Transcription
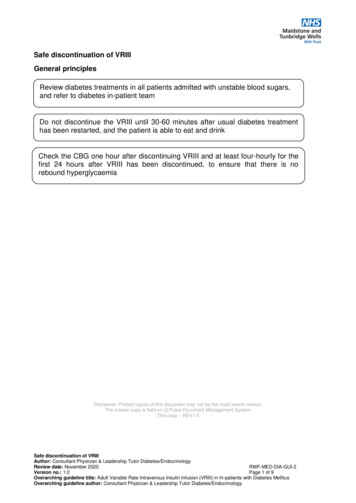
Safe discontinuation of VRIIIGeneral principlesReview diabetes treatments in all patients admitted with unstable blood sugars,and refer to diabetes in-patient teamDo not discontinue the VRIII until 30-60 minutes after usual diabetes treatmenthas been restarted, and the patient is able to eat and drinkCheck the CBG one hour after discontinuing VRIII and at least four-hourly for thefirst 24 hours after VRIII has been discontinued, to ensure that there is norebound hyperglycaemiaDisclaimer: Printed copies of this document may not be the most recent version.The master copy is held on Q-Pulse Document Management SystemThis copy – REV1.0Safe discontinuation of VRIIIAuthor: Consultant Physician & Leadership Tutor Diabetes/EndocrinologyReview date: November 2020RWF-MED-DIA-GUI-2Version no.: 1.0Page 1 of 9Overarching guideline title: Adult Variable Rate Intravenous Insulin Infusion (VRIII) in In-patients with Diabetes MellitusOverarching guideline author: Consultant Physician & Leadership Tutor Diabetes/Endocrinology
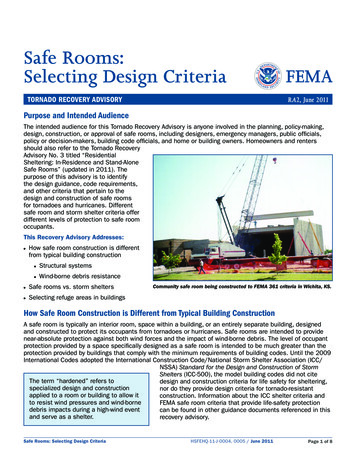
Restarting oral and injectable hypoglycaemic agentsRecommence oral and injectable hypoglycaemic agents once the patient is able to eat anddrink. Ensure that no contraindications to the previous hypoglycaemic therapy have arisen.Review diabetes treatment in all patients admitted with unstable blood sugars, and refer tothe in-patient diabetes team.Table 1. Restarting Therapy in Patients with Type 2 DiabetesGood control(HbA1c 58mmol/mol or7.5%)Diet aloneOral hypoglycaemic GLP-1 mimetics (injectable)therapyDiscontinueVRIII whenthe patient isstable.Restart usual diabetes Most patients will be takingtreatment when aadditional oral hypoglycaemicmeal is due.treatments, which should beDo not stop VRIII until restarted when a meal is due.at least 30 minutesafter treatment hasbeen given and thepatient has eaten.Some patients mayalso be on basalinsulin (see Table 5for additional advice).Suboptimalcontrol(HbA1c 58mmolmol or7.5%)Monitor bloodglucoseGLP-1 mimetics should berecommenced at the usualdose and time.Do not stop VRIII until at least30 minutes after treatment hasbeen given and the patient haseaten.In addition to above, discuss with diabetes in-patient team.Patient may need additional hypoglycaemic therapy depending onindividualised goals.CBG should be checked one hour after discontinuing VRIII and at leastfour-hourly for the next 24 hours, to ensure that there is no reboundhyper or hypo-glycaemia.Considerations Dose of insulin secretagogues eg sulphonylureas or glinides may needto be reduced if food intake is likely to be limited.Metformin should only be recommenced when eGFR is 30ml/min.Review GLP-1 mimetics and DPP4 inhibitors (gliptins) if patient wasadmitted with suspected pancreatitis.Review glitazone therapy if patient was admitted with heart failure, hasmacular oedema or has been admitted with a lower limb fracturefollowing a fall.Review SGLT-2 inhibitor therapy if patient was admitted with urogenitalinfection or diabetic ketoacidosis.Safe discontinuation of VRIIIAuthor: Consultant Physician & Leadership Tutor Diabetes/EndocrinologyReview date: November 2020RWF-MED-DIA-GUI-2Version no.: 1.0Page 2 of 9Overarching guideline title: Adult Variable Rate Intravenous Insulin Infusion (VRIII) in In-patients with Diabetes MellitusOverarching guideline author: Consultant Physician & Leadership Tutor Diabetes/Endocrinology
Restarting insulin for patients previously on subcutaneous insulinConvert to subcutaneous insulin when the patient is able to eat and drink and hasmanaged at least one meal. Ideally the transfer should take place at a mealtime, usuallybreakfast or lunch. Ensure that background insulin (either long-acting analogue orisophane) has been given before the VRIII is withdrawn (3).The VRIII should be continued until at least 30 minutes after the administration of asubcutaneous dose of insulin. This is to avoid rebound hyperglycaemia.Most patients will restart their normal regime (see Table 5 for detailed advice). The preadmission dose of insulin may need to be reduced if food intake is likely to be limited orthe patient was admitted with low blood sugars.Review diabetes treatment in all patients admitted with unstable blood glucose or HbA1c 58mmol/mol (7.5%), and refer to the diabetes inpatient team.Safe discontinuation of VRIIIAuthor: Consultant Physician & Leadership Tutor Diabetes/EndocrinologyReview date: November 2020RWF-MED-DIA-GUI-2Version no.: 1.0Page 3 of 9Overarching guideline title: Adult Variable Rate Intravenous Insulin Infusion (VRIII) in In-patients with Diabetes MellitusOverarching guideline author: Consultant Physician & Leadership Tutor Diabetes/Endocrinology
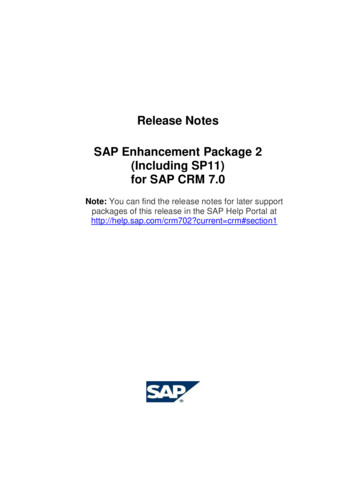
Table 2. Guidance for restarting insulin in patients according to previous regimesGood Control (HbA1c 58mmol/mol or 7.5%)BasalinsulinOnce ortwicedailymixedinsulinSuboptimal Monitoring bloodcontrolglucoseIn addition,discuss withlocaldiabetes inpatientteam.Restart usual dose of insulin together with a meal (either breakfast or evening meal). Do not stop InsulinVRIII until at least 30 minutes after insulin has been given and the patient has eaten.regime mayIf it is necessary to stop VRIII at lunchtime, give half the usual breakfast dose of mixed insulin. needadjustingThis will provide essential background insulin until the usual dose can be recommenced.Restart usual dose of insulin when it is due (usually with either breakfast or evening meal).Do not stop VRIII until at least 30 minutes after insulin has been given and patient has eaten.If it is necessary to stop VRIII but the basal insulin is not due for several hours, give half theusual dose of basal insulin. This will provide background insulin until the usual dose can berecommenced.Multipledailyinsulininjections(MDI orbasalbolus)Restart usual diabetes treatment together with a meal.Basal insulin will usually have been continued. Restart bolus dose of insulin together with thenext meal. Do not stop VRIII until at least 30 minutes after bolus insulin has been given and thepatient has eaten.If basal insulin has been stopped, background insulin must be restarted prior to stopping VRIII.Ideally, continue the VRIII until basal insulin is given and a meal is due, and stop at least 30minutes after basal and bolus insulin is restarted.If it is necessary to stop the VRIII, but the basal insulin is not due for several hours, give half theusual daily dose of basal insulin, along with a meal and bolus insulin. This will provide essentialbackground insulin until the usual dose can be recommenced.Insulinpump(CSII)Restart usual basal rate via CSII.Ideally stop VRIII at least 30 minutes after first meal-time bolus of insulin has been given viaCSII. Avoid restarting CSII at bedtime.Safe discontinuation of VRIIIAuthor: Consultant Physician & Leadership Tutor Diabetes/EndocrinologyReview date: November 2020RWF-MED-DIA-GUI-2Version no.: 1.0Page 4 of 9Overarching guideline title: Adult Variable Rate Intravenous Insulin Infusion (VRIII) in In-patients with Diabetes MellitusOverarching guideline author: Consultant Physician & Leadership Tutor Diabetes/EndocrinologyCBG should bechecked one hourafter discontinuingVRIII and at leastfour-hourly for thenext 24 hours, toensure that thereis no reboundhyper- or hypoglycaemia
Calculating subcutaneous insulin dose in insulin-naïve patients, or whereinsulin regime needs altering because of sub-optimal controlIt is important that patients starting insulin receive education and support inself-management of diabetes that they are confident to self-inject prior todischarge, and that follow-up support is available from appropriately trainedprofessionals.If the insulin dose is uncertain because the patient is new to insulin or has previouslyhad poor control there are two possible ways of calculating the starting dose. Thereis no evidence on which to base a recommendation. The following guidelines aresuggestions only, and detailed advice should be sought from local protocols and thediabetes team.The options are: Method A- weight based calculationMethod B- Based on insulin requirements during the stable phase of the VRIIISafe discontinuation of VRIIIAuthor: Consultant Physician & Leadership Tutor Diabetes/EndocrinologyReview date: November 2020RWF-MED-DIA-GUI-2Version no.: 1.0Page 5 of 9Overarching guideline title: Adult Variable Rate Intravenous Insulin Infusion (VRIII) in In-patients with Diabetes MellitusOverarching guideline author: Consultant Physician & Leadership Tutor Diabetes/Endocrinology
Step 1- Calculate the Total Daily Dose (TDD) requirement usingeither method A or B. Step 2- Use the TDD to convert the patient to either a premixedtwice daily insulin regime or a multiple dose regime- basal bolus.o For a basal-bolus regime, 50% of the total insulinrequirement is usually given as basal insulin, and theremainder as rapid-acting insulin, divided equally betweenbreakfast, lunch and evening meal.o For a twice-daily, pre-mixed insulin regime, patients usuallyneed 60% of the total insulin requirement at breakfast andthe remaining 40% with the evening meal. Step 3- Review response to any new insulin regime prior todischarge.o CBG should be checked one hour after discontinuing VRIII,at least four-hourly for the first 24 hours after VRIII hasbeen discontinued, and between two and four times a dayfor all in-patients on subcutaneous insulin.o Adjust the doses of insulin according to blood glucosemeasurements. A target of 6.0-10.0 mmol/L is appropriatefor most in-patients, but patients with significant comorbidities may benefit from less stringent targets (4.012.0mmol/l).o Ensure the patient and carers are confident in using theinsulin delivery device prior to resuming self-management.Refer to the in-patient diabetes team for education andsupport.Safe discontinuation of VRIIIAuthor: Consultant Physician & Leadership Tutor Diabetes/EndocrinologyReview date: November 2020RWF-MED-DIA-GUI-2Version no.: 1.0Page 6 of 9Overarching guideline title: Adult Variable Rate Intravenous Insulin Infusion (VRIII) in In-patients with Diabetes MellitusOverarching guideline author: Consultant Physician & Leadership Tutor Diabetes/Endocrinology
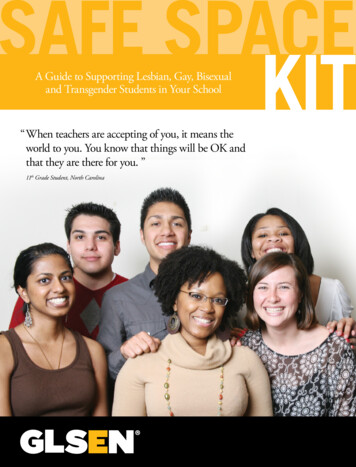
Method A: Calculating estimated insulin dose frompatient’s weightInsulin requirements for an adult patient can be calculatedfrom a weight-based formula (see worked example). Frail elderly patients, significant renal impairment (CKDstage 4 or 5), severe hepatic failure, newly diagnosedtype 1 diabetes:Total daily insulin dose 0.3 x body weight in kgAll other adult patients: Total daily insulin dose 0.5 xbody weight in kgWorked Example using method APatient with CKD Stage 4 weighs100 kgTotal daily insulin requirement(TDD) 0.3 x body weight100 kg0.3 x 100 30 unitsBasal bolus insulin regime (MDI)*Basal dose: 30 2 15 unitsGive half of TDD as basal insulinand divide the remainder by threefor bolus doses with each mealBolus dose: 15 3 5 units with eachmealTwice-daily pre-mixed insulinregime*Breakfast dose:60% 18 unitsGive 60% of total daily requirement(TDD) with breakfast and 40% withevening mealEvening meal:40% 12 units*For specific insulin brands to be used, see localformulary and stock lists, or seek advice of in-patientdiabetes teamSafe discontinuation of VRIIIAuthor: Consultant Physician & Leadership Tutor Diabetes/EndocrinologyReview date: November 2020RWF-MED-DIA-GUI-2Version no.: 1.0Page 7 of 9Overarching guideline title: Adult Variable Rate Intravenous Insulin Infusion (VRIII) in In-patients with Diabetes MellitusOverarching guideline author: Consultant Physician & Leadership Tutor Diabetes/Endocrinology
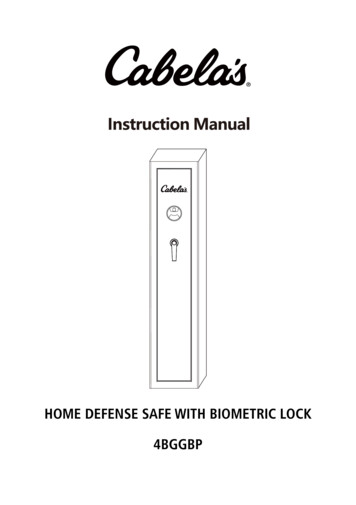
Method B: Calculating estimated insulin dose frominsulin requirements during the VRIIIThe daily insulin requirement can be estimated from the last 6hours of the VRIII as follows:Divide the total dose of insulin administered in last 6 hours ofthe VRIII by 6 to calculate average hourly dose of insulin.Multiply this by 20 (not 24, to reduce risk of hypoglycaemia) toestimate the patient’s total daily insulin requirement. A furthercorrection may be needed in some patients, depending onindividual insulin sensitivity, previous degree of glycaemiccontrol and severity of intercurrent illness.Worked example using method B:Total dose of insulin administered inlast 6 hours (6 times hourly rate)12 unitsDivide by 6 to calculate hourly dose12 6 2 unitsMultiply by 20 (not 24 to reduce risk ofhypoglycaemia) to estimate total dailyinsulin (TDD) requirement2 x 20 40 unitsBasal bolus insulin regime (MDI)*Basal dose: 40 2 20 unitsGive half of TDD requirement as basalinsulin and divide the remainder bythree for bolus doses with each mealTwice-daily pre-mixed insulin regime*Give 60% of TDD with breakfast and40% with evening meal*For specific insulin brands to be used, see localformulary and stock lists, or seek advice of in-patientdiabetes teamSafe discontinuation of VRIIIAuthor: Consultant Physician & Leadership Tutor Diabetes/EndocrinologyReview date: November 2020RWF-MED-DIA-GUI-2Version no.: 1.0Page 8 of 9Overarching guideline title: Adult Variable Rate Intravenous Insulin Infusion (VRIII) in In-patients with Diabetes MellitusOverarching guideline author: Consultant Physician & Leadership Tutor Diabetes/EndocrinologyBolus dose: 20 3 7 units witheach mealBreakfast dose:60% 24 unitsEvening Meal:40% 16 units
Patients on continuous subcutaneous insulin infusion (CSII) (insulin pumptherapy) The inpatient diabetes team should be involved with all patients on a CSII, togive individual advice. In most patients, the previous basal subcutaneous insulin regime should berestarted via the CSII. Continue the VRIII for at least 30 minutes after CSII isrestarted, to avoid rebound hyperglycaemia, and ideally in relation to a meal. Avoid restarting CSII at bedtime, because of the risk of reboundhyperglycaemia overnight. The CSII should not be recommenced until the patient is capable of managingit. Consult the patient about their pump management as patients are usuallyvery knowledgeable about their device.Safe discontinuation of VRIIIAuthor: Consultant Physician & Leadership Tutor Diabetes/EndocrinologyReview date: November 2020RWF-MED-DIA-GUI-2Version no.: 1.0Page 9 of 9Overarching guideline title: Adult Variable Rate Intravenous Insulin Infusion (VRIII) in In-patients with Diabetes MellitusOverarching guideline author: Consultant Physician & Leadership Tutor Diabetes/Endocrinology
from a weight-based formula (see worked example). Frail elderly patients, significant renal impairment (CKD stage 4 or 5), severe hepatic failure, newly diagnosed type 1 diabetes: Total daily insulin dose 0.3 x body weight in kg All other adult patients: Total daily insulin dose 0.5 x body weight in kg Worked Example using method A Patient .