Transcription
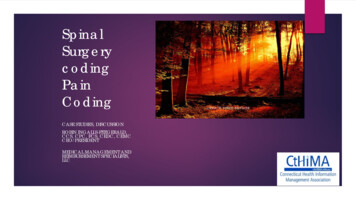
Evidence Based MedicineinSpinal SurgeryRoger Härtl, MDAssociate Professor of NeurosurgeryChief of Spinal SurgeryNeurosurgeon to the GIANTS Football teamBrain & Spine CenterWeill Cornell Medical CollegeNew York, NY, USA
Disclosure– Synthes Consultant– Baxter Fellowship funding / Consultant– Spinewave Consultant– BrainLab Consultant– Lanx Consultant– AOSpine AOSpine NA Board Fellowship funding Research funding
Back Pain Degenerative Discdisease Disc herniation Spinal stenosis Congenital anomalies– Spondylolisthesis “Slippage” Trauma– Sprains and Strains– Fractures Facet-joint pain Sacro-iliac joint pain Neoplasm, infection,referred pain
Dr. Rauschning
Types of low back pain Radicular pain; Sciatica– Herniated disc– Foraminal stenosis Neurogenic claudication– spinal stenosis Chronic low back pain– DDD– “instability” Referred pain: hips, knees
OrthopedicsFor 95%of ySurgeryCornellSpineCenterPhysiatry /PainManagementComplementaryMedicineNeurology
Non-operativemanagement At least 6 weeks Limited bedrest, early mobilization Exercises / PT– Aerobic, stretching, isometric
100 patients with low backpain
100 patients with low backpain
100 patients with low backpainOROR
What happens if nonoperative treatment fails?
The Role of Surgery- Short answer -Neck / back painRadiculopathy pain goingdown the legMyelopathy /Cauda equina Spinal cord ornerve injury
The Role of Surgery- Short answer - Factors that favor Surgery– Clinical findings and MRI findings fit– Failure of non-operative treatment– Severe Pain– Neurological deficit Weakness Bowel / bladder incontinence– Leg or arm pain or weakness
What is Evidence BasedMedicine?The use of clinical methods anddecision making that have beenthoroughly tested by properlycontrolled peer-reviewedmedical research.
Evidence Based MedicineClass I– Prospective, Randomized, Controlled TrialsClass II– Non-Randomized, Prospective ControlledTrials– Observational StudiesClass III– Case Series– Case Reports– Expert Opinion
Evidence Based MedicineLevel 1 Recommendation–Class I EvidenceLevel 2 Recommendation–Class II EvidenceLevel 3 Recommendation–Class III Evidence
Treatment AStudy SampleOutcome ARandomizationTreatment BOutcome BDiagram demonstrating the basic design of a RANDOMIZED CONTROLLED TRIAL. Thestudy sample is randomized to different treatments, and the outcomes are prospectivelydetermined.The Importance of Study Design in the Spine Literature, Pearson A.,et.al.Seminars in Spine Surgery, Vol 21 (4), Dec 2009
Treatment AOutcome ATreatment BOutcome BDiagram demonstrating the basic design of an OBSERVATIONAL COHORT STUDY. Thetreatment is chosen by the patient and physician rather than through randomization. Thestudy groups are defined by treatment and outcomes are compared. Cohort studies canbe prospective or retrospective.The Importance of Study Design in the Spine Literature, Pearson A. et.al.Seminars in Spine Surgery, Vol 21 (4), Dec 2009
Evidence Based Medicine:Spine Lumbar HNP (3)Lumbar stenosis (3)Degenerative spondylolisthesis (5)Axial LBP (4)Artificial disc (3)
LUMBARHERNIATEDNUCLEUSPULPOSUS
Case example: HerniatedLumbar Disk 43 y/o male with 2 months ofpain radiating into right foot No relieve by physical therapyand medication No back pain, weakness orurinary incontinence No “red flags”
S1L5L4L3
EBM-Spine: Lumbar HNPPeul WC et al NEJM 2007DesignMulticenter RCT with ITT AnalysisPatients141 Patients- early surgery (median: 1.9 weeks)142 Patients- non-operative managementResultsEarly surgery resulted in faster recoveryNo difference in outcomes in 1 yearLimitationsHigh cross-over rates11% of surgery Æ conservative39% of conservative Æ surgeryBlinding not possibleFollow-up only 1 year
EBM Spine: Lumbar HNPAtllas SJ, et. al. Spine 2005 (Maine Lumbar Spine Study)DesignProspective Cohort Study (observational)Patients235 Surgery272 ConservativeResultsSurgery: Improved in pain, function and satisfactionoutcomes at 1, 5 and 10 years.No difference in work status, surgery vs. conservative.Benefit of surgery narrowed between the two groups overtime but still statistically different at 10 years.LimitationsImaging not requiredMail in questionnaire rather than actual clinical exam.
EBM Spine: Lumbar HNPSpine Patient Outcomes Trial (SPORT)Weinstein JN , et.al. JAMA 2006, Spine 2008Design2 Combined Trials (Due to protocol non-adherence)RCT- 501 PatientsObservational Cohort- 743Patients1244 totalResultsSurgery resulted in greater improvement comparedwith non-operative treatment at 4 years.LimitationsCross over (40% of surgery group, 45% of nonoperative). This precluded meaningful analysis of thedata on an ITT basis because the 2 groups were verysimilar in treatment received at 2 years.
LUMBARSTENOSIS
EBM Spine: StenosisThe Finnish Spinal Stenosis StudySimotas A.C., Clin. Orthopedic Relat Res 2001DesignRCT with ITT AnalysisPatients94 Patients, (50 Surgical, 44 Non-surgical)ResultsSurgery better in ODI, leg and back pain. Greater difference at 1year than at 2 yearsCrossover rate 10% (low) in either direction.Level I evidence favoring surgery but not in walking abilityLimitationsSmall number of patients20% of surgery group had instrumented fusion (variation insurgical management)
EBM Spinal: StenosisMaine Lumbar Study Atlas SJ et al, Spine 2005DesignProspective observational Cohort10 year follow-upPatients148 Patients- (81 Surgical, 67 Nonsurgical)ResultsLevel 2 evidence that decompression MAY provide betteroutcomes over nonsurgical treatment.LimitationsCross over to surgery 39%Non-randomized: more severe patients to surgery.Few patients with mild symptoms were treated with surgery
EBM Spine: StenosisSport Trial for Lumbar Spinal StenosisWeinstein J, et. al., NEJM 2008, Spine 2010DesignRCT with prospective observational CohortPatients654 Patients (289 RCT, 365 Observational)ResultsLevel 2 evidence to suggest that surgery results in betteroutcome at 2 years and maintained at 4 years.LimitationsHigh cross over– 33% of surgery group to non-surgery group– 43% from non-surgery group had surgerySurgical treatment variable (11% had a fusion)Non-surgical treatment not specified
DEGENERATIVESPONDYLOLISTHESIS
EBM:Degenerative SpondylolisthesisSurgical vs. Nonsurgical Treatment for LumbarDegenerative SpondylolisthesisWeinstein J. et. al. NEJM 2007, JBJS 2009DesignRCT with prospective observational cohort(304 RCT, 303 Observational Cohort)Patients521 Patients Follow-up, (372 Surgery, 149 No-surgery)ResultsSurgery patients (laminectomy with 1 level fusion) hadsubstantially greater pain relief and improvement in function at 4years.LimitationsHigh level of cross over, difficult to interpret ITT analysis36% of surgery group, 49% of non-operative groupNon-operative treatment not standardizedSurgical treatment not standardized(fusion posteriorly or circumferentially with or withoutinstrumentation)
EBM:Degenerative SpondylolisthesisThe Surgical Management of Degenerative LumbarSpondylolisthesis: A Systemic Review.Martin CR et.al. Spine 2007DesignLiterature Review: RCT and comparative observational studies inEnglish, German and French (1966-2005)Patients13 Studies of 578 patientsResultsFusion is more effective than laminectomy in achieving asatisfactory outcomeInstrumentation increased fusion rateDecompression only had the least satisfactory outcomeLimitationsSome studies included non-consecutive patientsSome had undefined follow-upNo standardized outcome measure was used consistentlyStrenghtsComprehensive review on degenerative spondylolisthesis
EBM: Degenerative Spondylolisthesis”Degenerative Lumbar Spondylolisthesis with SpinalStenosis” Kornblum, et.al. Spine 2008DesignA Prospective Long Term Study “Comparing Fusion and Pseudoarthrosis”Patients58 Patients with laminectomy and non-instrumented fusionResultsGood or excellent outcome in86% fusion56% non-union25/47 (53%) developed non-unionStrengthsFollow-up was long (5-14 years)LimitationsSmall numberNon-standardized outcome measure19% (11 patients) lost to follow-upSingle center, secondary analysis
EBM:Degenerative SpondylolisthesisSurgical Treatment of Spinal Stenosis withSpondylolisthesis: Cost Effectiveness after 2 yearsTosteson AN et al, Ann Internal Medicine 2008DesignProspective Cohort StudyPatients601 Patients (randomized and observational cohort)368 Surgery (fusion in 93% / 78% instrumentation)233 Non-surgeryResultsA trend toward improved cost effectiveness with circumferentialinstrumented fusionSurgery results in better improvement of healthStrengthsMulticenter studyLarge number of patientsRCT and observational patientsValidated outcome measure usedLimitationsNon-operative care not specifiedCosts relied upon self-reported utilization dataFollow-up limited to 2 years
AXIALLOW BACK PAIN
EBM: Axial Low Back PainLumbar Fusion Versus Treatment of Chronic Low Back Pain:A Multicenter Randomized Controlled Trial From the SwedishSpine Study Group Fritzell P, et al Spine 2001DesignMulticenter RCT with 2 year follow, ITT AnalysisPatients292 (Fusion 222, Non-operative 72)ResultsFusion may lead to better outcomeStrengthsMulticenter RCT small dropout (5 patients)LimitationsNo standardization in either groupIndustry fundingAsymmetry of group sizes 75 (due to design as multiple fusionarms)
EBM: Axial Low Back PainRandomized Controlled Trial to Compare SurgicalStabilization of the Lumbar spine with IntensiveRehabilitation for Patients with Chronic Low Back Pain:The MRC Spine Stabilization Trial. Fairbank et al BMJ 2005DesignMulti-centre RCT with 2 year follow-upPatients349 Patients (179 Surgery, 170 Rehab)ResultsImprovement above rehabilitation in ODI (4.1) with surgery (barelystatistically significant)StrengthsMulticenter RCTMultiple outcome measures (ODI, walking test, SF36, work status)LimitationsHigh crossover (28% non-operative to rehabilitation)Included redo’s and spondylolisthesisFlexible stabilsations included as fusion
EBM: Axial Low Back PainRandomized Clinical Trial of Lumbar Instrumented Fusionand Cognitive Intervention in Patients with Chronic Low BackPain and Disc Degeneration. Brox et al Spine 2003DesignRCT with 1 year follow-upPatients64 patientsResultsBoth groups improved significantly and equallyStrengthsBlinding of physical therapy evaluatorStandardized nonsurgical treatmentLimitationsShort follow-upSmall numbersLack of no treatment armFailure of treatment in assigned group (4/37 of the surgery groupand 2/27 in non-surgical)
EBM Spine: Axial LBPLumbar Instrumented Fusion Compared with Cognitive Interventionand Exercises in Patients with Chronic Low Back Pain After PreviouSurgery for Disc Herniation: A Prospective Randomized ControlledStudy. Brox et al Pain 2006DesignNationwide (Norway) RCT with 1 year follow-up and ITT AnalysisPatients60 PatientsResultsNo DifferenceStrengthsRCTValidated outcome measuresBlinding of PT evaluatorLimitationsShort follow-up (1year)Small numbersLack of no treatment arm7/29 Did not have surgery, 2/31 Did not have non-surgical
ARTIFICIALDISC
EBM: Artifical DiscResults of Prospective, Randomized, Multicenter Food & DrugAdministration Investigational Device Exemption Study of Pro Disc-LTotal Disc Replacement vs. Circumferential Fusion for the Treatmentof 1 Level Degenerative Disc Disease Zigler et al Spine, 2007DesignMulticenter randomized controlled non-inferiority trial with 2 year follow-upPatients161 pro-disc patients, 75 fusion patientsResultsStudy suggests that short-term outcomes of artificial disc replacements aresimilar to or marginally better than fusionStrengthsRCTLimitationsIndustry fundingAbout 10% lost to follow-up in each groupFDA revision of success criteria
EBM: Artifical DiscA Prospective Randomized Food and Drug AdministrationInvestigational Device Exemption Study: Lumbar Total DiscReplacement with the Charité Artificial Disc vs. Lumbar Fusion. PartI: Evaluation of Clinical Outcome. Bleumenthal S, et al Spine, 2005DesignMulticenter RCT non-inferiority trial with 2 year follow-upPatients304 Patients. (205 Artificial Disc, 99 Anterior lumbar (BAK cageand autograft))ResultsSuggest that short term outcomes are similar or slightly betterwith artificial discStrengthsMulticenter RCTLimitationsLarge loss to follow-up (44 in disc group, 33 in fusion group)Industry funding72% of the disc replacement group and 86% of fusion group in theclinically “successful” results were still on narcotics at 2 years.
EBM:Cervical Artificial DiscCombined Results of 3 US IDE Randomized CervicalArthroplasty Trials with 2 years Follow-Up Upadhyaya et alNeurosurgery, 2010 (Abstract)DesignProspective randomized multicenter trials evaluating implants2 year follow-up605 study/561 controlPatientsPrestige- 276 study/265 controlBryan- 242 study/221 controlProDisc- 163 study/106 controlResultsSecondary surgery3.1% study group vs. 8.2% control (fusion)StrengthsLarge multicenter RCTLimitationsIndustry supportedShort follow-up
Conclusions from these StudiesLumbar HNPEarly surgery, faster recoverySurgery, greater improvementLumbar StenosisSurgeryDegenerative SpondylolisthesisSurgery – fusion with instrumentation
Conclusions from these StudiesAxial LBPConservative vs Surgery: NodifferenceArtificial DiscVerdict not inNONE are really Class I evidence
Studies in the FutureFor Axial LBPStudies to compare: fusion and structured post-op rehab to structured rehab only to a non-structured non-operativearmFor Axial LBPstudies examining the longevity andlong term complication of artificialdisc
Studies in the FutureFor lumbar stenosisstudies use validated oucomes (SSS/Zurichclaudication questionnaire)For degenerative spondylolisthesisThere is no randomized controlled trial with longterm follow-up comparing the various fusiontechniquesFuture studies will need to be:Not just effective but cost effective
Other questions remain .Timing of the surgery?Specific surgical technique?(e.g. various fusion approaches)The place for new technologydisc arthroplasty?dynamic stabilization?BMP?
Alternatives to EBM based onRandomized Control Trial (RCT)Observational cohort studyBest evidence & good judgmentPersonalized medical treatments
EBM – Spine: Observational Studiesfor Providing the Best Answersto Some Questions“RCT & Observational study designtypically yield the same answer”Benson K, Hartz AJ, NEJM 2000Cancato et al NEJM 2000OBSERVATIONAL STUDY Lower costs Easier patient recruitmentRCTExtremely Expensive And WorkIntensive 3 SPORT Studies - 12 million Difficult to obtain long termfollow-up (SPORT IDH 35% lostto follow-up at 4 years).
BEST EVIDENCEANDGOOD JUDGMENT
EBM in Spine Practice“Evidence-based medicine is theconscientious, explicit and judicious use ofcurrent best evidence in making decisionsabout the care of individual practice.”“EBM is not restricted to randomized trialsand meta analysis.”Evidence Medicine: Which is it and which is notSackett, et al BMJ 1996
“It involves integrating individualclinical expertise with bestavailable external clinicalevidence from systemicresearch.”Individual Clinical Expertise: Clinician experience and practiceExternal Clinical Evidence: Clinically relevant research
EBM:Cervical Artificial Disc Combined Results of 3 US IDE Randomized Cervical Arthroplasty Trials with 2 years Follow-Up Upadhyaya et al Neurosurgery, 2010 (Abstract) Design. Prospective randomized multicenter trials evaluating implants. 2 year follow-up 605 study/561 control. Patients. Prestige- 276 study/265 control. Bryan- 242 study/221 control