Transcription
2021 OVERDOSE EPIDEMIC REPORTPhysicians’ actions to help end the nation’sdrug-related overdose and death epidemic—and what still needs to be done.END-OVERDOSE-EPIDEMIC.ORG
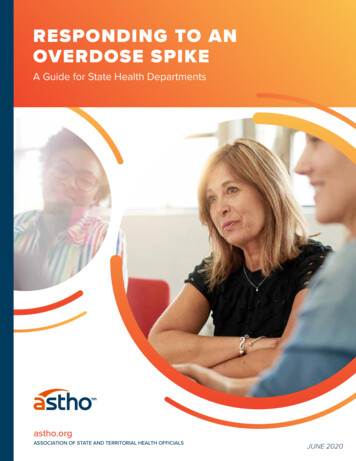
Opioid prescriptions decrease for the 10th consecutive year,but deaths continue to increase. It’s time to change course.AMA Opioid Task Force and memberorganizations urge policymakers totake action to remove barriers toevidence-based careAMA task force and its 25 member organizations releasenational recommendations onactions physicians can take toend the epidemicRise in overdose deathsdue to heroinCocaine and methamphetaminekill more people than heroin orRx opioidsCDC calls deaths from prescriptionopioids “an epidemic”AMA advises NationalGovernors Association in itsnew “Policy Academy” toaddress the growing epidemic20102011201220132014AMA joins harm reduction groups incalling for widespread access to naloxoneAMA warns that proposed2016 CDC opioid prescribingguidelines will harm patientswith pain2015201620172018AMA task force renews callto remove all barriers tocare, increase emphasis toreduce health inequities201920202021States take first steps to removebarriers to medications to treatopioid use disorderDeaths related to illicit fentanyl top 56,000AMA task force formed by AMA Board of Trustees tosupport patients with pain, substance use disorder ormental illness, and to enhance access to naloxoneRise in overdose deaths due to synthetic fentanyl beginsAMA drafts model legislation to remove insurance companybarriers to medications to treat opioid use disorderAMA Pain Care Task Forcefocuses on unique needs ofpatients with painEvidence-Informed Pain Management:Principles of Pain Care from the AMA PainCare Task Force releasedOpioid prescriptions decrease for 10thconsecutive yearThe American Medical Association convened two task forces between 2014–2019 that have providedactionable and measurable recommendations and principles for physicians, state and federal policymakers,and other stakeholders to combat the nation’s drug overdose and death epidemic.In response, there has been measurable progress by physicians and others across multiple areas and policychanges led by medical society advocacy. Yet, the nation’s drug-related overdose and death epidemic haschanged and worsened. As a result, the AMA has united the two task forces to launch a new, collectiveeffort to directly address this changing epidemic: AMA Substance Use and Pain Care Task Force.2021 OVERDOSE EPIDEMIC REPORT 2
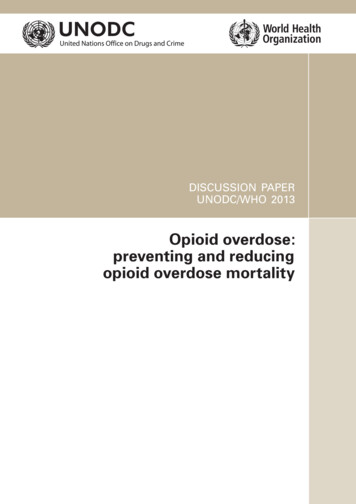
Fatal and non-fatal drug overdoses continue to increase.Reductions in opioid prescribing have not ledto reductions in drug-related mortalityPhysicians and other health care professionalshave reduced opioid prescribing in every statefor 10 consecutive years. They have increasedthe use of state prescription drug monitoringprograms (PDMPs) in every state for the pastfive years. Despite these efforts, drug-relatedmortality continues to rise.Overdose deaths:94,134*2010 2011(44.4% decreasesince 2011)910.6M44.4%decreasein opioid prescriptionsfrom 257.9M in 2011 to143.4M in 2020161.5M2012201320142015 2016201720182019 2020Opioid prescriptions:143,390,9511* Provisional data for the 12-month period Jan. 2020–Jan. se-data.htm106,000 physicians and healthIncrease in PDMPuse and 2.7B queriessince 20142care professionals certified to prescribebuprenorphine in-office—a nearly 70,000increase since 2017.3 Yet, millions witha substance use disorder (SUD) remainwithout access to evidence-based care.12 month-ending provisional number of drug overdose deaths by drug or drug classLegend for drug or drug classNumber of deaths60,000All opioidsSynthetic opiods, excl. methadonePsychostimulants with abuse potentialCocaineHeroinNatural & semi-synthetic opioidsMethadone40,00020,0000Jul 019Jul2019Jan2020Jul202012 month-ending periodPrescriptions for buprenorphine and naloxone4United States 2018–202017,500,000Prescriptions for buprenorphineand naloxone have increasedonly marginally in the past threeyears despite rising mortality.The AMA encourages physiciansto prescribe naloxone to patientsat risk of 5,000,00014,500,00014,000,00020182019Harm reduction and other communitybased organizations distributed morethan 3.7 million doses of naloxonebetween 2017–2020.⁵During the COVID-19 pandemic, thenumber of individuals filling a naloxoneprescription from retail pharmaciesdecreased more than 26%.⁶20202021 OVERDOSE EPIDEMIC REPORT 3
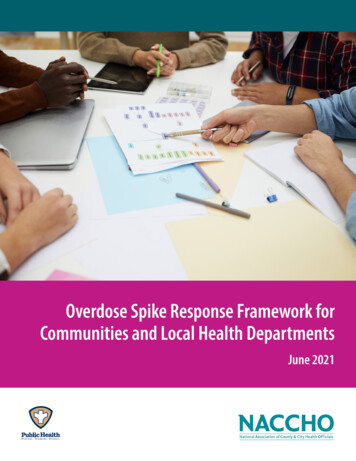
The COVID-19 pandemic has exacerbated the nation’s drug overdoseand death epidemic.Every state has reported increases in overdoses during the COVID-19 pandemic. It has affected patients withpain and an SUD, as well as patients who use harm reduction services. Structural racism and health inequitieshave made the pandemic even worse for marginalized and minoritized individuals.Drug overdose deaths in 2020 hit highestnumber ever recorded, CDC data showsIn pandemic, drug overdose deaths soar amongBlack Americans–Associated Press News–CNNChronic pain can be burdensome. Isolation duringthe pandemic can make it worse.–Washington PostAMA Urges Changes After Dramatic Increase inIllicit Opioid Fatalities–Medscape"From 1999 to 2018 [t]he greatest increases were among nonHispanic Black men for heroin overdose (3.3 in 1999 to 17.7 in2018) and synthetic opioid overdose (0.1 in 1999 to 36.0 in 2018)".⁷Overdose Deaths Surged In Pandemic,As More Drugs Were Laced With Fentanyl–NPRLatinos grapple with opioid overdose riseas pandemic triggers surge in U.S. use–NBC NewsSharp Rise In Drug Overdose Deaths SeenDuring 1st Few Months Of Pandemic–NPR"American Indian and Alaska Native (AI/AN) populations had thesecond highest overdose rates from all opioids in 2017 (15.7deaths/100,000 population) among racial/ethnic groups in the US.AI/AN populations also had the second highest overdose death ratesfrom heroin (5.2) and third highest from synthetic opioids (6.5)."⁸"From 2014-2017, among the Hispanic population drug overdosedeath rates involving all types of opioids increased, with thesharpest rise from synthetic opioids. Death rates involving syntheticopioids increased by 617 percent, and was the second highest forHispanics compared to all other race/ethnicities."⁹“The stakes are life and death”: Addictiontreatment’s Covid-19 challenge –VoxRead about reports in all 50 states: AMA issue brief:Nation’s drug-related overdose and death epidemic continues to worsen2021 OVERDOSE EPIDEMIC REPORT 4
Stakeholders need to work together to develop comprehensive, stateand community-based solutions and action-oriented efforts to improveoutcomes and save lives.The AMA strongly believes that ending the nation’sdrug-related overdose and death epidemic—as well asimproving care for patients with pain, mental illness orSUD—requires partnership, collaboration and commitmentto individualized patient care decision-making toimplement impactful changes, including: Urging states to adopt federal telehealth flexibilities toallow for the induction of buprenorphine at home Decriminalizing drug checking suppliesbased care for patients with pain, as well as supportedthe Rhode Island Medical Society in its campaign to enactthe nation’s first harm reduction center pilot program.13 S upported efforts with the American Society ofAddiction Medicine, the American Association forthe Treatment of Opioid Dependence and other keystakeholders to increase access to care for patients withan opioid use disorder. Ensuring opioid litigation funds are used only for publichealth purposes C onducted analysis with the nonpartisan and objectiveresearch organization NORC at the University of Chicagoto identify the gaps in states’ overdose reporting systems. Urging the Centers for Disease Control and Preventionto rescind the arbitrary thresholds in its 2016 opioidprescribing guideline and to restore compassionate carefor patients with pain A dvocated and provided support for the NationalAssociation of Insurance Commissioners to meaningfullyaddress health inequities in its work to advance mentalhealth and SUD parity.14 Removing structural inequities in care provided tohistorically marginalized and minoritized communities J oined with medical societies and patient advocates inOklahoma and Colorado to enact legislation to supportindividualized patient care decisions for patients withpain, including opioid therapy and non-opioid pain care.15Key collaborative AMA efforts in 2020–2021 C ollaboration with the Johns Hopkins School of PublicHealth and more than 50 national stakeholders has ledto over a dozen states enacting laws directing opioidlitigation funds to be used mainly for public health uses.10 P ublished a national roadmap with Manatt Health toprovide tangible actions for policymakers and publichealth officials to increase access to evidence-based care.11 W orked with the Milken Institute and the DrugEnforcement Administration to promote evidence-basedrecommendations to help employers increase access tocare for pain, SUDs and harm reduction services.12 Partnered with state and specialty societies to help enactseveral dozen laws and regulations to increase access tomedications to treat opioid use disorder, meaningfullyenforce mental health and SUD parity laws, decriminalizedrug checking supplies and remove barriers to evidence-2021 OVERDOSE EPIDEMIC REPORT 5
Physicians are ready towork with all stakeholdersto develop and implementcollaborative, evidence-basedsolutions to reduce mortalityand improve outcomes. Public health officials can help control infectious diseasespread through supporting comprehensive needle andsyringe exchange services.More stakeholders must come togetherand work collaboratively to act onthese recommendations. Medical and other health care professional licensingboards can help patients with pain by reviewing andrescinding arbitrary restrictions on opioid therapy. Policymakers can help increase access to evidence-basedSUD care by removing administrative barriers—such asprior authorization—for medications to treat opioiduse disorder. State officials can demonstrate leadership and supportfamilies by removing punitive policies against pregnant,peripartum and parenting individuals who have an SUD. Faith leaders can help destigmatize SUDs and harmreduction by educating parishioners and holdingoverdose awareness events.EMSBystandersLaw EnforcementFriends & FamilyFire & RescuePolicymakersPublic Health AgenciesHuman/Social ServicesState Bar AssociationsCommunity CentersFaith LeadersPayersEmergency DepartmentMedical Examiners/CoronersProfessional SchoolsMedical BoardsHealth CarePhysiciansPharmaciesHarm Reduction CentersTreatment CentersJails & PrisonsTo make meaningful progress towards ending this epidemic, a broad-based public health approach is required. This approachmust balance patients’ needs for comprehensive pain management services, including access to non-opioid pain care aswell as opioid analgesics when clinically appropriate, with efforts to promote appropriate prescribing, reduce diversion andmisuse, promote an understanding that substance use disorders are chronic conditions that respond well to evidence-basedtreatment, and expand access to treatment for individuals with substance use disorders.– Gerald E. Harmon, MDPresident, AMA2021 OVERDOSE EPIDEMIC REPORT 6
Treating the nation’s drug overdose and death epidemicdemands a far more proactive and coordinated approachfocused on evidence-based, public health solutions.Evidence and data are essential to helping patients with pain, increasing treatment forSUDs, reducing stigma, and preventing overdose and death.What we do today:“Crisis framework”Evolve to preventionframeworkEmploy effectivesurveillance strategiesImplement provenpublic health solutionsPrioritize preventingand treating SUDsBetter identify patientsat risk of an overdose andthose who have overdosedin the pastTake an evidence-basedapproach to prevention andtreatmentWhat we must do tomorrow:Integrated, sustainable, predictable and resilient public health ORINIAOKKSOHKYNDNCNYLAMTNENVNHNJMAMSMNFatal overdosesNon-fatal overdosesNo dataMOPrescriptionsPDMPMIData categoriesMDNMEMInadequate data collection preventseffective public health interventionsto reduce overdose and death.UTVTDifficulties remain in accessing high quality, timely,comprehensive and standardized data. Whilemetrics are generally available for drug-relatedoverdoses, data for non-fatal overdoses andother key indicators are not widely collected orstandardized across states and communities.These data gaps greatly hinder understandingof local situations and advancing prevention,treatment and harm reduction efforts.WA incomplete not standardized for comparison not timely widely variable from location to locationAKWhile data is critical to improving outcomes, current data is:2021 OVERDOSE EPIDEMIC REPORT 7
The AMA urges policymakers and otherstakeholders to take meaningful actionto remove barriers and increase patients’access to evidence-based care to savelives and help end the epidemic.1Remove barriers to evidence-based care for patients withan SUD. This includes removing prior authorization andstep therapy for medications to treat opioid use disorder(MOUD), continuing federal flexibilities for take-homemedication for opioid treatment programs and continuingtelehealth options for patients to begin MOUD.2Remove barriers to MOUD and treatment for SUDsand co-occurring mental illness in the nation’s jails andprisons. There is no legal, medical, or policy reason todeny access to MOUD or mental health care for justiceinvolved persons.Policymakers and other stakeholders have a choiceof whether to pursue evidence-based strategiesto support patients’ access to lifesaving and lifeaffirming care. Every effort must be made to removehealth inequities and other barriers for patients withsubstance use disorders, mental illness and patientswith pain. More of our loved ones will suffer and dieif these barriers remain.– Bobby Mukkamala, MDChair, AMA Substance Use and Pain Care Task Force3Take immediate steps to protect families by focusing on increasing access to evidence-based care ratherthan using punishment and the threat of family separation for persons who are pregnant, peripartum,postpartum and parenting.4Support patients with pain by rescinding arbitrary laws and policies focused on restricting accessto multidisciplinary, multimodal pain care; require health insurance companies and other payers to makenon-opioid pain care alternatives more accessible and affordable, emphasizing social determinants of health.5State insurance commissioners, attorneys general and the U.S. Department of Labor must increase effortsto review health insurers’ policies on a regular basis to ensure they comply with the Mental Health Parityand Addiction Equity Act—and hold them accountable if not.6Support increased efforts to expand sterile needle and syringe exchange services programs, decriminalizedrug checking supplies (e.g., fentanyl test strips) and urge manufacturers to make naloxone available overthe counter.7Develop and implement systems to collect timely, adequate and standardized data to identify at-riskpopulations, fully understand polysubstance drug use, and implement public health interventions thatdirectly address removing structural and racial inequities.2021 OVERDOSE EPIDEMIC REPORT 8
References1. I QVIA Institute Custom Xponent Opioid Dataset, SpecialtyView. For more information, IQVIA Institute PrescriptionOpioid Trends in the United States (December 16, 2020).Available at -states2. A MA Fact sheet: Physicians’ and health care professionals’use of state PDMPs available at s/2021/09/AMA-fact-sheetPDMP-2014-2020-FINAL.pdf3. U .S. Substance Abuse and Mental Health ServicesAdministration. Practitioner and Program Data. Availableat nt/practitioner-resources/DATA-program-data4. I QVIA Xponent limited to retail pharmacy dispensedprescriptions. Definition: USC 78312 Opioid ReversalAgents (naloxone) and USC 78340 Drug Dependence(buprenorphine and buprenorphine/naloxone), excludesbuprenorphine indicated for pain management (USC 02200)5. “ Recommendations for Federal Partners and HealthDepartments Navigating Naloxone Supply.” NASTAD. July2021. Available at https://www.nastad.org/file/7467/download?token J9L5i7YZ6. O ’Donoghue AL, Biswas N, Dechen T, et al. Trends in FilledNaloxone Prescriptions Before and During the COVID-19Pandemic in the United States. JAMA Health Forum.2021;2(5):e210393. doi:10.1001/ jamahealthforum.2021.03937. H oopsick RA, Homish GG, Leonard KE. Differences in OpioidOverdose Mortality Rates Among Middle-Aged Adults byRace/Ethnicity and Sex, 1999-2018. Public Health Rep. 2021Mar-Apr;136(2):192-200. doi: 10.1177/0033354920968806.Epub 2020 Nov 19. PMID: 33211981; PMCID: PMC8093836.8. I ndian Health Service. D-OVERDOSE-EPIDEMIC.ORG9. S ubstance Abuse and Mental Health Services Administration:The Opioid Crisis and the Hispanic/Latino Population: AnUrgent Issue. Publication No. PEP20-05-02-002. Office ofBehavioral Health Equity. Substance Abuse and MentalHealth Services Administration, 2020. A Digital Download/PEP20-05-02-002 0.pdf10. https://opioidprinciples.jhsph.edu/11. h er-2020-FINAL.pdf12. h L.pdf13. R hode Island is first state to support pilot harm reductioncenter. July 8, 2020. ion-center14. N ational Association of Insurance CommissionersMental Health Parity and Addiction Equity Act (MHPAEA)Workgroup. https://content.naic.org/cmte b mhpaeawg.htm. AMA letters to the workgroup include: wnload?uri Group-Aug-3-2020-FINAL.pdf15. S ee, for example, an actuarial analysis that demonstratedthe benefits of comprehensive care for patients with pain.American Medical Association, Colorado Medical Society,Colorado Pain Society, Manatt Health. Available at L.pdfThese materials include information derived from market research information provided by IQVIA, Inc. (“IQVIA”). IQVIA marketresearch information is proprietary to IQVIA and available by subscription from IQVIA. The IQVIA XponentR market research dataincludes estimates of dispensed drug prescription information from retail pharmacies (chain, mass merchandisers, independentand food stores) in the United States. IQVIA sources transaction information for 90% of the retail channel and uses a customizedand patented estimation methodology to generate accurate market estimates. IQVIA employs various proprietary methodologiesin data sourcing, data receipt, data editing and cleansing, creation and maintenance of reference files, data quality assurancesprocesses, reference data bridging, database management and report creation to produce these estimates. More informationabout IQVIA can be found at www.IQVIA.com. 2021 American Medical Association. All rights reserved. 21-5728772021 OVERDOSE EPIDEMIC REPORT 9
AI/AN populations also had the second highest overdose death rates from heroin (5.2) and third highest from synthetic opioids (6.5)."⁸ "From 1999 to 2018 [t]he greatest increases were among non- Hispanic Black men for heroin overdose (3.3 in 1999 to 17.7 in 2018) and synthetic opioid overdose (0.1 in 1999 to 36.0 in 2018)".⁷