Transcription
!1
2 0 18 al l con tr ibu ting aut hors.A l l r i gh ts rese rve d.T his wor k i s distr ib uted under aC re ative C om mon s At tribution N o nCo mm e rci al -NoDerivatives4 .0 In ter n atio nal L icense.T his wo rk m ay n ot be translated or c opi ed in wh oleo r in pa r t w i th ou t the written perm is s ion of it sa u th ors . How ever, t his edit ion is offered at noc ost as a reso urc e fo r all RRT clinicians .Whi l s t th e a d vi ce and information in t h is bo ok a reb elie ve d to be tr ue an d accurate at t h e d at e ofp ublic a tion , n eith er th e authors n or t h e e di t ors c a na cc ep t a ny legal resp onsibility for a n y e r ror s oro mis s ion s th at may be made. The e di tor s m a k e n ow ar r a nt, express o r implied, with re sp ec t t o t h em at eria l co ntain ed herein .T his bo ok i s in tend ed for use by m ed ic a lp rofe ssio na l s wi thin a h ospital en v iron m e n t .A lt hou gh all autho rs are medical e x pe r ts , anya ppl ic at i on o f in format ion provided is alway s theres pon si bi lity of the t re a t i n g h e a l th carepro fes si on al.I S BN 97 8 -0- 473 -4 537 5 -6Typeset in H elveti ca N eue, Futura & Droid SansT he l ate st versio n o f t his book will a l way s bea va ilab le to d own lo ad at:h t t ps://rr th an db oo k.orgC o nta c t: i n f o@r rt han dbook.org!2
MANAGINGD E T E R I O R AT I N GPAT I E N T SA Quick BedsideGuide forRapid ResponseTeam MembersRick ChalwinDar yl JonesAlex PsiridesSam Radford!3
Ed i t or s (l iste d alp hab e ti c al l y )Dr. Ri c k Ch a l wi nMB ChB F CICM M PHSta ff S pe c ia li s t , I n t e n si ve C a re U n i t , Ly e l l McEwi nHo s pit a l , S o ut h A u s tr a l i aSe nio r Le c t ure r, Ad e la i de H e a l t h S i m u l a t i on, Uni ve rs i t yo f A d el ai dePhD Ca ndi d at e , S c h o o l of P u b l i c H e a l t h , Uni ve rs it y ofAde la ideA / P ro f D ar y l Jon e sBSc (Hons) MB BS FR ACP FCICM MD PhDInt e nsi ve Ca re S p e c i a l i s t , A u s t i n H e a l t h , M el bo ur neAs so c ia t e P ro fe s s o r S P H P M , M o n a s h U n i v ersi t yAdj unc t A ss o c ia t e P ro f e s s o r, U n i v e rs i t y Melb our neMed ic a l D ire c t o r C ri ti c a l C a re O u t re a c h , Aust i n Ho sp i t alTwi t ter: j o ne s da z aDr. A lex P s i ri d e sB Sc ( Hon s) MB B S F CI CMInt e nsi ve Ca re S p e c i a l i s t , We l l i n g t o n R e g i onal H o spi t alSe nio r Cli ni ca l L e c t u re r, U n i v e rs i t y o f O t agoCli nic a l L e a d , N a ti o n a l D e t e ri o ra t i n g P a t i e ntPro g r amme , HQ S C , N e w Z e a l a n dTwi t ter: @ p si ride sDr. S am R a df ordB . Me d Sci (Hon s) MB BS ( Hons) FRA CP FCI CMGC H PEInt e nsi ve Ca re S p e c i a l i s t , A u s t i n H e a l t h , M el bo ur neHo no r a r y Le c t ure r, M e lb ou r n e U n i v e rs i t yDep ut y S t at e M e di c a l D ire c t o r, Do n a t e L i f e Vic t ori a!4
P REFAC EIn 2017, the president of the College of Intensive CareMedicine of Australia and New Zealand challenged therapid response community to develop a reference text forRapid Response Team (RRT) members. This handbook isa response to that challenge.It is intended to be a concise primer for those new to theRRT but may also provide useful insights for moreexperienced clinicians too. The content has been writtenfor all front-line clinicians attending RRT calls, and shouldbe applicable to staff from any discipline or department.This is intentionally not a comprehensive, didactictextbook. Chapters can be read in any order, or inisolation. Additional sources and reference documents arelisted at the end of each chapter for those seeking moreinformation.For this first edition, we have described approaches tothe management of general, adult in-patient deterioration.A future edition may be expanded to address specificpatient groups such as paediatrics, obstetrics and mentalhealth.This book is provided to the rapid response systemcommunity as a free resource in the hope that it will beuseful for responders. To enable us to track downloads,please share the website link rather than this file.Feedback and comments are welcomed and can be sentto info@rrthandbook.org!5
!6
INDEX(select page number to move to relevant chapter)01. Introduction902. What Is Known About Deteriorating Patients1103. Hospital Structures And Governance For DeterioratingPatients1904. Principles of Team Management3105. The Roles And Goals Approach To Rapid ResponseTeam Management4006. Key Phases Of A Rapid Response Team Call07. Rapid Response Team Activation475008. Team Assembly5409. Team Action Phase6110. Team Disassembly6811. Follow Up After the Rapid Response Team Call12. How To Approach Clinical Deterioration758213. Management Of The Patient With Respiratory Distress8914. Management Of The Patient With AlteredConsciousness And Neurological Deterioration10015. Management Of The Patient With Hypotension AndAltered Heart Rate11316. Management Of The Patient With Low Urine Output 12917. Management Of The Patient With Possible Sepsis13418. Management Of The Dying Patient140!7
!8
01. INTRODUCTIONDaryl JonesThe profile of hospitals and the patients they manage arechanging. Advances in medical treatments, increasing lifeexpectancy, societal and clinician expectations, andimproved anaesthetic and surgical techniques haveresulted in older patients receiving more complex, oftenmultiple, treatments. Concurrently, there are pressures onhospital occupancy, resource utilisation, and access tocritical care beds. These combined effects put patients ongeneral hospital wards at risk of experiencing clinicallyimportant deterioration.Studies conducted in the 1990s reported that patientsadmitted to hospital suffered serious adverse events inapproximately 10% of cases. Other studies revealed thatsuch events were preceded by signs of physiologicaldeterioration in up to 80% of cases, often for severalhours before the event occurred.In response, many hospitals worldwide have nowimplemented Rapid Response Systems (RRSs) toimprove the recognition of, and response to clinicaldeterioration in hospital wards. Key to this approach isthe presence of an expert responder team, referred to asa Rapid Response Team (RRT). Three systematic reviewshave demonstrated that the introduction of RRSs resultsin decreases in the frequency of in-hospital cardiacarrests, and one revealed a decrease in all-cause inhospital mortality.!9
With RRSs becoming widespread, focus has now shiftedtoward the epidemiology of the RRT patient. Severalstudies have revealed that between 10-25% of patientsare admitted to the intensive care following RRT review,that one fifth of patients receive more than one RRT call intheir hospital admission, that delayed review is associatedwith increased mortality, and that approximately onequarter of patients reviewed by the RRT will die duringthat hospital admission.Appreciation of the vulnerable nature of the RRT patienthas prompted efforts toward understanding of the causesof clinical deterioration needing RRT review, and trainingthe responders to optimise treatment and outcomes ofsuch patients. In contrast to in-hospital cardiac arrests,deterioration that causes a RRT review can be due tomultiple aetiologies. Thus, the patient is far lessdifferentiated, and the management of the their review ismuch more complex and diverse. Accordingly,management does not lend itself as much to thealgorithmic approach of basic and advanced cardiac lifesupport. In addition, an individual staff member from theward may attend RRT calls infrequently. This means thatthe formation of responding team is ad-hoc and it ishighly unlikely that they have trained together in themanagement of the RRT patient.In this book, we outline historic studies reporting adverseevents in hospitalised patients. In addition, we discusshospital strategies to improve the recognition of andresponse to clinical deterioration. Finally, we discuss theprinciples of team-based assessment of a deterioratingpatient, important elements of team leadership, and thespecific approach to common causes of RRT activation.!1 0
0 2 . W H AT I S K N O W N A B O U TD E T E R I O R AT I N G PAT I E N T SDaryl Jones, Chris SubbeSerious adverse events were previously common inhospitalised patientsSince 1960 there have been multiple studies exploring thenature of clinical deterioration in hospitalised patients.Initially, these studies identified the potential role ofmedical neglect and iatrogenesis in causing patient harm.These were supported by studies conducted in the 1990swhich further explored the resultant serious adverseevents.In Australia Wilson and co-workers reported that 17% off14,179 patients in 28 hospitals suffered an adverse eventwhich they defined as “unintended injury or complicationthat resulted in disability, death, or prolonged hospital stayand was caused by the healthcare management ratherthan by the underlying disease process". In New ZealandDavis and co-workers conducted a similar study amongst6579 patients in 13 hospitals and found a serious adverseincident rate of 12.9%. Using this definition multiplestudies worldwide identified that patients experience suchevents in around 10% of hospital admissions, and in onequarter of cases these were associated with permanentdisability or death.In 2000 the Institute for Medicine’s published a landmarkreport entitled ‘To Err is Human’ which introduced the!1 1
concept of healthcare related harm into the medicalmainstream. Subsequent studies explored adverse eventsin hospitalised patients in the context of specific clinicalcomplications. These were sometimes defined by severeevents such as cardiac arrest, unplanned ICU admission,or preventable in-hospital death. Alternatively, the eventwas defined by clinical complication such as myocardialischaemia, pulmonary embolism, in hospital sepsis, oracute kidney injury. In some studies the investigatorsjudged whether these events were preventable. However,there was not always strong agreement in suchjudgement.Adverse events were preceded by signs of instabilityIn order to examine for more objective criteria ofpreventability, some researchers assessed the periodleading up to the development of a serious adverse eventor complication to ascertain whether there was evidenceof prior clinical instability. Several studies revealed thatthese events what preceded by derangements incommonly measured vital signs, escalation in treatment,or documented staff concern in up to 80% of cases.Importantly, such deterioration had been present forseveral hours, potentially allowing for intervention priorthe occurrence on the event.The response of ward clinicians was often notcommensurate to the deteriorationRetrospective analysis of the assessment andmanagement by ward clinicians in the period leading upto serious adverse events found that the escalation ofcare and the subsequent treatment was deemed too!1 2
frequently be suboptimal. Common care issues prior tocardiac arrests included inadequate clinical assessment,medication errors and sub-optimal response tosymptoms. In a study of 100 consecutive emergency ICUadmissions suboptimal care was thought to results fromlack of organisational skills or knowledge, failure toappreciate the urgency of the situation, and failure to seekadvice.Several clinical conditions are common causes of inhospital complicationsStudies amongst surgical patients suggest that infections,thromboembolism and acute kidney injury are the mostcommon complications. For example, amongst 614,525patients in 300 US hospitals Hyder and co-workersrevealed that wound infection (5.25%), urinary tractinfection (1.54%), pneumonia (0.97%), venousthromboembolism (0.73%), acute kidney injury (0.43%)and myocardial infarction (0.3%) were the most commoncomplications.In a study of 4158 patients aged older than 70 years in 23Australian and New Zealand hospitals, the most commoncomplications were acute renal impairment (6%), acutepulmonary oedema (3%), acute myocardial infarction (2%)and wound infection (2%).Amongst general adult patients reviewed by the RapidResponse Team (See chapter 3) in Australia and NewZealand, pulmonary oedema, sepsis, seizures,arrhythmias and acute respiratory failure were the most!1 3
frequently reported clinical causes of clinicaldeterioration.Both clinical and system factors contribute to clinicaldeteriorationThere are a number of factors contributing to clinicaldeterioration in hospitalised patients (Table 2.2). In afollow-up study of the 2353 adverse events reported byWilson and co-workers a detailed qualitative assessmentwas conducted which found the following factorscontributed to the development of adverse events: 34.6%: 'a complication of, or the failure in, thetechnical performance of an indicated procedureor operation'15.8%:'the failure to synthesise, decide and/or act on available information'11.8%:'the failure to request or arrange an investigation, procedure or consultation', and10.9%:'a lack of care and attention or failure to attend the patient'In the United States, the term 'failure to rescue' is used todescribe an inadequate response by the hospital toclinical deterioration. While initially used in the context ofpost-operative complications, this terms is now morebroadly applied to deterioration without appropriateresponse to any hospital in-patient. Organisational cultureas evidenced by beliefs and behaviours might play animportant part. A study by Ghaferi comparied high andlow performing hospitals. It showed that althoughcomplication rates for major surgery were comparablebetween the hospitals, death after complication was!1 4
markedly different. This suggests that outcomes followingcomplications might be determined by a hospitalscapacity to recognise and respond to these events in atimely and efficient manner.How can adverse events be detected and managed?The following chapters will outline hospital structures andsystems aimed at improving the recognition of, andresponse to clinical deterioration. The principles of teammanagement (chapters 4 and 5), and the phases of teambased management of a deteriorating patient will then bepresented (chapters 6-11). Finally, approaches to themanagement of common scenarios encountered duringward-based clinical deterioration will then be outlined(chapters 12-18).Table 2.1: Summary of literature on deteriorating inhospital patientsSerious adverse events occurred in approximately 10%of hospital actionsSerious adverse events were commonly preceded bysigns of clinical deteriorationThe response of ward clinicians was often notcommensurate to the degree of clinical deteriorationThe assessment and treatment of clinical deteriorationon the ward preceding serious adverse events was oftensuboptimalEscalation to senior staff did not always occur!1 5
Table 2.2: Clinical and system factors contributingto clinical deteriorationVital sign measurement on hospital wards is intermittentIntervals between vital sign measurements maybe aslong as eight (or even twelve) hoursReviews by ward nurses and unit doctors can varyconsiderablyMany hospitals do not have policies to guide escalationof care when vital signs become abnormal or patientsdeteriorateThe first clinicians to review deteriorating patients areoften junior, lack experience and knowledge, and havemultiple competing prioritiesIn some instances, the usual clinicians may not beavailableStaffing levels out of hours are usually markedly lowerthan those during the day!1 6
Further reading:Jones D. Chapter 1. The role of a medical emergencyteam in a teaching hospital. Doctorate Thesis 2009Jones D, Mitchell I, Hillman K, Story D. Defining ClinicalDeterioration. Resuscitation. 2013;84:1029-1034Hyder JA, Wakeam E, Arora V, Hevelone ND, et.al.Investigation of the “Rule of W”, a mnemonic for reachingon postoperative complications. J Surg Educ. 2015;72:430-437Story DA, Leslie K, Myles PS, Fink M, et.al. Complicationsand mortality in older surgical patients in Australia andNew Zealand (the REASON study): a multicentre,prospective, observational study. Anaesthesia. 2010;65:1022-1030Jones D. The epidemiology of adult Rapid ResponseTeam patients in Australia. Anaesth Intensive Care.2014;42:213-219Wilson RM, Harrison BT, Gibberd RW, Hamilton JD. Ananalysis of the causes of adverse events from the Qualityin Australian Health Care Study. Med J Aust.1999;170:411-415Kohn LT, Corrigan JM, Molla S. To Err Is Human. Buildinga Safer Health System. Institute of Medicine (US). 2000Hogan H, Healey F, Neale G, Thomson R, Vincent C,Black N. Preventable deaths due to problems in care in!1 7
English acute hospitals : a retrospective case recordreview study. BMJ Qual Saf, 2012 Sep;21(9)Schein RMH, Hazday N, Pena M, Ruben BH, Sprung CL.Clinical antecedents to in-hospital cardiopulmonaryarrest. Chest. 1990:1388–92McQuillan P, Pilkington S, Allan A, Taylor B, Short A,Morgan G, et al. Confidential inquiry into quality of carebefore admission to intensive care. BMJ. 1998;316:1853–8Ghaferi AA, Birkmeyer JD, Dimick JB. Complications,Failure to Rescue, and Mortality With Major InpatientSurgery in Medicare Patients. 2009;250(6):1029–34!1 8
0 3 . H O S P I TA L S T R U C T U R E SAND GOVERNANCE FORD E T E R I O R AT I N G PAT I E N T SDaryl Jones, Chris Subbe, Tammie McIntyre,Carmel TaylorOverviewAll hospitals must develop and implement strategies toidentify patients who are at increased risk of deterioration,identify the deterioration when it occurs, and promptlymanage it in order to reduce the risk of subsequentmorbidity and mortality.This chapter outlines hospital structures and governancemechanisms that have been implemented to improve theprevention and identification of clinical deterioration andprovide a response to deterioration once it has occurred.Such approaches can be preventive, or reactive (Table2.1), and some strategies are outlined in more detailbelow. In Australia, the Australian Commission on Safetyand Quality in Healthcare (ACSQHC) has developed andpromulgated a National Consensus statement outliningeight essential elements for recognising and respondingto clinical deterioration in acute hospitals. In NewZealand, the Health Quality and Safety Commission(HQSC) has a national programme standardising bothrecognition and responses to adult in-patients whodeteriorate.!1 9
Vital sign documentationStudies examining adverse events such as in-hospitalcardiac arrest, unplanned ICU admission and unexpectedin-hospital deaths have noted that these are oftenpreceded by derangements in commonly measured vitalsigns. In many cases, these abnormalities remaineduncorrected for many hours.Hospitals should have a policy for the acquisition anddocumentation of vital signs. Studies in Australia haveshown that graphical representation of vital signs usingcolour coding to indicate normal or acceptable rangesimproves clinician recognition of deranged physiology.New Zealand has standardised the vital signs chart thatincorporated human factors design testing to optimiserecognition of abnormalities and vital sign trends. Inselected patients it may be desirable to continuouslymonitor vital signs, although evidence for theeffectiveness of this strategy is not definitive.Intensive care unit liaison nursesIntensive care unit liaison nurses (ICULNs) are seniornurses based in the ICU who aim to facilitate thedischarge of patients from the ICU to the ward, as well asreviewing and identifying at-risk and deteriorating patientsin hospital wards. In some instances, they are alsomembers of the Rapid Response Team (RRT) and canalso form part of early escalation systems. They areparticularly prevalent in Australia, the United Kingdomand New Zealand typically in larger hospitals with higherICU admission rates. Internationally they may be known!2 0
by a number of different names including outreach or'patient at risk' (PAR) teams.Several studies have explored the scope of practice ofICULNs and report that their value is in supporting andeducating ward staff, patients and relatives (Table 2.2).Available evidence suggests that the most reviewsperformed by the ICULN occur during routine follow-up ofpatients discharged from the ICU. Additional case-loadarises from participation in or follow-up of RRT patients,and de novo referrals from ward staff for patient concern.Hospital wide escalation policyThe ACSQHC consensus statement requires that all acutehospitals have a protocol to outline how the organisationwill respond to different levels of clinical deterioration.This is typically a graded response whereby theintensively of the response is commensurate to the levelof clinical deterioration. In Australian hospitals there aretypically three levels of response1.2.3.A 'Code Blue' or cardiac arrest call. A team isactivated and responds immediately when thepatient has a cardiac or respiratory arrest, or otherimmediately life-threatening emergencyA Medical Emergency Response or Rapid Responsecall. The team is typically activated when a patienttriggers pre-defined physiological calling criteria.The team is typically composed of senior and expertresponders, often from the ICU, and typically arriveswithin 5 minutes.Ward team based clinical review. This response isactivated when the patient displays milder degrees!2 1
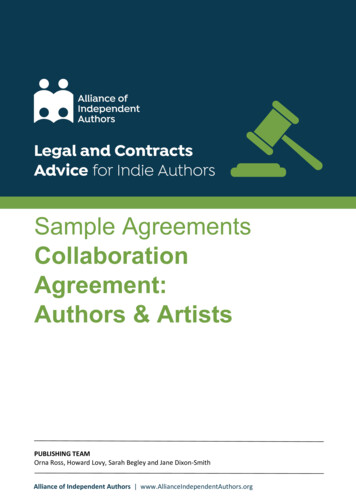
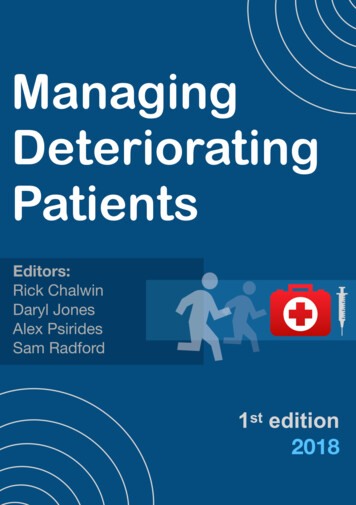
of physiological derangement. The responders aretypically the ward treating doctors under whom thepatient was admitted and who may have 20-30 minto attend.There are several methods by which an RRT can beactivated. These include single parameter systems (wherea team is called if a single vital sign parameter thresholdis breached) and aggregate scoring systems where eachvital sign parameter is assigned a score according to thelevel of derangement. These are then summed togenerate an early warning score (EWS) with the responsedictated by the value of the aggregate EWS. Otheractivation systems include patient, family or staff concern(in the absence of physiological derangement).Hybrid models that combine an aggregate EWS andsingle parameter calling are also described. One suchexample is the New Zealand National Early Warning Scoreimplemented by the Health Quality and SafetyCommission across every acute public hospital in 2018(see Figure 3.1). This matches early detection ofdeterioration with a graded escalation that increases frommore frequent vital sign monitoring, through home teamjunior medical staff, to expert nursing review and finally torapid response team activation for higher aggregatescores or worsening single parameters.Automated systems that are able to continuouslyintegrate multiple parameters including vital signs andlaboratory data are under development and undergoingclinical testing.!2 2
Rapid Response Systems and Rapid Response TeamsOne of the most common reactive systems for improvingthe recognition of and response to clinical deterioration ofhospitalised patients is the Rapid Response System(RRS). The RRS describes a hospital wide approach toprovide a coherent and integrates system of care withfour components.1.The afferent limb. This is the method of identifyingdeterioration, the calling criteria, and the means ofactivating the call2.The efferent limb. This is the responding team,generically referred to as the Rapid Response Team(RRT) or Medical Emergency Team (MET)3.The patient safety and quality improvement limbprovides audit and feedback to constantly improvethe system4.The administrative or governance limb coordinatesresources and provides oversight for the running ofthe entire system.In Australian and New Zealand hospitals with an ICU, thevast majority of RRTs and METs have staff from the ICUas part of the team membership, typically an ICU registrarand/or nurse. Direct consultant involvement in the RRTappears to be relatively uncommon. There is evidencethat the number of RRT calls are increasing, and thatpatients reviewed by the RRT are at increased risk of inhospital morbidity and mortality. For these reasons, it isimportant that ICU advanced trainees and nurses aretrained in the elements of RRT call management,particularly team leadership skills.!2 3
Effectiveness of interventionsIntroduction of ICULN services have been associated withreductions in the risk of ICU readmission, following ICUdischarge. Other reported benefits include reducingdischarge delay as well as patient and family anxietybefore ICU discharge.Introduction of standardised escalation criteria using EWSsystems in Hospitals in Wales and Scotland lead to areduction in mortality from sepsis by 20%. There are nowthree systematic reviews reporting that the introduction ofan RRS is associated with an approximately 30%reduction in the risk of in-hospital cardiac arrests. Inaddition, one of these reviews reported an associationwith decreased all-cause in-hospital mortality.Two studies have suggested improved outcomes ofhospitalised patients with the introduction of ACSQHCconsensus statement in Australia. Thus, amongst morethan 110 ICU-equipped hospitals introduction of thestandard was associated with a reduction in theproportion of ward admissions to ICU associated with acardiac arrest (from 5.6% to 4.1%). In addition, the risk ofin-hospital death for cardiac-arrest related ICUadmissions from the ward was reduced by approximately21%.The second study involved assessment of cardiovascularcomplications for all hospitals in Victoria, including thosewithout an ICU. This study also revealed a reduction in inhospital cardiac arrests in association with the nationalstandard. In addition, there were also reductions in the!2 4
risk of other hospital acquired cardiovascularcomplications.Table 3.1: Overview of hospital-based strategies fordeteriorating patients Measurement and documentation ofvital signs Continuous physiological monitoring inselected patientsPre-emptive Rounding and review by usual clinicians& pro-active Nurse consultantsstrategies Intensive Care Liaison nurses Hospitalists and peri-operativephysicians Elective high dependency and intensivecareReactivesolutions Hospital wide escalation policy Review by usual clinicians when earlydeterioration occurs 'Code Blue' or cardiac arrest teams Intensive Care Liaison nurses Rapid Response Teams!2 5
Table 3.2: Summary of roles and scope of practiceof Intensive Care Liaison NursesTypes ofpatientsreviewed ICU discharges During or following RRT review New referrals from ward staff Patient and carer escalation Education of ward staff, patients andrelativesNonReferring patients of concern to othertechnical hospital staffskills Assessment of patients, review ofperformed investigation Contribution to patient management plan Management of obstructed airway,assisting with endotracheal intubationTechnical Set-up and modify oxygen deliverysystems and/or non-invasive ventilationskills Delivery of medicationperformed Trouble shooting or setting up equipment Insertion of nasogastric tube, venouscannula, or urinary dwelling catheter!2 6
Table 3.3: Some examples of RRT activation criteriaAirwayproblems Obstructed airway Noisy breathing or stridor Problem with a tracheostomy tubeBreathingproblems Any difficulty breathing Respiratory rate 8 or 25 breaths/min SpO2 90% despite high-flow oxygenCirculationproblems Heart rate 40 or 120 beats/min Systolic blood pressure 90 mmHg Urine output 50mL over 4 hrConsciousstateproblems Sudden change in conscious state Patient cannot be roused Prolonged or recurrent seizuresThe staff member is worried for any other reason!2 7
!2 8Figure 3.1: Example of a hybrid early warning score - the New Zealand national system
Further reading:Jones D. Chapter 1. The role of a medical emergencyteam in a teaching hospital. Doctorate Thesis 2009Jones DA, DeVita M, Bellomo R. Current Concepts:Rapid-Response Teams. NEJM. 2011;365:139-46Story DA, Leslie K, Myles PS, Fink M, et.al. Complicationsand mortality in older surgical patients in Australia andNew Zealand (the REASON study): a multicentre,prospective, observational study. Anaesthesia.2010;65:1022-1030ACSQHC. National consensus statement: essentialelements for recognising & responding to acutephysiological deterioration 2nd ed. 2017Mcintyre T, Taylor C, Reade M, Jones D, Baldwin I.Characteristics and outcomes of patients subject tointensive care nurse consultant review in a teachinghospital. Crit Care Resus. 2013;15:134-140Eliott S, Chaboyer W, Ernest D, Doric A, Endacott R. Anational survey of Australian Intensive care unit (ICU)liaison nurse (LN) services. Aust Crit Care. 2012; 25:253-262Martin C, Jones D, Wolfe R. State-wide reduction in inhospital cardiac complications in association withintroduction of a national standard for recognisingdeteriorating patient. Resuscitation. 2017; 121:172-178!2 9
Jones D, Bhasale A, Bailey M, Pilcher D, Anstey MH.Effect of a National Standard for deteriorating patients onIntensive Care admissions due to cardiac arrest inAustralia. Crit Care Med. 2018;46:586-593Health Quality & Safety Commission New Zealand.National deteriorating patient programme. Recognitionand response systems. Visited 13th September 2018Sethi SS, Chalwin R. Governance of rapid responseteams in Australia and New Zealand. Anaesth IntensiveCare 2018;46:304-12!3 0
04. PRINCIPLES OF TEAMMANAGEMENTRick Chalwin, Stuart GillonOverviewThe RRT call is a significant stress burden on the team aswell as the patient. As noted by Gillon et al: "therequirement for a MET response has been described as acrisis, as the patient is at risk of imminent harm or death”.The skills required for the successful management of anRRT call go beyond the theory and technical abilities ofpatient management and are imperative.Various terms describe this skill set such as crisisresource management (CRM) and non-technical skills. Allsystems share the same principles of establishing teamroles and responsibilities, building adaptability andresilience, and achievin
Sam Radford !3. Editors (listed alphabetically) Dr. Rick Chalwin MBChB FCICM MPH Staff Specialist, Intensive Care Unit, Lyell McEwin Hospital, South Australia Senior Lecturer, Adelaide Health Simulation, University of Adelaide PhD Candidate, School of Public Health, University of Adelaide A/Prof Daryl Jones BSc (Hons) MB BS FRACP FCICM MD PhD