Transcription
Facility DesignAmerican Association of Physicists in Medicine2007 Summer SchoolJ. Daniel Bourland, PhDDepartment of Radiation OncologyWake Forest University School of MedicineWinstonWinston-Salem, North Carolina, USAOutline Facility PurposesFacility Design ProcessDesign Team FunctionsFunctional Plan To Spatial RealityExample: A Radiation Oncology FacilityKeys For Successful PlanningSummary JD Bourland and Wake Forest University Hugh Chatham Mem HospHealthcare Facility Purposes Accomplish Mission – Program, Department,Institution, other relevant groups (community, etc) WFUBMC A Facility is a Tool - a basic resource, facilitatingcomponent which programs and people depend on– Facilities house people – workers, patients, others– Facilities honor people; memorialize people– Facilities provide for visual response – artPoint – the physical structure is about people UNCUNC-Chapel HillFacility Design Process Identify Need and General Solution Vision – For the Future– What is desired to be accomplished?– Facilities – a 100-year event – future revisions Identify Players GreatBuildings.comPlanning On TheGrand Scale All spaces designated How will your plan fit? Challenges can beextreme– Proponents, participants, related programs,infrastructure, administration Proposal – A convincing argument UNC-Chapel Hill
Design Process and PeopleDesign Process – Continual, Iterative Designate Architect, Planner, Coordinator Define Design Team – Participants – “The Owners”Thorough planning provides for a successful facility andminimizes mistakes that may cost dollars or limitusefulness. This process may take a long time, dependingon the project scale.– There are different levels of ownership – “Physics” Planning Questionnaire - Program Objectives Functional Space Program Spatial Relationships of Functions (review) Planner/Coordinator – in-house, architectural firm– Space Functions (rev) Æ Block Diagram (rev) Æ Floor Plan– Key individuals to hold everything together, organize, etc Design Team – participating programs, departments,infrastructure (IS, utilities), administrationFacility Planning Process - DetailPlan ReviewSpecifications (Systems, Equipment, Shielding, Vendors)Plan Review and AcceptanceThen, Construction Phase (a different, important, story!)Facility Planning Process - DetailMeeting 1 – Month 1Meeting 2 – Month 2Meeting 3 – Months 3-4Meeting 4 – Months 5-9 Discuss Departmental ObjectivesReview Space Needs QuestionnairesIdentify Potential Options for PlanningReview Connections with otherMedical Center FunctionsBrief Overview of Site PlanningConsiderationsOverview Construction BudgetRequirementsEvaluate Preliminary MilestoneScheduleDiscuss Major Medical EquipmentSelection and Specification User GroupOrganizational ChartReview First Draft of Program andSpace RequirementsEvaluate Preliminary Sketches ofDepartment Adjacency OptionsIdentify Major EngineeringComponents and Obtain BaseEngineering DataReview Preliminary SketchesIndicating Room-By-RoomAdjacenciesDiscuss Building Design ObjectivesReview Parking and SiteObjectives/ParametersReview Construction BudgetRequirementsDiscuss Preliminary Building MaterialsReview Major Medical EquipmentSelection and SpecificationSteeringCommitteeDesign Teams llaryServicesBusiness,IS/IT Review and Approve Final Draft ofProgram and Space RequirementsConfirm Departmental AdjacenciesConfirm Room-By-Room AdjacenciesReview Preliminary EngineeringConceptsEvaluate Building Design OptionsConfirm Construction BudgetRequirementsReview Preliminary Life-Safety PlansReview First Draft of Schematic DesignNarrativeConfirm Major Medical EquipmentSelections Present Final Program of SpaceRequirementsPresent Final Building DesignPresent Final Floor PlansPresent Final Site Plan IndicatingParking, Entrances, Landscaping, EtcDeliver Final Schematic DesignSubmissionInitiate Preparation of PreliminaryEstimate of Project CostPhysicist – an important member of the Design TeamPlanning QuestionnaireFor each department, program, or serviceThe future is 5 years from now (or so) Scope of Services, Goals, and Objectives– Current and Future; Special future equipment or space (Vision) Workloads: Past, Current, Projected (Stats, Growth) Internal Functional Relationships Æ Flow– A map of how your department works (or doesn’t work)– Opportunity for revision Important External Relationships Æ Flow, Collaborators Staffing: Current, Projected, Organizational Chart (Flow) Existing Conditions – perceptions of current spaces
Planning Questionnaire - Existing ConditionsFunctional Space ProgramGrade as: Excellent, Adequate, InadequateAn Outline of Functions – A Relationship Map Systems––––––– SpaceHeating, A/CCommunicationsElectrical ServiceLightingPlumbingMedical GasesTransportation– Architectural Finishes– Efficiency of Layout– Size of Department Location–––– Medical Equipment– Linear Accelerators, otherTreatment– CT, MR, other Imaging– Patient supportRelationship to Other ProgramsRelationship to Outpatient FlowRelationship to Inpatient FlowRelationship to Supply Flow General Comments What is liked about currentspace?Functional Space ProgramReception/Waiting Entrance!Spatial Relationships - ClusteringClinic – Treatment and ImagingReception/WaitingFunctional Space ProgramAdd Individual Rooms, Hallways, etcConsider important relationshipsClinic – Treatment and ImagingReception/WaitingPatient SupportAdministrationClinic – Treatment and ImagingAdministrationClinicClinic SupportPatient SupportEducationPatient SupportReception/WaitingClinic SupportAdministration EducationResearchWhateverStaff SupportTechnical SupportResearchTechnical SupportStaff SupportPatient SupportAdministrationClinic SupportEducation ResearchClinic SupportEducation ResearchStaff SupportTechnical SupportStaff SupportWhateverTechnical SupportWhateverImportant Planning ActivitiesPossible Problem Areas(vary with project size and scope)A large number of possibilities Site visits to other facilities– Facility design aspects – with architects– Equipment – with vendors– Reps: technologists, therapists, physics, MDs, admin Equipment decisions and specificationsEquipment routes to rooms for installation - riggersSpecific room layouts, shielding consultant/specificationPlanning for the future: potential and unknownsClustering/Segregation of areasCommunication and review of all plans: follow processRequirements: State, Local Building Codes; Rad Prot RegsTimeline for Planning and Construction Net vs Gross space – use room templates Specification of shielded doors– mechanical and radiological parameters Thru-wall penetrations (signal cables, utilities): 2o, 1oDesign/layout of operator control areasLaser wall-mounting systems; Signage; InterlocksRoute for equipment entry (size and weight)Lead vs concrete shielding (diagnostic vs therapy)18 feet slab-to-slab thickness for therapy rooms
Possible Problem AreasExample: Comprehensive Cancer CenterA large number of possibilitiesWake Forest University Baptist Medical Center Room accommodations for the future? Location of network access ports (eg, in-room) Designation of utility chases – they always eat upspace in the end When possible, overstate site footprint relative tobuilding – don’t run out of land Main structural columns – widest placement possible Corridor width – standard 8 ft (code) Education of participants on unique or important itemsComprehensive Cancer CenterComprehensive Cancer CenterFacility RationaleDesirable Characteristics (Solutions)RadOnc Vision “One Stop Shop” for cancer services Multidisciplinary clinics“A premier academicradiation oncologydepartment committedto reducing the burdenof human cancer.” Cancer services spread in disparate locationsthroughout the institution Patients required to travel to multiple locations forspecialty care: med surg rad onc; labs, etc Few multidisciplinary clinic locations wherespecialty physicians could visit the patient Radiation oncology facilities over 30 years old,limited for expansion opportunities: 16,000 sq ft State-of-the-art facilities for radiation oncology, medical oncology,multidisciplinary clinics, and outpatient radiology (with a canceremphasis) Provision of existing/additional quality cancer support services in apleasing and comforting environment Radiation Oncology: Four same-class linear accelerators (IMRT,EPID), gamma/linac radiosurgery, 3 dedicated simulators (R/F,PET-CT, MR), dedicated HDR imaging, increase in examrooms, academic-admin offices, computing, trainee space (etc)Functional Space Program – RadOnc ExampleFunctional Space Program – RadOnc Example– for efficient patient visits with reduced patient burden– to facilitate interactions across physician specialtiesAdministrationClinicClinic SupportEducationPatient SupportReception/WaitingResearchTechnical SupportStaff SupportAsst. Clinical DirectorCast/ImmobilizationEnvironmental ServicesClass RoomComputer LaboratoryClinical Physics Lab.Copier/Fax, Office Stor.CT ScanningLinen Holding, CleanSeminar RoomCancer SupportProgramAppointments/Sched'ingBusiness ManagerClinic LobbyProtocol Review RoomLoungeChairmanCT Scanning ControlLinen Holding, SoiledConference RoomDietaryClinic ReceptionRad. Biology LabsCommunicationsClosetsChairman SecretaryExaminationNurses Sta./Work RoomLibrarySocial WorkWaiting, InpatientClinical/Resident LabClinical DirectorLinac TreatmentPat. Records/Film StorageMedical ResidentsRestroomsCesium IrradiatorClinical EngineerLinac ControlPatient TransportationMedical StudentsWaiting, OutpatTreatmentCoder/BillingLinac Film Stor/ReviewPhysician Work RoomNursing EducationComputer ProgrammerLinac Modulator RoomsUtility, CleanPhysics ResidentsDosimetristsScrub Room for IORTUtility, Soiled (Reproces)Physics StudentsNurse ManagerMinor Procedures, HDR/Orthovolt. TreatmentNursesPhysician Faculty-NCBHPhysician Faculty-RotatePhysics Faculty-NCBHPhysics Faculty-RotateProtocol ManagerRad. Biology FacultySecretarial PoolSenior TranscriptionistTranscription PoolRadBio Postdocs/RAsSupplies StorageWaiting, OutpatFU/Cons.Equipment RoomAdmin. Recept./WaitingEquipment Space - currently"borrowed"Admin/Chair MeetingCold RoomWarm RoomOrthovolt./HDR ControlDark RoomRad./Fluoro. ControlDishwashing/SterilizingPatient DressingLounge/Food StorageSimulationRestroomsSimulation ControlRadiosurgery SuiteComputer RoomClinical Engineer ShopElectrical ClosetsEquipment StorageFilmProcessing/StorageIsotope Storage/Prep.Mold Rm/MachineShopTreatment PlanningMail Center (Copy Rm?)RestroomsTherapist/Nurse Lockers
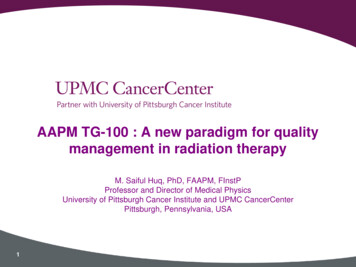
Functional Space Program – RadOnc ExamplePlan Review CommentsComments: July, 2000Comments: September, 20021. Group the Physics Section offices as a cluster –current plans have a few intervening offices.2. The main staff entrance enters through the mainpatient waiting area. This will not work.3. In general, it looks like a long walk from the MainEntry to the clinic area. If this length could bereduced, it might be helpful for some of our patients.4. We suggest that “customer service” and patient flowbe examined carefully to make the facility as patientoriented and patient friendly as possible. We suggestthe following approach for patient reception and“calling” of patients for treatment: The followingprocess is proposed:1. CT-PET Layout? Major column in space. Meet withvendor. Location of patient prep and injection areas?Use stretcher holding. Lead shielding required?2. MR Layout? (Ok? Are there changes to 3T design)Meet with vendor. Patient access acceptable? Doorsize?3. Linen cart alcove totally useless now.4. Location of blanket warmers? Place in one ofStorage Rooms.5. Badge controlled door access only to MR area.6. Move doors for Storage Rooms within MR/CT-PETform West side to North side7. Location of emergency OFFs in Linac rooms8. Gamma Knife room – plan for “Model C Unit” –vendor to review?9. Location of Radiation Monitor in HDR room (1620)10. Short conduit runs for Linac rooms, HDR, andGamma Knife?11. Review of door design for Linac rooms12. Review of communication plan so far13. Review of lighting plan, especially rooms withdimmable lighting?14. Lateral laser heights for Linac shown at incorrectheight. Height needs to match isocenter height (planA810). 14 A, B & C.1. Patients wait in Rad Onc waiting area, whether forconsults, sim, or on-treatment2. Patients only enter the consult/sim/treatment area whenaccompanied by a therapist or other staff5. Treatment Planning for the Gamma Knife and HDRmay be too small for both planning systems.6. Two Virtual Simulation rooms are needed in theSimulation area7. Two of four Linear Accelerator Rooms need the 3.5meter isocenter-to-wall distance.8. At one point large common conference room areaswere shown. Have these been moved to anotherfloor?WFUBMC Radiation OncologyNorthFunctional AreasSimulation: R/F, PET-CT, MRTreatment: 4 Linacs, GK, HDRReception, Exam, NursingAdmin, Ed, Clin TrialsDosimetryNorthWFUBMC Radiation OncologyFunctional AreasSimulation: R/F, PET-CT, MRTreatment: 4 Linacs, GK, HDRReception, Exam, NursingAdmin, Ed, Clin TrialsDosimetryLA1R/FPETLA2MRLA3LA4HDRGKOutpatient Comprehensive Cancer CenterBioanatomic Imaging and Simulation ToolsLA 1R/FPET-CTLA 2VSimGE Discovery ST PET-CT ScannerGE 3T MRI Scanner – Short Bore8 slice, helical scan, LightSpeed (Ultra) CTscanner, extra large FOV, BGO detectors,2D/3D, gated acquisition, Exact couch,LAP laser marking.3.0T (short bore), 3D brain and prostate spect,fMRI, MR angio, diffusion-weighted imaging,diffusion tensor imaging, multi-nuclear spect,Excite technology, LAP laser markingMRLA 3
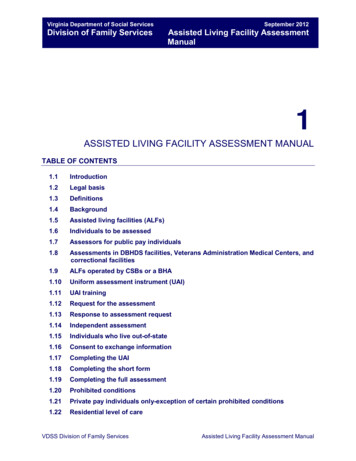
PET-CT Adjacent control, scanner,inject-wait, lab, and toilet 1/8 in Pb; control, scannerPET-CT ControlSimulation-TreatmentRelationship1/2 in Pb; inject-wait, toiletIsotope prep near on-siteShared Virtual SimulationLaser marking systemAutomated PACS archive,selective push to TPS Normal access securityView from Operator Entry Adjacent control, view window,scanner, plus annexRF- and B-Field shielding – 5gauss line containmentShared Virtual SimulationLaser marking system (work)Med gases, port for monitoringEquipment is very stable, excellentfield homogeneity, meets ACRaccreditation criteria for 3.0TExamining MRSI stabilityAutomated PACS archive,selective push to TPSPostings per magnetic field inEnglish and SpanishAll entry points carded for securityPET-CT Control3.0T MRPET-CTWaitHTMR mWaitMROfficeMREquipOfficePatient Access, Injection RoomInject-WaitVirtualSimPET-CTMREquipWaitMR Control– adjacent waiting, scanner bkg Inject-WaitView from Annex Entry
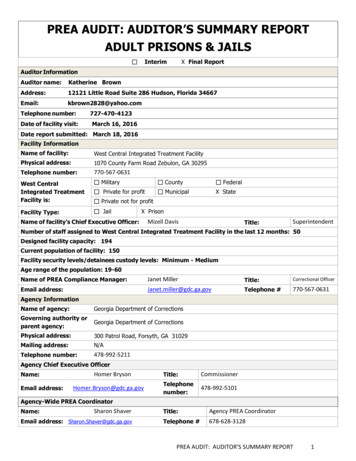
Gauss LineShieldingComputationMR Shield Materials“mu metal” and CopperPET-CT 5 gauss containment 0.5 gauss at operator –lower at PET-CT Institutional approval Performed by vendor Implemented at time ofconstruction Surveys show effectiveView from AnnexRadioactive Materials ControlFriendly to Homeland SecurityRADHDRGKExam Rooms,Structural Columnsand Utility Chases Exam Rooms – Standard,ENT, and In-patient Structural columns have togo somewhere Utility chases often added tocolumns– to the demise of adjacent space– designate as soon as possible!Keys For Successful PlanningEXEXEXEXEXEXEXEXEX Excellent communication– Make written comments, dated and sent; maintain records– Attend all User Meetings or send designee in your place Ask for high-quality architects, contractors, sub-contractors– Probably not your choice, but Administration’s;– Architect experience, level of expertise, match to the scope of theproject – choose a good one you can work with A critical eye for detail – learn to read plans (A, E, P, S)EXEXEX– A: Top-view floor plans;E: Electrical P: Plumbing– S: Structural (concrete, shielding)C: Communications– Obtain Sections – vertical planes;Know “Plan North”
SummaryKeys For Successful Planning Well-written [Device] specifications: radiologicaltreatment and imaging devices, their receipt, installation,and acceptance testing Well-written [Shielding] specifications: shieldingmaterials, thicknesses, shielded door mechanical andradiological properties, receipt of all devices, materials,and components and match to specifications [concretedensity 147 lb/ft3] Ask to be consulted on any potential changes on vendorsfor any radiological devices or components Be innovative to help solve problems – You’re a Physicist! Never revise anyone else’s space without their permission There are always constraints – make reasonable requestsYou’reInvited Facility Design: an important processSmall- or large-scaleVision and Proposal are importantParticipants are varied – multi-disciplinaryCommunication is keyPhysicist plays a key technical role – Get Involved!– Equipment, facility design, shielding specifications Have a great time designing and building!(hard hat time!)Thank you to the Organizers, the LAC, and AAPMStaff for the great Summer School and especially thefresh Minnesota sweet corn!Help!PleaseCome VisitAcknowledgements––––Karen Huey, WFUBMC Facilities PlanningEllerbe Becket, ArchitectsWFU Dept of Radiation OncologyIndustry Partners: GE Healthcare, Varian Grain Systems, Inc
8. Gamma Knife room - plan for "Model C Unit" - vendor to review? 9. Location of Radiation Monitor in HDR room (1620) 10. Short conduit runs for Linac rooms, HDR, and Gamma Knife? 11. Review of door design for Linac rooms 12. Review of communication plan so far 13. Review of lighting plan, especially rooms with dimmable lighting? 14.