Transcription
Illustration by Matt Herring AN NP EXCLUSIVE30th AnnualAPRN Legislative UpdateImproving access to healthcare one state at a timeBy Susanne J. Phillips, DNP, APRN, FNP-BC, FAANPAbstract: The Annual Legislative Updatedescribes recent legislative changes topractice, reimbursement, and prescriptiveauthority that have the most impact onNPs and other advanced practice nursesacross the country.n 2017, over 20 states passed legislation thatpositively impacted access to and delivery ofhealthcare to patients nationwide. As in previous years, professional advanced practice registerednurse (APRN) organizations and Boards of Nursing(BONs) have worked tirelessly in their respective legislative sessions to ensure patients have access to highquality healthcare services in their states. Following isa summary of legislative advancements pertaining topractice authority, reimbursement, and prescriptiveauthority in 2017.IKeywords: advanced practice registered nurses, APRNs, healthcare reform, legislative update, nurse practitionerswww.tnpj.comThe Nurse Practitioner January 2018Copyright 2018 Wolters Kluwer Health, Inc. All rights reserved.27
30th Annual APRN Legislative UpdateTwo states in particular are highlighted for theirsubstantial and successful efforts in moving towardfull-practice authority. Lawmakers have recognizedthe importance of APRN practice and their impacton access to and delivery of high-quality healthcare inSouth Dakota and Illinois. These states join a growinglist of states that have passed full-practice authority(FPA) with and without exceptions following a periodof supervision, collaboration, or consultation with anAPRN and/or physician following licensure since enactment of the Patient Protection and Affordable CareAct in 2010 (see Summary of practice authority for NPs).On September 20, 2017, Illinois enacted PublicAct 100-0513, extending FPA to APRNs after attaining national certification and following a transitionto practice period, including 250 hours of continuingeducation or training and 4,000 hours of clinical experience in collaboration with a physician. The definition of FPA in Illinois excludes authority to prescribebenzodiazepines and Schedule II controlled substancenarcotic medications. APRNs must maintain a consultation relationship with a physician if these medications will be prescribed by an APRN; the relationshipmust be recorded in a Prescription Drug MonitoringProgram (PDMP) by the physician and APRN.The transition to practice period and exclusion ofbenzodiazepines and Schedule II controlled substancenarcotic medications within the FPA definition doescompletion of 1,040 hours of practice in collaboration with a physician, CNP, or CNM. The BON nowsolely regulates both CNPs and CNMs, and FPA includes prescriptive authority for legend and scheduledcontrolled substances, without exception, identifyingSouth Dakota as full practice by the AANP.1 Pleasesee the individual state descriptions for additionalinformation. Practice authorityMajor accomplishments in the area of practice authority for NPs during the 2017 legislative session includedthe passage of global and partial signature authority,recommendation for medical marijuana use, adoptionof the APRN Consensus Model recommendations onAPRN role recognition and educational programs, aswell as clarification on ownership of medical corporations and minor surgical procedure authorization.Signature authority. Six states enacted legislationpertaining to full or partial global and partial signature recognition and authority, including APRNauthorization for certain aspects of care. Global signature authority is generally defined as authorizationfor recognized APRNs to sign, certify, or endorse alldocuments related to healthcare within their scope ofpractice (SOP) provided for their patients. Some stateslimit these documents (partial) to a statutorily authorized list, while others are broader in their approach.APRN authority to sign deathcertificates among other documentsTwo states in particular are highlighted foris particularly important and wasaccomplished in Arkansas (Act 372;their substantial and successful efforts inenacted March 2017), Minnesotamoving toward full-practice authority.(HF 2177; effective May 2017),Nevada (Chapter 318; effectivenot apply to an APRN when privileged to practice in January 2018), Texas (SB 919; effective June 2017),a hospital, hospital affiliate, or ambulatory surgical and Wyoming (Chapter 160; effective March 2017).treatment center. Although the statutory definition North Carolina (Act 2017-111; effective July 2017)for FPA does not meet the standard for full practice enacted legislation adding NPs to the list of providersaccording to the AANP1, the state’s sponsoring leg- authorized to sign handicap parking certificates.Recommendation for medical marijuana use. Theislators and APRNs feel the positive impact this newauthority will have on access to care outweighs the District of Columbia joins Connecticut, Hawaii,narrow area of practice where physician consultation Maryland, Maine, and New York as states/districtsthat authorize APRNs as providers who may recomis still a requirement.On February 23, 2017, South Dakota’s gover- mend the use of medical marijuana to a qualifyingnor signed Senate Bill 61 into law, removing the re- patient with a qualifying medical condition as dequirement of a collaborative agreement and thereby scribed. Act 21-565, Medical Marijuana Omnibusadopting FPA for certified nurse practitioners (CNPs) Amendment Act of 2016, was issued December 16,and certified nurse midwives (CNMs) after verified 2016. This authority does not confer prescriptive28 The Nurse Practitioner Vol. 43, No. 1Copyright 2018 Wolters Kluwer Health, Inc. All rights reserved.www.tnpj.com
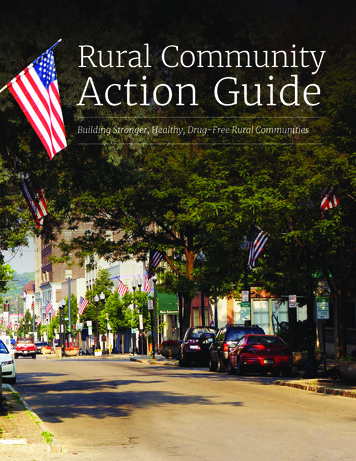
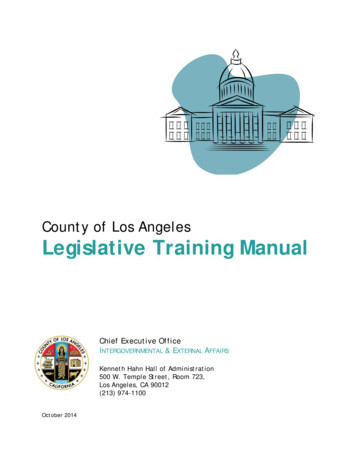
30th Annual APRN Legislative UpdateSummary of Practice Authority for KFLHIFull Practice NPs are regulated by a BONand have full, autonomouspractice and prescriptiveauthority without a requirementor attestation for physiciansupervision, delegation,consultation, or collaboration:AK, AZ, DC, HI, IA, ID, MT, ND,NH, NM, OR, RI, WA, WYFull Practice or Reduced Practicewith Transition NPs are regulated by a BONand have full autonomouspractice and prescriptiveauthority but require a postlicensure/certification period ofsupervision, collaboration, ormentorship: CO*, CT, DE*, MD*,ME*, MN*, NE, NV*, SD*, VT*, WV *[Washington, D.C. is included as a state in this table.]CO: 1,000-hour post-licensure practice periodCT: 3-year and a minimum of 2,000-hour post-licensure practice periodDE: 2-year and a minimum of 4,000-fulltime-hour post-licensure periodMD: 18-month post-licensure practice periodME: 24-month post-licensure practice periodMN: 2,080-hour post-licensure practice periodNE: 2,000-hour post-licensure practice periodNV: 2-year or 2,000-hour post-licensure practice periodSD: 1,040-hour post-licensure practice periodVT: 2-year and 2,400-hour post-licensure practice periodNY: 3,600-hour post-licensure practice period and attestation of physiciancollaboration requiredauthority as marijuana is listed as a Schedule I controlled substance by the Drug Enforcement Administration (DEA). Designated APRNs in these states haveauthority to recommend the use of this substance asdescribed by each state’s law.www.tnpj.comReduced or Restricted Practice NPs are regulated by a BON or acombination of BON and BOMoversight exists; requirement orattestation for physician supervision,delegation, consultation, orcollaboration for authority to practiceand/or prescriptive authority: AL, AR,CA, FL, GA, IL†, IN, KS, KY, LA, MA, MI,MO, MS, NC, NJ, NY, OH, OK, PA, SC,TN, TX, UT, VA, WIIL: 4,000-hour post-licensure practice period 250 continuing education/training units; Controlled substances Schedule II opioids and benzodiazepine prescribing requires physician consultation† APRNs credentialed in a hospital, hospital affiliate, or ambulatorysurgical treatment center may practice without a written collaborationagreementWV: 3-year post-licensure practice period; Excludes Schedules I, IIcontrolled substances, antineoplastics, radiopharmaceuticals, and generalanesthetics* State may not require post-licensure/certification period of supervision,collaboration, or mentorship when an experienced NP endorsing intothe state has met the regulatory requirement through experience inanother stateConsensus Model adoption. The Legislative Updatehas provided readers with annual progress on implementation of Consensus Model adoption. Accordingto the National Council of State Boards of Nursing,15 states have implemented 100% of the ConsensusThe Nurse Practitioner January 2018 29Copyright 2018 Wolters Kluwer Health, Inc. All rights reserved.
30th Annual APRN Legislative UpdateModel recommendations for APRN licensure, accreditation of APRN programs, certification in respectiveAPRN roles, and educational program requirements.2Although many states have achieved FPA as defined bythe AANP, many states continue to work on legislativeand regulatory amendments to move toward uniformity in these areas.The enactment of Michigan’s Public Act 499 of2016 recognizes the clinical nurse specialists (CNS)as an APRN role and adds a CNS seat to the MichiganBON. Additionally, the act defines APRN in statute, recognizing nurse midwives, NPs, and CNSs asAPRNs. Minnesota amended their law requiringAPRN programs to include separate, graduate-levelcourses in advanced physiology and pathophysiology, advanced health assessment, and pharmacokinetics/pharmacodynamics of all broad categoriesof agents in alignment with the Consensus Modelrecommendations.North Dakota adopted the APRN Compact forlicensure in 2017, joining Wyoming and Idaho as thethird APRN licensure compact state in the UnitedStates. The purpose of the APRN Compact is to provide opportunities for interstate practice by APRNswho meet uniform licensure requirements, facilitationof information exchange between compact states inareas of APRN regulation, investigation, and adverseactions, among other things.3 Oklahoma updatedstatutes to reflect the recommended title “APRN” fromadvanced practice nurse (APN) throughout the NursePractice Act.Ordering home health services. This year, surveyrespondents were asked to respond to a question regarding state statutory authority to order home healthservices. If the home health agency is Medicare- and/or Medicaid-certified, 42 Code of Federal Regulation 484.18 (c) requires a physician signature to orderhome health services. However, some states authorizehome health agencies to accept orders from APRNswhen patients are private-paying or non-Medicare/non-Medicaid recipients under state law. While manystates did not respond to the question, there is initialState response to statutory/regulatory authorityState statutory authorityCA, FL, OR, WYStatutory authority not prohibitedCO, NHNo statutory authorityKS, RI, SD, VA, WVinformation on statutory authority (see State responseto statutory/regulatory authority).Advances in protocol/collaborative agreement requirements and SOP. Florida successfully removed therequirement to file ARNP protocols with the BON. Effective June 23, 2017, ARNP protocols must be maintained onsite at the practice location. The supervisorynature of practice in Florida was not changed duringthis legislative session. Oregon amended ORS 435.305,which previously prohibited performance of a sterilization procedure by an NP. NPs are now authorized toperform a vasectomy, specifically citing the procedureis within the NP’s SOP.Professional corporations. Oregon amended current law, authorizing co-ownership of medical clinicsby NPs, physicians, and physician assistants (PAs).Specifically, the corporations’ codes were amended toclarify that the majority of directors and shareholdersof a medical corporation can be physicians, NPs, orPAs. The law specifically prohibits a physician, NP, orPA from directing the services of another practitioner in the professional corporation unless the otherpractitioner also practices within the same SOP. Additionally, individuals employed in the professionalcorporation or individuals who own interest in thecorporation may not direct medical judgment of thephysician, NP, or PA. This law will go into effect January 1, 2018. ReimbursementAmendments to statutes or regulations pertaining toAPRN reimbursement historically have been lacking. In 2017, only one state reported the passage oflegislation impacting APRN reimbursement. On June7, 2017, Vermont enacted Act 64 relating to insurance coverage for telemedicine services delivered inor outside a healthcare facility. Specifically, Act 64requires commercial health plans and Medicaid tocover telemedicine services regardless of where thepatient receives those services. The act uses the provider-neutral term “healthcare provider,” inclusive ofAPRNs as providers for whom the plan must providereimbursement. Prescriptive authorityControlled substances regulation. In July 2017, Alaskaenacted Chapter 2 SSLA 17, mandating PDMP registration by all DEA registered prescribers licensed inthe state of Alaska. Practitioners must review PDMP30 The Nurse Practitioner Vol. 43, No. 1Copyright 2018 Wolters Kluwer Health, Inc. All rights reserved.www.tnpj.com
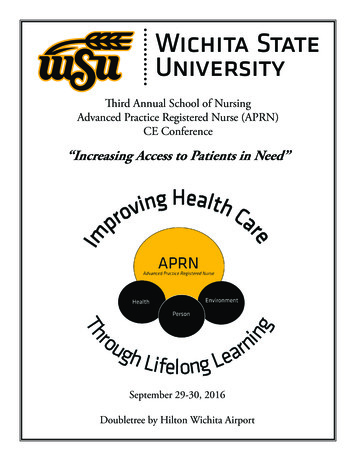
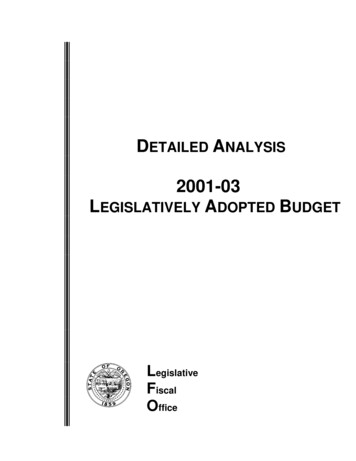
30th Annual APRN Legislative UpdateTotal Number of Licensed/Certified APRNs Reported by BONs and/or State Nursing Associations in 2017StateAlabamaAlaskaArizonaArkansas CaliforniaColoradoConnecticut Delaware District of ColumbiaFloridaGeorgiaHawaii IdahoIllinoisIndiana ttsMichigan MinnesotaMississippi MissouriMontanaNebraska Nevada New Hampshire New JerseyNew MexicoNew YorkNorth CarolinaNorth DakotaOhioOklahomaOregonPennsylvania Rhode IslandSouth Carolina South DakotaTennesseeTexasUtah Vermont VirginiaWashingtonWest VirginiaWisconsin WyomingTotals*††!@# 630*5,5561,899 ,034*765421761608111541 CNS; 809 PCNS!531Not 61,3222,04239@437††3930 8329331275945*105! 9 183713647!2311,3524582,5494,56527369*1,438761 13746,944§Total ,4932,7493,875 724354,062Combined with total number of APNs/APRNs for that state; these states may not break out NP, CNS, CNM,or CRNA numbers individuallyRecognized as APRNs but counted separately from other APRN rolesNot recognized as an APN/APRN/ARNP by the BON and not included in total APRNsPsychiatric clinical nurse specialists recognized as APRNs onlyLicensed/certified as NPs by the BONCertified as APNPs (Advanced Practice Nurse Prescribers)No update to APRN license/certification number was provided by BON.Total of the states that breakout NP, CNS, CNM, or CRNA numbers individuallywww.tnpj.comThe Nurse Practitioner January 2018 31Copyright 2018 Wolters Kluwer Health, Inc. All rights reserved.
30th Annual APRN Legislative Updateinformation prior to prescribing or administering aSchedule II or III controlled substance with certainexceptions, including those receiving treatment in aninpatient setting; at the scene of an emergency; in anED; immediately before, during, or within 48 hoursafter surgery or medical procedure; in a hospice orlong-term-care facility that has an in-house pharmacy;or when a nonrefillable prescription of a controlledsubstance in a quantity for no longer than 3 days. Ad-ambulatory settings by NPs and PAs. NPs and PAsseeking this authority must complete a required 24hour training course related to medication-assistedtreatment of substance abuse disorder prior to applying to the DEA for a waiver. This year, Californiapassed legislation codifying federal authority, eliminating confusion of authority with the DEA whenan NP applies for a buprenorphine waiver. This lawwill go into effect January 1, 2018. Oregon reportedNPs are authorized to prescribe buprenorphine under federal law.Vermont enacted Act 64 relating to insuranceMiscellaneous updates to existing prescriptive authority statutes. Ascoverage for telemedicine services delivered instate APRN and nursing organizaor outside a healthcare facility.tions and BONs work toward FPA,incremental advances provide theditionally, APRNs are required to complete at least 2 opportunity to improve access over time. Tennesseehours of continuing education in opioid prescribing made substantive change in terminology surrounding the professional relationship between physicianseach license renewal period.Kentucky, Louisiana, and North Carolina have and APRNs for prescriptive services, amending codeadopted statutes limiting the quantity of initial and/ sections utilizing “supervision” to “collaboration.”or refill prescriptions of opioid controlled substances. Designated responsibilities and relationships betweenReacting to the nation’s opioid misuse crisis, states are physicians and APRNs were not altered through thisincreasingly regulating all prescribers with respect to legislation; however, changes such as this inform theopioid medications with reasonable exception. The public about the nature of the relationship betweenpublication of the CDC’s Guideline for Prescribing APRNs and physicians in individual states.The author would like to thank the state BONOpioids for Chronic Pain in 2016 has provided lawmakers with evidence needed to positively impact the representatives and APRN association representativeswho contributed to this update via submission of theuse of opioids for pain conditions.4Kentucky amended KRS 218A.205, establishing annual survey. All efforts are made to ensure the inmandatory prescribing and dispensing standards re- formation provided to readers is accurate and up-tolated to controlled substances in Schedules II and III date through validation of adopted regulations andfor the purpose of treating acute and chronic pain enacted legislation.in accord with the CDC’s guidelines.4 Louisiana approved Act 82 in August 2017, limiting the number ofREFERENCESdays opioids can be prescribed with some exceptions. 1. American Association of Nurse Practitioners [AANP]. State practice environment. 2017. legislation/North Carolina adopted the Strengthen Opioid Misstate-practice-environment.use Prevention (STOP) Act, CH. SL 2017.74, applying 2. National Council of State Boards of Nursing [NCSBN]. Implementationstatus map. 2017. rprovisions for screening and prescribing of targetedence-Info/sessionaltcd/1408.controlled substances, including limits on the length 3. National Council of State Boards of Nursing [NCSBN]. The APRN compact:a summary of the key provisions. 2015. https://www.ncsbn.org/Key Proviof initial and refill prescriptions of opioid medicasions of New APRN Compact.pdf.tions for acute pain with some exceptions. The statute 4. Centers for Disease Control and Prevention [CDC]. CDC guideline forrequires NPs to consult with a supervising physicianprescribing opioids for chronic pain. 2016. m.prior to prescribing a targeted controlled substanceunder certain conditions.Susanne J. Phillips is a clinical professor and practicing family nurse practitioComprehensive Addiction and Recovery Act (CARA). ner at the University of California, Irvine.Signed into federal law in July 2016, CARA expanded The author has disclosed that she has no financial relationships related to thisaccess to substance use treatment services by extend- article.ing the privilege of prescribing buprenorphine in DOI:10.1097/01.NPR.0000527569.36428.ed32 The Nurse Practitioner Vol. 43, No. 1Copyright 2018 Wolters Kluwer Health, Inc. All rights reserved.www.tnpj.com
30th Annual APRN Legislative ama.govwww.campaignforaction.org/state/alabama Legal authorityAPRNs are defined as APNs in Alabama andinclude CNP (CRNP in statute), CNS, CNM,and CRNA roles. Although the BON has soleauthority to establish the qualifications andcertification requirements of APNs throughR&Rs, the BON and BOME regulate thecollaborative practice of physicians withCRNPs and CNMs, requiring them to practicewith BON- and BOME-collaborative practiceagreements. The collaborating physician andCRNP or CNM must sign written protocols.The term collaboration does not requiredirect, on-site supervision by the collaborating physician. The term does, however,require such professional oversight anddirection as may be required by the R&R ofthe BON and BOME.The CRNP or CNM and collaboratingphysician shall be present in any approvedpractice site a minimum of 10% of the CRNP/CNM’s scheduled hours if the CRNP or CNMhas less than 2 years of collaborativepractice experience. Remote practice site isdefined in rule, and the collaboratingphysician must visit each remote site atleast quarterly. CRNP SOP is defined instatute and regulation; APNs practice inaccordance with national standards andfunctions identified by the appropriatespecialty-certifying agency in congruencewith Alabama law.Alabama does not recognize APNs asPCPs and does not have “any willingprovider” language in statute. CRNPs arerequired to hold an MSN degree and nationalcertification upon entry into practice with afew exceptions: Initial CRNP applicants areexempt from requirement for MSN at thediscretion of the BON if graduation wasbefore 1996 in a post-BSN NP program orgraduation before 1984 from a non-BSNprogram preparing NPs.CRNAs must, at minimum, hold amaster’s degree from an accredited nurseanesthesia graduate program and becurrently certified as a CRNA; CRNAs whograduated before December 31, 2003, areexempt from the master’s degree requirement. CNS approval requires a master’sdegree or higher in advanced practicenursing as a CNS and national certification. ReimbursementThere are no legislative restrictions for APNson managed-care panels. The AlabamaMedicaid Program enrolls and reimbursesCRNPs independently pursuant to supervisionrules; however, a CRNP who is employed andreimbursed by a facility that receivesreimbursement from the Alabama Medicaidprogram for services provided by the CRNPmay not enroll. BC/BS will reimburse CRNPsand CNMs in collaboration with a preferredphysician provider at 70% of the physician rate.A BON and BOME joint committeerecommends R&R governing the collaborative relationship between physicians,CRNPs, CNMs, and the prescription oflegend drugs that may be prescribed byauthorized CRNPs and CNMs. Authorizationis tied to the collaborative agreement; ifCRNPs or CNMs change physicians, theymust reapply. Prescription pads mustinclude the physician’s name and address,the CRNP’s or CNM’s name, RN licensenumber, and prescription number. The CRNPor CNM who is in collaborative practice andhas prescription privileges may sign for anddispense approved formulary drugs. CNSsand CRNAs are not regulated by the jointcommittee (BON and BOME) and are noteligible for Rx laska Legal authority Prescriptive authorityCRNPs and CNMs may prescribe, administer,and provide therapeutic tests and drugswithin a BON- and BOME-approvedformulary. CRNPs and CNMs in collaborativepractice with a physician may prescribecontrolled substances in Schedules III, IV,and V pursuant to the rules of the AlabamaBOME Chapter 540-X-18. CRNPs and CNMsare required to complete 12 continuingmedical education contact hours inadvanced pharmacology and prescribingtrends and 4 additional contact hours every 2years for renewal of the Qualified AlabamaControlled Substances Certificate undercurrent regulation for Schedule III-Vcontrolled substance authority.APRNs are regulated by the Alaska BON,defined in statute, and include CNP, CNS,CNM, and CRNA roles. APRNs are furtherdefined as RNs who, due to specializededucation and experience, are certified toperform acts of medical diagnosis andprescription as well as dispense medical,therapeutic, or corrective measures underregulations adopted by the BON.Regulations require that an APRNmust have a plan for patient consultationand referral, but a physician relationshipis not required. SOP for APRNs is notdirectly defined in statute or regulation;however, regulation refers to the nationalcertifying body for definition of SOP inspecialty areas.Legislative update PUSAdvanced Nurse PractitionerAdvanced Practice NurseAdvanced Practice Nurse PrescribersAdvanced Practice Registered NurseAdvanced Registered Nurse PractitionerAmbulatory Surgical Treatment CenterBlue Cross/Blue ShieldBoard of MedicineBoard of Medical ExaminersBoard of NursingBoard of PharmacyBoard of Registered NursingCivilian Health and MedicalProgram of the Uniformed WFNPFPAGNPHMOMCOsCertified Nurse MidwifeCertified Nurse PractitionerClinical Nurse SpecialistCollaborative Practice AgreementCertified Pediatric Nurse PractitionerCertified Registered Nurse AnesthetistCertified Registered Nurse PractitionerDrug Enforcement AdministrationDoctor of Osteopathic MedicineDepartment of Public WelfareFamily Nurse PractitionerFull Practice AuthorityGeriatric Nurse PractitionerHealth Maintenance OrganizationManaged-care xSOPWHNPNurse AnesthetistNational Council of State Boards of NursingNurse MidwifeNurse Practice ActPhysician AssistantPrimary Care ProviderPsychiatric Clinical Nurse SpecialistPsychiatric Mental HealthPediatric Nurse PractitionerPreferred Provider OrganizationRegistered Nurse PractitionerRules and RegulationsPrescriptive/PrescribeScope of PracticeWomen’s Health Nurse PractitionerThe Nurse Practitioner January 2018 33Copyright 2018 Wolters Kluwer Health, Inc. All rights reserved.
30th Annual APRN Legislative UpdateAPRNs in Alaska are statutorilyrecognized as PCPs. Nothing in the lawprecludes admitting privileges for APRNs.Entry into APRN practice requires a graduatedegree in nursing and national boardcertification. CE requirements for APRNs are30 CE units; 12 of these must be advancedpharmacotherapeutics as well as 12 hours ofCE in clinical management of patients every 2years. CRNAs practice under separate BONrules and regulations from the CNP, CNS, andCNM; however, incorporation of all APRNregulations is in process.All healthcare in Alaska is provided on afee-for-service basis, and managed caredoes not exist. FNPs, PNPs, and CNMs areauthorized by law to receive Medicaidreimbursement; NPs receive 85% of thephysician payment. A nondiscriminatoryclause in the insurance law allows forthird-party reimbursement to NPs; Alaskalegally requires insurance companies tocredential, empanel, and/or recognizeAPRNs. Alaska does not have “any willingprovider” language in current law.condition occurs that is beyond theknowledge and experience of thenurse or if the referral will protect thehealth and welfare of the patient.No formal collaboration agreement isrequired. RNP SOP is defined in the ArizonaAdministrative Code R4-19-508. In the SOP,RNPs are authorized to admit patients tohealthcare facilities, manage the care ofpatients admitted, and discharge patients.However, Arizona Department of Healthregulations require that patients admitted toan acute care facility must have an attendingphysician. Acute care facilities apply thiscitation as the basis to deny independentadmitting and hospital privileges to RNPs.RNPs, CNMs, and CNSs must have a graduatedegree in nursing and national boardcertification in their focus area to enter intopractice. CRNAs must have a graduate degreeassociated with an accredited CRNA programand hold national certification to enter intopractice. For CRNA SOP, it was clarified that aphysician or surgeon is not liable for any actor omission of a CRNA who orders oradministers anesthetics. CRNAs, therefore,are responsible for their own practice. Prescriptive authority ReimbursementAuthorized APRNs have independent Rxauthority—including Schedules II-Vcontrolled substances—and may apply forDEA registration. APRNs are legally requiredto review the Prescription Drug MonitoringProgram database prior to prescribingcontrolled substances. They are legallyauthorized to request, receive, and dispensepharmaceutical samples in Alaska.Prescriptions are labeled with the APRN’sname only. To renew Rx authority, APRNsmust complete 12 contact hours of continuingeducation (CE) in advanced pharmacotherapeutics, including 2 CE hours in opioidprescribing each 2-year renewal cycle.RNPs and other APRNs may receivethird-party reimbursement, enabled by theDepartment of Insurance statutes. RNPreimbursement varies depending on thehealth insurance plan. na Legal authorityThe Arizona State Legislature grants APRNsauthority, and the BON alone regulates theirpractice. APRNs include RNPs, CNSs, CNMs,and CRNA roles. According to ArizonaRevised Statutes Title 32, Chapter 15 32-1601;20 (vi), the following language was added toboth the RNP and the C
30 The Nurse Practitioner † Vol. 43, No. 1 www.tnpj.com Model recommendations for APRN licensure, accredi-tation of APRN programs, certifi cation in respective APRN roles, and educational program requirements. 2 Although many states have achieved FPA as defi ned by the AANP, many states continue to work on legislative