoTreatment Center2011: 49 clientsSource: Department of Health and Welfare records.2018: 17 clientsIn 2015 and 2016, the department intended to accomplish thisinitiative by “build[ing] an improved facility at an alternativelocation.” This improved facility would have replaced SWITC’scurrent location. The department conducted a conceptual studyand developed blueprints for this improved facility. In 2017 thegoal for the improved facility was dropped after the departmentdecided not to sell the 600-acre campus. The goal was replacedby an alternative goal to establish a secure treatment facility.During the 2017 legislative session, the Legislature authorizedthe creation of a state-licensed secure treatment facility atSWITC. The secure treatment facility would be used for residentswho have been found by a court to be a substantial threat to thesafety of themselves or others.10
Southwest Idaho Treatment CenterEvaluation approachSWITC is overseen by multiple outside entities. In 2017 and2018, the Bureau of Facility Standards conducted eightrecertification or complaint surveys. Surveys are intended toensure that SWITC complies with minimum regulatorystandards. During our scoping process, stakeholders said theybelieved compliance to federal regulations was necessary, butcompliance alone was not sufficient to ensure that SWITC offeredthe best possible quality of care.DisAbility Rights Idaho is the state’s federally mandatedprotection and advocacy agency. Its investigative authorityrevolves around protecting individuals from abuse and neglect.In October 2018 it released a report titled No Safe Place to CallHome. The report reviews serious breakdowns in oversight atSWITC that contributed to an ongoing abuse of clients fromJanuary 2017 to January 2018. The report reviews internalinvestigations for abuse and neglect and concludes by suggestingthat the state should consider closing the facility. Nineteenrecommendations are directed toward revising SWITC’s practiceor state policy.SWITC’s responses to ongoing oversight activities and its internalquality improvement efforts mean that SWITC’s operations haveevolved throughout this evaluation. Our evaluation seeks to fill agap not addressed by other oversight activities. This gap is toseek solutions by looking at SWITC as a system. We focus onconcerns of external oversight and on issues of operations andmanagement that appear to be persistent or appear to be the rootcause of more visible issues. The scope of our evaluation is inappendix B. The methods for the evaluation are discussed inappendix C.11
Long-term visionIdaho has mirrored the nationwide effort to move individualswith intellectual disabilities out of institutions and into thecommunity. This effort has resulted in a dramatic decline ofindividuals living at SWITC in the past several decades. The mostrecent step in this effort came in 2009. The Legislature directedthe Department of Health and Welfare, which oversees SWITC,to create a plan to transition residents into the community.The resulting plan led to legislation in 2011 that renamed theIdaho State School and Hospital to SWITC. In addition,legislation limited admission, except in cases of emergency, to (1)those who had exhausted all community options or (2) thosecommitted to the department’s custody by the courts. The planled to a further decline in the number of clients, from 62 in 2009to 17 in September 2018.SWITC is no longer a long-term home for clients. Its mission nowis to help in crisis situations those with the most complex needsin the state to become stable, to develop skills, and to successfullytransition to the community.12
Southwest Idaho Treatment CenterSWITC’s transformation occurred withouta coherent long-term vision for crisis care.The decline in SWITC’s population speaks to the department’ssuccess at moving individuals into the community. This success,however, has changed SWITC. SWITC has transformed in thepast 30 years from serving 200 clients with a wide range of needsto serving fewer than 20 clients. The focus on moving individualsout of SWITC came without an assessment of how to best servethe clients who stayed.Each client at SWITC has unique and complicated needs. Theseneeds range from full control of food intake because a disorderprevents the client from feeling full to the management ofcomplex seizure disorders. Behavioral concerns include historiesof physical assault, sexual assault, self-injurious behavior, andthe ingestion of inedible objects. Mental health diagnoses includeschizophrenia, bipolar disorder, borderline personality disorder,and posttraumatic stress disorder. SWITC serves both adults andminors. A federal surveyor who has visited facilities throughoutthe nation for decades commented during an October 2018survey that SWITC’s clients were the most complex andinteresting group she had ever seen.A seasonedfederal surveyorsaid that SWITC’sclients were themost complexand interestinggroup she hadever seen.SWITC’s staff and operational structure were insufficientlyprepared for the changing mission and population. Some longterm staff, hired to work with clients whose primary needs werefeeding and toileting, reported never being trained enough tomanage complex behavioral issues. Similarly, as SWITCdownsized, staff with specialized functions were eliminatedwithout sufficient plans to replace those functions.13
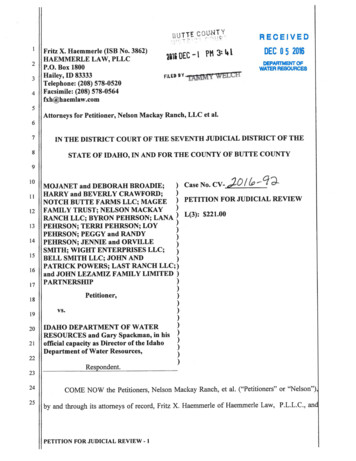
SWITC’s facilities are not well-suited forits mission.Residential buildings were completed in 2002. In interviews weconducted for an earlier evaluation in 2005, staff of the thenIdaho State School and Hospital commented that buildings weretoo institutional. They said that individuals with knowledgeabout actual operations were not consulted in the design of thesebuildings. Hallway andcommon area.The resident’scommon area has atelevision and anexit to a fenced-incourtyard.The design of the buildings was not initially conducive to clienttreatment or to staff or client safety. With fewer staff and morecomplex clients, the design is even less effective today. Thedepartment acknowledged this limitation in its 2015 and 2016strategic plans.Safety issuesFrom no locationin a unit cansomeone see theentirety of a unit.Deficits noted by staff include poor lines of sight. From nolocation in a unit can someone see the entirety of a unit. Staffalso reported that blind corners and nooks allow clients to hideor stalk others, putting other clients and staff at risk. Several exitroutes from each building makes it difficult to follow clientsattempting to leave without permission.The design of the residential buildings also contributes to a sensethat clinical and administrative staff are isolated from the day-today client care. Although some staff have offices located in theresidential buildings, no office has direct access to units.Unlike models of crisis care in some states, SWITC’s facilities donot mirror any living arrangements available in the community.14
Southwest Idaho Treatment CenterThe department reported that some clients struggle with theinstitutional model of living, which exacerbates the antisocialbehavior that SWITC was meant to address. In addition, SWITC’scampus is more isolated from resources in the community thanother places clients could live. It is at the center of more than 600acres zoned only for agricultural use. As of September 2018, thecampus contained more buildings, though many abandoned,than it did clients.As of September2018, thecampuscontained morebuildings,though manyabandoned, thanit did clients.Residential buildingsClients reside in three nearly identical buildings: Aspen, Birch, andPine. Aspen and Birch are each divided into two residential units,comprised of a kitchen and dining area, a day hall or common area,rooms for laundry, storage, giving medication, and 10 bedrooms. Ofthe 10 bedrooms, one has been converted to a private room forclients to relax or use the phone. Three to six bedrooms areoccupied, and the rest are vacant.Between each unit are hallways with staff offices and a clientcomputer room. Each unit has a fenced-in courtyard.Pine is also divided into two units: one side is a crisis bed and theother side is the secure treatment facility. The crisis bed isoccupied by one client at a time, at most, and is staffed by directcare staff who normally work in other buildings. The securetreatment facility has been modified from the other units: a firedoor closes off the kitchen and dining areas and alterations havebeen made for enhanced safety and more restrictive interventions. Kitchen anddining area. Staffnoted that someonein this layout caneasily get behindstaff. Staff workingin the kitchen donot have a line ofsight and arevulnerable toobjects thrown fromthe dining area.15
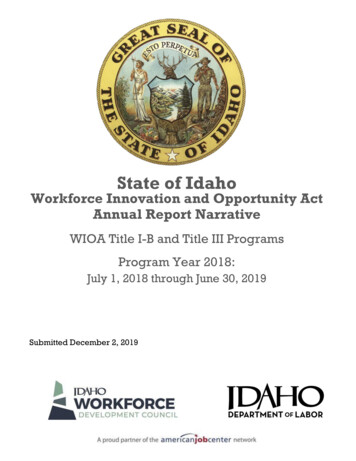
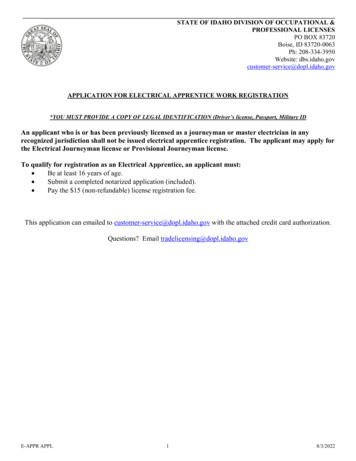
Operations suffered when SWITC losteconomies of scale.When SWITC was home to a much larger population, itsupported a variety of specialized staff. Full-time staff werededicated to training, occupational therapy, physical therapy,vocational services, quality assurance, pharmacy, and admissionand discharge. They included a full-time dietician, a chaplain,and a school teacher. Their positions were not eliminated for alack of need by clients or the organization. Rather, the needs ofsuch few clients did not justify a full-time position. Exhibit 2shows the decline in SWITC’s population, staff, and budget overthe past 10 years.Exhibit 2The size of SWITC’s population, staff, and budgethas dropped 60–80% in the past 10 years.Fiscal year 2018’s level as a percentage of 2009’s.100%75 clients375.53 FTE 28,748,40080%60%40%130.75 FTE 11,053,90017 clients20%Census on June 30StaffInflation-adjustedappropriationSource: Department of Health and Welfare records and legislative budget books.Appropriation adjusted to 2017 dollars using data from the US Bureau of LaborStatistics, Consumer Price Index for all urban consumers.16
Southwest Idaho Treatment CenterSWITC attempted to replace work performed by the eliminatedfull-time staff using alternative methods:Assigning additional duties to existing personnelHiring or contracting with part-time personnelUsing community providersDelegating responsibilities elsewhere in the departmentEach of the methods to replace full-time staff has led toshortcomings:Duties assigned to existing personnel were too oftenneglected, particularly as crises arose.Part-time personnel and community providers have not beenwell integrated with the treatment team, and the difficultyserving SWITC’s clients in the community created unmetneeds for SWITC’s clients.Responsibilities moved elsewhere in the department, mostnotably discharge coordination, have been done withoutenough communication and coordination with SWITC.SWITC was downsized without a sufficient vision for theorganization. Many programs that had been in place, such astraining and quality assurance, have faded. Staff have beenassigned these functions again, but they must establish newprocesses. Establishing new functions takes more effort thanmaintaining existing ones. This is particularly true given theexodus of staff with institutional knowledge and the need toadapt these functions to SWITC’s new size and mission.SWITC wasdownsizedwithout asufficient visionfor theorganization.Downsizing, by itself, poses systemic challenges due to manyfactors, such as a loss of economies of scale and the change in theprofile of clientele. The department, as the parent agency ofSWITC, had a responsibility to ensure that SWITC received thesupport necessary to avoid the struggles it has gone through.Although downsizing is inherently difficult, SWITC did so whilebeing neglected by the department and while losing much of itsinstitutional knowledge.17
SWITC’s operational model is neithereffective nor efficient for the long-term.SWITC is a vestige of an old treatment model and has large fixedcosts, both from its old campus and its variety of treatmentneeds. It has the fewest clients of any state-operated intermediatecare facility in the nation that is not currently closing. It carriesthe costs of a large, isolated treatment center without benefitsfrom economies of scale.The department acknowledged SWITC’s obsolescence in its planto sell the campus and build a new facility elsewhere. The planwas abandoned due to barriers selling the land, not changes inthe state’s needs. In the meantime, expectations that SWITC’sfacilities were to be demolished had discouraged thedepartment’s long-term investment in maintenance andimprovement.Other states also struggle to serve an increasingly complexpopulation. As they expanded services in the community,institutions have served an increasingly complex population.Some states continue to have large populations in institutionsbecause of policy decisions or larger overall populations. Somestates have done away with state-operated institutions, andothers have smaller, home-like crisis facilities. We did not findany single best system for Idaho to replicate. However, recentchanges and continuing struggles in other states represent anopportunity for Idaho to learn from and collaborate with them.RecommendationThe Legislature should direct the department to develop a longterm vision for Idaho’s system of crisis care and its role asprovider of last resort for those with intellectual disabilities. TheLegislature should provide policy guidance for this vision.Stakeholders and other states should be included as appropriate.18
Southwest Idaho Treatment CenterAt a minimum, long-term visionshould address the followingquestions:What series of living arrangements wouldenable the state to provide the most effective care? How wouldthese arrangements be licensed?Would a centralized crisis center or smaller regional centers bemore effective and efficient?How will resources in the community be developed to ensurethat individuals are receiving the least restrictive care?How will SWITC be coordinated with other elements of thedepartment, such as the state psychiatric hospitals and thecrisis prevention and court services team?How will the state ensure access to specialists and theintegration of specialists into clients’ care?What plans will be in place to ensure clients undergo anytransition smoothly?How will the state leverage the expertise of existing staff?Will crisis beds be licensed and possibly access federalMedicaid matching funds?Idaho’s neighbors have a variety of methods for serving individualswith intellectual disabilities in state-operated settings. A detaileddiscussion of models in other states and licensing options is inappendix D.19
OversightMultiple organizations are formally charged with the oversight ofSWITC or of its client rights. Issues of noncompliance and clientabuse led to a significant engagement of these oversightorganizations, including eight surveys in the past two years and areport by DisAbility Rights Idaho. Nevertheless, stakeholdersraised concerns that surveyors—employed by the Department ofHealth and Welfare—might not be sufficiently independent tooversee SWITC, particularly given that decertification would costthe department 8 million per year in federal matching funds.Additionally, advocates learned that former SWITC staff fired forabuse in June 2017 have continued to work with vulnerableadults. The continued employment of individuals with a historyof abuse raises questions about the system’s ability to protectvulnerable adults from individuals with a history of abuse.Who oversees SWITC?AdministrationSWITC is part of the Department of Health andWelfare, within the Division of Family andCommunity Services. The department’s human resources,contracts, financial operations, and facilities oversee SWITC’soperations. The Office of the Attorney General provides SWITC’slegal representation.Bureau of Facility StandardsWithin the department, as part of the Division of Licensing andCertification, the bureau conducts
Southwest Idaho Treatment Center 5 Why we were asked to do this study. The Southwest Idaho Treatment Center (SWITC) is the highest level of residential treatment for Idahoans with intellectual disabilities. Clients served at SWITC have needs that could not be met in the community or have been placed by the court into the