Transcription
2013 Annual ReportPartners forhealth,inspiringho p e and well-being
Bob Dunbar , Executive DirectorWith so many unfortunate and violent events making headlines, the introduction of mental health parity, andthe on-going debates around Healthcare Reform, behavioral health prevention and intervention systems ofcare have been the subject of increased attention over the past year. In 1982, Adult and Child Center wascreated to support the mental health needs of our community and we continue to lead this charge todaythrough community partnerships, innovative programming, and patient-centered care.Beyond our core belief that Adult and Child staff are consumer partners in treatment, we believe in buildingstrong relationships with community partners who enable us to holistically treat each child, adult, and familywho need our support. A great example of these partnerships include our work with both WindRose HealthNetwork and Community Health Network, which have enabled us to advance our primary care and behavioral health careintegration services in multiple medical settings; thus expanding and improving access to behavioral health services in ourcommunity.Adult and Child Center is dedicated to providing a community-based response to the behavioral and primary care needs of ourcommunity. As those needs change, we are prepared to continually adapt and lead the industry in the provision of an evidencebased response through prevention, early identification, and intervention services.70%1 in 4 Adults experiencemental illness in any given year.Serious Mental Illnesscosts America 193,000,000,000of youth in juvenile justice systemshave at least one mental healthcondition and at least 20 percent livewith a severe mental illnessin lost earnings each year.1
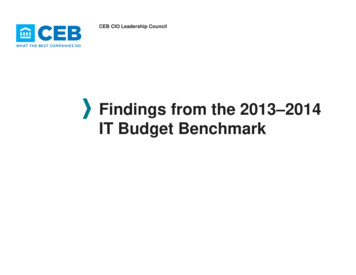
Sue Collins, Board PresidentAs our nation continues to focus on the delivery of affordable and high-quality health care, many health careproviders are left trying to predict the future and navigate their practice toward an ever-changing destination.Among behavioral health providers, which is a specialty practice historically not aligned with major health carenetworks, the future is very exciting. Adult and Child Center had been navigating toward integrated primary andbehavioral health care for nearly a decade through our partnership with WindRose Health Network and, morerecently, with Community Health Network.As our government continues to debate over the details of the Affordable Care Act, we believe a common threadwill appear and we are very excited about it. The Parity Act required insurance plans to reimburse for mental healthservices in a fashion similar to that of primary care, which was a historical step in recognizing the importance of mental health servicesin holistic health. Recent trends in health care reimbursement programs appear to encourage health care networks to “better manage”the holistic health care needs of specific populations through the use of medical homes, shared savings plans, and Accountable CareOrganizations.As the transformation of health care continues, we believe behavioral health providers will play a significant role in working withprimary care providers to effectively care for those with mental and physical illness, encourage holistic health, and decrease the earlymortality rate experienced by people with serious mental illness.Most Common Diagnosis TypeCenter-WideConsumer Contact 0.0060,000.0040,000.0020,000.000.0011%Other -201390,732.73155,567.4213%8%4% 3%7%Adult Consumer Employment Status35%Mood disorderV Codes and Other44%ETOH/Drug AbuseSchizophrenia/Psychotic20%Deferred DxMental Retardation2Unemployed, LookingUnemployed, Not in WorkforceFT EmployedPT Employed
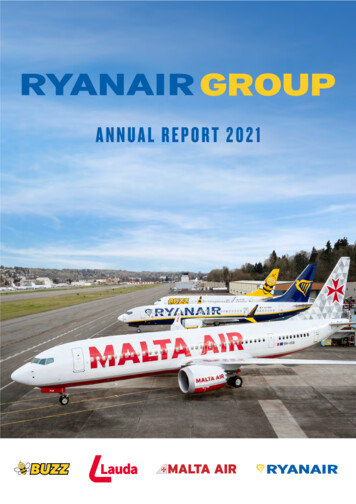
Stephanie Beasley Yoder, New Director of Child and Adolescent ServicesIn March 2013, Stephanie Beasley Yoder came to Adult and Child Center to lead our Child andAdolescent Service Line. Mrs. Yoder earned an MSW from IU and began her child welfare career as aFamily Case Manager (FCM) with the Indiana Department of Child Services (DCS). She was quicklypromoted to a Child Welfare Policy Consultant position at the Indiana DCS where she provided bestpractice consultation, provided guidance on administrative processes in local DCS offices, and trainedregional staff on legislative changes. Mrs. Yoder later served as Policy and Program Manager, DeputyDirector of the Marion County DCS Office, and Deputy Director of Field Operations for DCS.“The Child and Adolescent service line has the honor to serve some of Indiana’s most vulnerablefamilies and children. Our team provides vital supports to children and families through intensive services in the home,community and school. As our service line grows our attention is on ensuring that gaps in services for youth areaddressed. All too often children and youth have complex needs that far exceed the abilities of any one communitypartner to meet. Adult and Child continues to partner to ensure that the diverse needs of children and families can bemet. Partnerships with schools, DCS, probation, courts, primary health care networks, and other youth-servingorganizations are opening more opportunities for children and families to be supported in their recovery in their ownhomes and communities.”Most Common Diagnosis TypeChildren Only# Served Aged 0-17300025004%20004%2% 1%Other MIV Codes and Other12%150056%21%100002004Deferred DxETOH/Drug 1235%4%Medicaid Rehab Option3%Medicaid38%12%Mood disorderMental Retardation500Child Services Funding Sources38%Department ChildrenServicesSchool ContractsTFC/TLP Residential PerDiemCommercial
Our 2012-2013 Board of Directorsfor excellenceMark LoydCarole McKinneyDawn ShimpJoseph SmedleyPam ThompsonKevin TyraJoe VillanuevaSTRIVESue CollinsSteve WohlfordMike KolendaNick HopkinsJane BlessingJames CarterJerry FrenchTom GauntNumber of A&C Consumers ServedConsumer AgeFY 2012FY2013Age 1-172,8173,229Age 18-641,9732,344Age 65 nceawardwinnersKyla Romans Susan PetersonKim GattenGina HensonMary FisherBeth SmithLiz StirnFred PrivetteJane Wiles4Misty ParksEmployee of the yearKathy Rinks
Child and Adolescent ServicesFoster CareWhen children are removed from thecare of their parents andtemporarily placed in a foster home,nurturing foster families are a criticalalternative to residential care settings.These foster families are trained andsupported by Adult&child staff toprovide a safe and caring temporaryhome while biological parents worktoward reunification with their children.Adult and Child Center encouragesdiversity when licensing foster familesand can typically fully license amotivated home in 3-6 months.School BasedEarly identification, prevention, andintervention are critical whendealing with behavioral health concernsin children. Adult and Child Center iscurrently working alongside teachers inover 100 area schools to ensure rapidaccess to behavioral health servicesfor children and their families. Theseprofessionals are specifically trained tosupport children in an educationalsetting, they are respectful ofconfidentiality issues, and they often“bridge the gap” between the student,their family, and the educational system.5TransitionalLivingFor young adults who have lived infoster care or residential homes, thetransition into adulthood can be verychallenging. In fact, an estimated 30%of the nation’s homeless are formerfoster children. A significant percentageof foster kids remain in the foster carenetwork as they reach the age ofindependence (18-24). This programsupports the unique needs of thisage group as they make difficult life,relationship, and vocational decisionswhich often determine “success” intoadulthood.
ResidentialSupportWe are known for our strong clinicalexpertise, our use of evidence-basedpractices, and our strength indelivering trauma-informed care. Wehave developed partnerships withresidential care providers in which ourhighly trained clinicians work sideby side with residential technicians tooptimize the treatment environment foryouth who experience behavioral healthchallenges. This partnership alsoexpands the continuity of care availablefor youth and families once the child ishealthy enough to return home.Home BasedTypically utilized by families involvedin child welfare services, this programprovides supports intended to bothpreserve an “at risk” family and reunitea separated family. Providers typicallymeet with families in their homes andeach family is “wrapped” with a fullarray of supports based upon theirunique strengths, needs, and goals.Adult and Child providers work withfamilies to achieve their goals and oftenprovide a direct line of communicationand advocacy between the Departmentof Child Services and the family.6ChildIntermediatePart of building a strong behavioralhealth program is developing a fullcontinuum of care which fits the everchanging needs of each patient. ChildIntermediate services provide a moretypical outpatient-like service designedto both prevent a more intensiveplacement and provide a step downfrom more intensive services. Theseservices are provided in an office settingand are often brief in scope andduration.
Adult ServicesHeartfeltHealth AllianceIn partnership with WindRose HealthNetwork, this team of behavioral andphysical health care providers integratethe delivery of person-centeredholistic health care. Nationally, adultswith mental illness die 25 years youngerthan the general population and thisprogram is designed to help people whoexperience co-occurring mental illnessand chronic diseases like Diabetes,Asthma, COPD, or Hypertension livelonger, and healthier, lives. This projectis currently supported by SAMHSA.H.O.P.E.HOPE is a relatively new program atAdult and Child Center and is builtupon the idea that, with education andsupport, consumers know how to bestmanage their illness. Through acombination of Illness Management andRecovery (IMR), WellnessRecovery and Action Planning(WRAP), and chronic diseasemanagement, adult consumers learnabout their illness, gain confidence inmanaging their symptoms, and workwith their peers to experience the joy ofrecovery.7TransitionalLivingThis exciting program providessupport for adults who experiencemental illness and are able to live andwork in the community with minimalsupport. Consumers typically live witha few peer roommates and have regularcontact with staff, but live mostlyunsupervised in their homes. As theybegin to experience success in theirlives, they are able to reduce oreliminate the frequency of staff supportwhile remaining in their home with theirestablished support network in place.
CommunityTreatmentBased upon an adapted AssertiveCommunity Treatment model, theseteams provide community-basedsupport to adults with serious mentalillness. The teams are uniquely trainedto deliver evidence-based practiceswhich have been proven effective inhelping this population experiencerecovery from mental health andsubstance use disorders. These staffwork collaboratively with homeless andemergency shelters, physicians, healthcare networks, job training programs,and other community resources.Critical TimeInterventionFunded by a PATH grant, and inpartnership with Wheeler Mission, thisevidence-based practice engagesindividuals who show signs of mentalillness and who currently experiencehomelessness. The program staff areembedded in the operations of WheelerMissions and actively work to identifyand engage symptomatic individuals inservices. Once engaged, the CTI teamwill spend 6-9 months working withthe individual to access health care,stabilize medications, secure housing,and seek employment.8JobLinksA supported employment and Ticket toWork provider, JobLinks works withunemployed individuals to identifyand achieve their personal employmentgoals. Specializing in serving peoplewith a variety of disabilities, JobLinksstaff have developed a uniqueapproach to employment and a networkof employers who look to JobLinks forstrong employees. Services ofteninclude job training, placementassistance, job coaching, soft skillsdevelopment, and post-placementsupport.
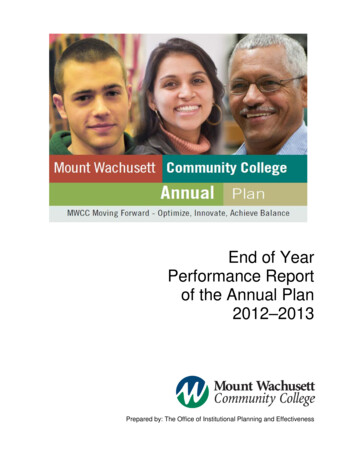
Demographics and OutcomesConsumers by RaceHispanic3.93%350Af. American24.30%250White68.26%Consumer GrowthAge of A&C 00810 15 20 25 30 35 40 45 50 55 60 65 70 75 80 8520092010Age 0-17Centerwide Disability Types201120122013Age 18 A&C Consumer Gender281725%34%Adult FemaleAdult Male1262118818%23%577Child st Common Diagnosis TypeCenter-WideAgency Service Delivery StatsFY 2012-20135,699 Unique consumers342,182 Encounters256,609 Client hours4% 3%11%7%Other MI42%13%Mood disorderV Codes and OtherETOH/Drug AbuseSchizophrenia/Psychotic20%Deferred DxMental Retardation9Consumer Contact 0.0060,000.0040,000.0020,000.000.00Child 01390,732.73155,567.42
Agency FinancialsRevenuesA&C’s Revenue and Expense BreakdownIncome From Services, 65.2%Salaries, Benefits, & Taxes, 73.5%PublicSupport, 30.5%ClientRelated,8.25%Other4.3% 17,109,123Public Support Revenue 8,059,283Other Operating RevenueTotal RevenuesSalaries and BenefitsA&C’s Administration rate compared to otherIndiana Community Mental Health Centers25th Percentile75th PercentileMedianAverage 1,212,373 26,380,779Other18.25%ExpensesA&C AdministrationAmountNet Revenue from Services & Per DiemAmount 20,987,979Client Related Expenses 2,356,191Other Expenses 5,222,566Total Expenses 28,566,73613.0%17.5%Net Income from Operations23.0%Net Income from Non Operations19.4%Net Income for mission20.8%10( 2,185,957) 783,684( 1,402,273)
222 East Ohio Street, Indianapolis603 E Washington Street, Indianapolis8320 Madison Avenue, Indianapolis8404 Siear Terrace, Indianapolis86 Drake Road, Franklin877-882-5122AdultandChild.org
Adolescent Service Line. Mrs. Yoder earned an MSW from IU and began her child welfare career as a Family Case Manager (FCM) with the Indiana Department of Child Services (DCS). She was quickly promoted to a Child Welfare Policy Consultant position at the Indiana DCS where she provided best