Transcription
93Group Cognitive-Behavioral Therapy for Auditory Hallucinations: A Pilot StudyA m y E. P i n k h a m , A n d r e w T. Gloege, Steven Flanagan, a n d David L. P e n n ,University o f North Carolina at Chapel H i l lIn this article, we describe a pilot study that investigated the effectiveness of group cognitive behavioral therapy (CBT) for auditoryhallucinations. Eleven inpatients with either chronic schizophrenia or schizoaffective disorder participated in 2 CBT groups of differing treatment duration (i.e., 7 versus 20 sessions). The results showed that participation in both groups was associated with significant positive changes in the participants' beliefs about their voices and with a trend for reduced negative reactions to the voices. Thesechanges were not a function of premorbid cognitive functioning. Finally, duration of treatment did not affect participants' beliefs ordistress associated with the voices. Implications for future clinical research in this area are discussed.UDITORY HALLUCINATIONSoccur frequently amongindividuals who have been diagnosed with schizophrenia and are a defining feature of the disorder. In fact,16 studies, reviewed by Slade and Bentall (1988), indicatethat, on average, 60% of individuals who are diagnosedwith schizophrenia experience auditory hallucinations.These hallucinations vary widely in the number of voices anindividual hears, the physical characteristics of the voices,and the content of what the voices say; however, individualswho hear hallucinations often describe the experience asdistressing, which is consistent with evidence that abusivelanguage is the most common form of auditory hallucination (Nyani & David, 1996). Additionally, some researcherspostulate that auditory hallucinations may contribute toand maintain depression and low self-esteem in individualswith schizophrenia (Wykes, Parr, & Landau, 1999).The first line of treatment for auditory hallucinationsis andpsychotic medication; however, estimates indicatethat as many as 25% to 50% of individuals with schizophrenia experience residual positive symptoms of psychosis, despite proper levels of medication (Kane &Marder, 1993; Pantelis & Barnes, 1996; WiersIna, Nienhuis, & Sloof, 1998). Given the periodic medication resistance of auditory hallucinations, several psychological interventions have been explored. These interventionshave employed thought stopping, exposure with anxietyreduction, self-monitoring, and distraction techniquessuch as listening to music, subvocal counting, or wearingearplugs (see Haddock et al., 1998; Shergill, Murray, &McGuire, 1998, for reviews). Recently, several new approaches have been adapted from cognitive behaviorCognitive and Behavioral Practice 11, 9 3 - 9 8 , 2 0 0 4107%7229/04/93 -9851.00/0Copyright 2004 by Association for Advancement of BehaviorTherapy. All rights of reproduction in any form reserved.[ Continuing Education Quiz located on p. 131.therapy (CBT) that appear to be beneficial. Controlledtrials of individual CBT for psychosis indicate that this approach has been successful in reducing overall symptoms(see Bustillo, Lauriello, Horan, & Keith, 2001; Gould,Mueser, Bolton, Mays, & Goff, 2001; Norman & Townsend, 1999, for reviews). Further, randomized controlledtrials of individual CBT have demonstrated that individualswho receive CBT are more likely to maintain improvement during follow-up than individuals who receiveother forms of treatment. Sensky et al. (2000) comparedindividual CBT to a nonspecific befriending interventionand found that at the end of treatment, both interventions led to significant clinical improvements in whichboth positive and negative symptoms were reduced; however, only the CBT group maintained these gains at a 9month follow-up (see Tarrier et al., 1999, 2000, for exceptions). Similarly, a study comparing individual CBT withstandard care demonstrated that for the CBT group, a reduction in the frequency of auditory hallucinations aswell as the intensity of and distress associated with thesehallucinations was evident at a 9-month follow-up (Kuiperset al., 1998). These findings indicate that individual CBTfor residual symptoms is especially effective for reducingauditory hallucinations (Tarrier et al., 2001).The success of individual CBT has prompted researchers to examine more efficient means of administering CBT for residual psychotic symptoms. One such wayis to present the intervention in a group format, and thefew studies that have examined group CBT have reportedpositive findings. Gledhill, Lobban, and Sellwood (1998)found that a group CBT intervention was associated withparticipants being better able to cope with symptoms,and having lower depression, higher self-esteem, andgreater knowledge about schizophrenia. Wykes et al.(1999) utilized a wait-list control design and reported thatfollowing group CBT, participants reported a reductionin the experience of auditory hallucinations and an
94Pinkham et al.i n c r e a s e d p e r c e p t i o n o f c o n t r o l over the voices. Likewise,six o f n i n e individuals who p a r t i c i p a t e d in a CBT-basedself-control skills g r o u p r e p o r t e d that their voices wereless distressing a n d less distracting at the e n d o f treatm e n t (Perhnan & H u b b a r d , 2000). Finally, Chadwick,S a m b r o o k e , Rasch, a n d Davies (2000) r e p o r t e d that individuals who p a r t i c i p a t e d in their g r o u p CBT for auditoryhallucinations h a d less conviction in beliefs that the voiceswere o m n i p o t e n t a n d that they h a d no control over thevoices following treatment. These results provide encoura g e m e n t that g r o u p CBT may decrease the severity ofpsychotic symptoms, although, at this time, only o n e controlled trial has b e e n c o m p l e t e d (i.e., Wykes et al., 1999).Thus, g r o u p CBT has p r o m i s e for r e d u c i n g the negativeeffects of h e a r i n g voices a n d may aid participants in theirefforts to cope with auditory hallucinations.T h e above g r o u p CBT studies for auditory hallucinations were c o n d u c t e d either with groups c o m p r i s e dsolely o f outpatients or a c o m b i n a t i o n of o u t p a t i e n t a n di n p a t i e n t participants. Litde is known, therefore, a b o u tw h e t h e r g r o u p CBT is effective for inpatients withc h r o n i c schizophrenia. Since inpatients are likely to havem o r e severe p a t h o l o g y than outpatients, as well as greatert r e a t m e n t refractory symptoms, a trial o f g r o u p treatm e n t with chronically ill inpatients represents a m o r e rigorous test o f the effectiveness o f CBT for hallucinationsthan has h i t h e r t o b e e n c o n d u c t e d .T h e p u r p o s e o f this study was to c o n d u c t an initialevaluation o f g r o u p CBT for auditory hallucinations o nan i n p a t i e n t sample o f individuals with chronic psychoticsymptoms. To o u r knowledge, there are no p u b l i s h e dstudies o n g r o u p CBT for auditory hallucinations a m o n ginpatients. F u r t h e r m o r e , with the e x c e p t i o n of P e r l m a na n d H u b b a r d (2000), which focused on self-control skills,n o n e o f the above g r o u p CBT studies were c o n d u c t e d inthe U n i t e d States. T h e r e f o r e , this study represents an initial a t t e m p t to apply i m p o r t a n t clinical techniques develo p e d in the U n i t e d Kingdom, particularly those thatfocus on r e d u c t i o n of auditory hallucinations, to workwith inpatients in the U n i t e d States. A final p u r p o s e o fthis study was to e x a m i n e w h e t h e r the d u r a t i o n o f g r o u pCBT has an effect on auditory hallucinations. Specifically,we c o m p a r e the original Wykes et al. (1999) protocol,c o m p r i s e d o f 7 sessions, to an e x p a n d e d p r o t o c o l o f 20sessions in which topics were e x p l o r e d in greater depth.D u r a t i o n o f t r e a t m e n t was investigated because o f thepossibility that inpatients with chronic s c h i z o p h r e n i a mayrequire t r e a t m e n t c o n d u c t e d over a greater time p e r i o dthan outpatients in o r d e r for clinical gains to accrue. Itwas hypothesized that (a) a CBT g r o u p intervention forvoices would have a significant effect on participants' beliefs a b o u t their voices, a n d (b) the longer, m o r e ext e n d e d p r o t o c o l would result in greater t r e a t m e n t gainsthan the s h o r t e r t r e a t m e n t protocol.MethodParticipantsIndividuals were r e c r u i t e d via t r e a t m e n t teams thath a d b e e n notified a b o u t the p r o p o s e d study, a n d potentim participants were r e f e r r e d for g r o u p CBT by these individual t r e a t m e n t teams, which i n c l u d e d a psychiatrist,psychologist, social worker, nurse, a n d two h e a l t h technicians. Eligible individuals were those who e x p e r i e n c e dmedication-resistant auditory hallucinations a n d r e p o r t e dthat these experiences were distressing. Medication resistance was d e f i n e d as persistent auditory hallucinationsdespite b e i n g on a stable dose of neuroleptics (i.e., b e i n gon the m e d i c a t i o n for at least 3 m o n t h s ) , a n d all individuals were currently taking atypical antipsychotics. Individuals who d e n i e d h e a r i n g voices a n d those who experie n c e d no distress d u e to their voices were e x c l u d e d f r o mthe sample. Eleven inpatients that m e t DSM-/Vcriteria foreither s c h i z o p h r e n i a (n -- 5) or schizoaffective d i s o r d e r(n 6) p a r t i c i p a t e d in the study. Diagnoses were determ i n e d based on chart review, a n d the sample c o m p r i s e d8 males a n d 3 females, o f w h o m 63.6% were Caucasian.T h e average age o f participants was 39.6 years a n d theyh a d b e e n hospitalized for an average o f 44.6 m o n t h s(minimum -- 3 months, m a x i m u m 228 months, m o d e 20 months) p r i o r to participating in the groups.MeasuresAuditory Hallucinations Rating Scale (PSYRATS, Haddock,McCarron, Tarri & Faragher, 1999). T h e PSYRATS is an11-item, interview-based m e a s u r e that assesses the emotional content, physical characteristics, a n d cognitive int e r p r e t a t i o n o f auditory hallucinations. R e p o r t e d reliability for each item ranges from 1.0 to .788 ( H a d d o c k et al.,1999). In the c u r r e n t study, we administered the PSYRATSas a self-report m e a s u r e (Wykes et al. 1999). C r o n b a c h ' sa l p h a was .56 at the initial assessment a n d .63 at the postintervention assessment, indicating m o d e r a t e i n t e r n a lreliability.1Beliefs About VoicesQuestionnaire-Revised (BAVQ-R; Chadwick, Lees, & Birchwood, 2000). T h e BAVQ is a self-reportmeasure that assesses the individual's beliefs, emotions,a n d behavior a b o u t auditory hallucinations. Sampleitems include statements such as, "My voice is p u n i s h i n gme for s o m e t h i n g I have done" a n d "My voice makes m efeel down," a n d the p a r t i c i p a n t is asked to state to whatd e g r e e they agree with each statement. A l t h o u g h theBAVQ-R has five subscales, only the total score was used inthis study as it is considered to be a m o r e comprehensivet Because no significant differences were found between thegroups, all retiabiliV calculations were computed by combiningGroups 1 and 2. Additionally, in order to achieve acceptable reliabilityfor this study, Item 5 of the PSYRATSwas omitted from the analyses.Omission of this item did not alter any substantive results.
Group CBT for Auditory Hallucinationsr e p r e s e n t a t i o n o f an individual's reaction to auditoryhallucinations. T h e r e p o r t e d m e a n C r o n b a c h ' s a l p h a forthe measure's five subscales was .86, a n d each subscaleh a d a d e q u a t e reliability r a n g i n g between .74 a n d .88.Similarly, the total score reliability for this study was acceptable with C r o n b a c h ' s a l p h a of .85 at p r e t r e a t m e n tassessment a n d .84 at p o s t t r e a t m e n t assessment.Positive and Negative Syndrome Scale (PANSS; Kay, Opler,&Fiszbein, 1992). T h e PANSS is a structured clinical interview d e s i g n e d to assess the severity o f positive a n d negative symptoms. F o r the p u r p o s e s of this study, only thehallucinatory behavior item was used, which consists o f aseries o f questions c o n c e r n i n g the frequency a n d qualityo f a u d i t o r y hallucinations as well as the d e g r e e to whichthey affect thinking a n d behavior. This m e a s u r e has adequate internal reliability (.73 to .83 for each o f the scales)a n d high test-retest reliability (.89 a n d .82 for the positivea n d negative scales, respectively). Raters h a d b e e n previously t r a i n e d to a d e q u a t e reliability (ICC .80 with a criterion rater).WideRangeAchievementTest-III (WRAT3; Wilkinson, 1993).T h e WRA F3 was used to assess the r e a d i n g ability o f eachp a r t i c i p a n t to obtain an estimate of p r e m o r b i d generalintelligence.ProcedureTwo groups were c o n d u c t e d in this study. The firstg r o u p followed the m a n u a l d e v e l o p e d by Wykes et al.(1999; discussed below). T h e second group, c o n d u c t e d 4m o n t h s after c o m p l e t i o n of the first group, followed ane x p a n d e d version o f the Wykes et al. manual. O n e individual who was in the first g r o u p was also r e f e r r e d fora n d i n c l u d e d in the s e c o n d group. F o r m a l a t t e n d a n c erecords were n o t k e p t for e i t h e r group; however, b o t hsets o f g r o u p leaders r e p o r t e d that a t t e n d a n c e was high.T h e PSYRATS a n d BAVQ-R were a d m i n i s t e r e d to eachp a r t i c i p a n t in b o t h groups at the time o f referral a n d atthe e n d o f the group. T h e PANSS was a d d e d to the assessm e n t battery after c o m p l e t i o n o f G r o u p 1 a n d thus wasa d m i n i s t e r e d pre- a n d p o s t i n t e r v e n t i o n for G r o u p 2 only.These measures were a d m i n i s t e r e d e i t h e r by hospitalstaff o r by the g r o u p CBT leadersY T h e WRAT3 wasa d d e d to the battery at the e n d o f G r o u p 2 to address thepost-hoe question o f w h e t h e r cognitive f u n c t i o n i n g couldaffect the participants' ability to benefit from the intervention. Thus, the WRAT3 was a d m i n i s t e r e d postintervention for G r o u p 2. 32Although it could be argued that allowing the assessments to beadministered by the group leaders may have introduced demandcharacteristics that could have influenced the data for Group 2, this isunlikely because many of the measures were self-report and no groupsignificant differences existed between Group 1, in which hospitalstaff conducted the assessments, and Group 2.3Raters were not blind to treatment condition.InterventionG r o u p 1 followed the Wykes et al. m a n u a l a n d m e t forseven 1-hour weekly sessions. Each session a d d r e s s e d aparticular ssion1:2:3:4:5:6:7:sharing o f i n f o r m a t i o n a b o u t the voicesm o d e l s of psychosism o d e l s of h a l l u c i n a t i o neffective c o p i n g strategiesstigma a n d the role o f m e d i c a t i o ni m p r o v i n g self-esteemoverall m o d e l o f c o p i n g with the voicesG r o u p 2 followed an e x p a n d e d version o f the Wykes etal. m a n u a l that was revised by o n e o f us (DLP) to b e t t e rm e e t the clinical n e e d s o f an i n p a t i e n t p o p u l a t i o n . Thisrevised m a n u a l e x t e n d e d the g r o u p to 20 sessions a n dm e t for 1 h o u r twice weekly. O n l y m i n o r alterations werem a d e to the c o n t e n t o f the original manual; the m a i nchanges were that m o r e time was spent on difficult topicsa n d additional h o m e w o r k was assigned. T h e interventionwas as follows:Sessions 1 - 3 : sharing o f e x p e r i e n c e s a n d i n f o r m a t i o na b o u t voices a n d n o r m a l i z a t i o nSession 4: p s y c h o e d u c a t i o n a n d m o d e l s o f psychosisSession 5: tileme a n d c o n t e n t o f e x p e r i e n c e sSessions 6 - 1 0 : behavioral analysis of voices with particular emphasis on the A n t e c e d e n t s - B e l i e f s Consequences (ABC) m o d e lSessions 11-13: establishing c o n t r o l over the voiceswithin the c o n t e x t o f the ABC m o d e l (increasinga n d decreasing strategies)Sessions 14-17: c o p i n g with the voicesSession 18: stigmaSessions 19-20: overall m o d e l o f c o p i n g with voicesand terminationThus, the overall goal o f the intervention is to applycognitive-behavioral techniques to auditory hallucinations.T h e initial sessions focus on b u i l d i n g r a p p o r t a m o n g theg r o u p m e m b e r s a n d the therapists a n d on p o i n t i n g o u tto participants that m a n y o t h e r individuals have experiences similar to their own. Some time is s p e n t t e a c h i n gc u r r e n t theories o f psychosis a n d e x p l a i n i n g c o m m o n l yused treatments. CBT techniques, such as self-monitoringand coping strategies, are at tile heart o f the intervention.Self-monitoring is employed by asking participants to monitor their thoughts and actions prior to, during, a n d afterhearing voices. This allows for the identification o f any patterns that may be present a n d encourages a functional analytic a p p r o a c h to their experiences. After completing theseexercises, individuals begin to utilize coping strategieswhen they h e a r voices and are asked to m o n i t o r the effectiveness of these coping strategies. Over the course of treatment, multiple coping strategies are tried, a n d participants95
96Pinkham et al.Table 1Demographic Information for the Final SampleAgeGenderMalesFemalesQualifying diagnosisSchizophreniaSchizoaffectiveNote.Group 1Group 240.6 (11.67)37.8 (4.66)41414114All diagnoses were derived from chart reviews.are e n c o u r a g e d to c o n t i n u e u s i n g the strategies t h a t allow- t h e m to feel m o r e c o n t r o l o v e r t h e i r voices a n d t h a tr e d u c e the a m o u n t o f distress they e x p e r i e n c e . 4ResuRsAll p a r t i c i p a n t s in e a c h g r o u p successfully c o m p l e t e dt r e a t m e n t , with t h e e x c e p t i o n o f o n e i n d i v i d u a l w h o wasd i s c h a r g e d p r i o r to g r o u p c o m p l e t i o n . This individual'sd a t a w e r e e x c l u d e d f r o m t h e analyses. Additionally, forthe participant who completed both groups, only datac o l l e c t e d f r o m G r o u p 1 w e r e i n c l u d e d in the analysis.These modifications brought the number of participantsin e a c h g r o u p to five. 5 Table 1 s u m m a r i z e s the d e m o g r a p h i c characteristics o f t h e two g r o u p s o f final particip a n t s in t h e study.Preliminary AnalysesP r i o r to a d d r e s s i n g tile hypotheses, we c o n d u c t e d prel i m i n a r y analyses to e x a m i n e w h e t h e r the two g r o u p sd i f f e r e d o n any o f t h e d e m o g r a p h i c o r b a s e l i n e clinicalvariables. C h i - s q u a r e tests r e v e a l e d t h a t t h e g r o u p s d i dn o t significantly differ o n g e n d e r , X2(t, N 10) .000,ns, diagnosis, X2(1, N 10) 3.600, ns, o r ethnicity, X2(1,N 10) .476, ns. Additionally, a M A N O V A was cond u c t e d to e x a m i n e w h e t h e r t h e two g r o u p s d i f f e r e d inage o r l e n g t h o f c u r r e n t hospitalization. T h e M A N O V Awas n o t significant, Wilks's h .791, F(2, 7) .927, ns,thus i n d i c a t i n g t h a t t h e g r o u p s d i d n o t significantly differo n t h e c o m b i n e d variables o f age o r l e n g t h o f hospitalization. A s e c o n d M A N O V A was c o n d u c t e d o n t h e b a s e l i n eclinical variables (i.e., BAVQ-R a n d PSYRATS). T h i s analysis was n o t significant, Wilks's X .846, F(2, 7) .637, ns,4A revised manual is available upon request.5Full regression diagnostics did indicate potential oudiers on eachmeasure; however, given that no one individual was deviant on allmeasures and the extremely small size of this sample, the decision wasmade to leave the data set intact, and results should be interpretedcautiously.Table 2Pre- and Posttreatment Mean Scores on the Clinical Measuresas a Function of CBT GroupGroup 1PretreatmentBAVQ-R 52.6 (22.69)PSYRATS 25.4 (6.31)PANSSN/AGroup 2PosttreatmentPretreatmentPosttreatment40.8 (21.78)21.8 (4.15)N/A61.8 (10.62)27.4 (5.98)5.4 (.89)55.6 (9.66)22.4 (8.56)4.6 (.55)Note. Standard deviadons are in parentheses. BAVQ-R BeliefsAbout Voices Questionnaire-Revised; PSYRATS Auditory Hallucinations Rating Scale; PANSS Positive and Negative Syndrome Scale.i n d i c a t i n g that t h e g r o u p s did n o t differ o n t h e c o m b i n e db a s e l i n e clinical measures.Primary AnalysesTo test the h y p o t h e s i s t h a t t h e l o n g e r p r o t o c o l w o u l dl e a d to g r e a t e r t r e a t m e n t gains t h a n t h e s h o r t e r p r o t o c o l ,we c o n d u c t e d a M A N O V A o n t h e raw c h a n g e scores o nt h e BAVQ-R a n d PSYRATS (see Table 2 for m e a n scoresfor e a c h g r o u p ) . T h e o m n i b u s test r e v e a l e d t h a t g r o u pwas n o t a significant p r e d i c t o r o f the c o m b i n e d o u t c o m em e a s u r e s ; t h e m a g n i t u d e o f t h e c h a n g e b e t w e e n prea n d p o s t t r e a t m e n t d i d n o t differ as a f u n c t i o n o f g r o u p ,Wilks's X .9088, F(2, 7) .35, ns. Additionally, n o sign i f i c a n t u n i v a r i a t e effects w e r e f o u n d ; g r o u p was n o tsignificantly r e l a t e d to c h a n g e o v e r t i m e in e i t h e r t h eBAVQ-R, F(1, 8) .80, ns, o r i n the PSYRATS, F(1, 8) .10,ns. T h u s , c o n t r a r y to o u r hypothesis, t h e l o n g e r p r o t o c o ldid n o t result in g r e a t e r t r e a t m e n t gains t h a n the s h o r t e rprotocol.Given these findings, t h e two g r o u p s w e r e c o m b i n e dto test o u r o t h e r h y p o t h e s i s t h a t g r o u p C B T w o u l d h a v ean effect o n beliefs a n d r e a c t i o n s to a u d i t o r y hallucinations. S i m p l e t tests w e r e c o m p u t e d to d e t e r m i n e if t h ea m o u n t o f c h a n g e s e e n o n e a c h m e a s u r e after t r e a t m e n tsignificantly d i f f e r e d f r o m zero. Results d e m o n s t r a t e dt h a t a significant i m p r o v e m e n t was e v i d e n t b e t w e e n t h epre- a n d p o s t t r e a t m e n t scores o n t h e BAVQ-R, t(9) 2.91, p .05, effect size .51. T h e a m o u n t o f i m p r o v e m e n t b e t w e e n pre- a n d p o s t t r e a t m e n t scores o n t h ePSYRATS a p p r o a c h e d statistical significance, t(9) - 2.07,p .0689, effect size .7213, a n d for t h e individuals inG r o u p 2 only, t h e a m o u n t o f c h a n g e o n t h e PANSS didn o t significantly differ f r o m zero, t(4) 2.14, p .0993,effect size 1.1188).66Significance values were not corrected for alpha inflation due tothe small sample size and the obvious loss of power associated withsuch a correction.
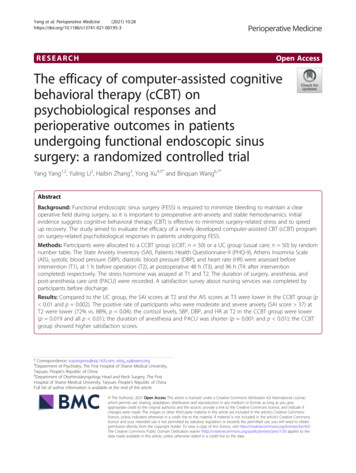
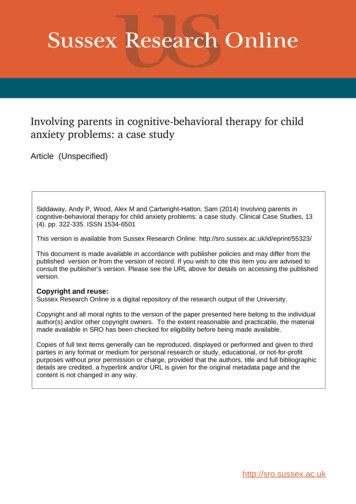
97Group CBT for Auditory HallucinationsTable 3Pre- and Post-treatment Mean Scores on the Clinical t57.2 (17.39)26.5 (5.85)5.4 (.89)48.2 (17.69)22.l (6.35)4.6 (.54)Standarddeviationsare in parentheses,and scores for the PANSSare for Group 2 only. BAVQ-R BeliefsAbout Voices QuestionnaireRevised; PSYRATS AuditoryHallucinationsRating Scale; PANSS Positive and Negative SyndromeScale.Note.lucinations following the first group a n d t h e n experie n c e d a n increase in negative beliefs prior to b e g i n n i n gthe second group. What is most interesting, however, isthe decline in distress associated with his or h e r voicesafter c o m p l e t i o n of the second group. This single casedesign suggests a specific t r e a t m e n t effect a n d indicatesthat individuals may receive greater benefits from repeated exposure to the principles a n d techniques taughtin the group.DiscussionIt is interesting to note that although the results forthe PSYRATS a n d PANSS did n o t reach conventional statistical significance, the m e a n scores for the PSYRATSa n d PANSS did decrease following treatment. Scores o nthe PSYRATS decreased from a m e a n of 26.5 to 22.1 aftertreatment, a n d scores o n the PANSS decreased from anaverage of 5.4 to 4.6, indicating some i m p r o v e m e n t (seeTable 3 for complete pre- a n d posttreatment scores forthe c o m b i n e d groups). Thus, the marginally significantresults, despite large effect sizes for both tests, appear tobe due to the low statistical power of the study ratherthan an absence of a t r e a t m e n t effect (Cohen, 1988).Supplementary AnalysesTo address the post-hoc hypothesis that intellectualf u n c t i o n i n g may influence a participant's ability to benefit from the group, multivariate regression was used to exa m i n e the predictive ability of p r e m o r b i d intellectualability. The o m n i b u s test revealed that r e a d i n g ability wasn o t predictive of the c o m b i n e d clinical o u t c o m e measures, Wilks's X .1174, F(1, 3) 2.51, ns, or for eachmeasure individually (BAVQ-R: F [1, 3] 2.32, ns; PSYRATS: F[1, 3] 1.45, ns; PANSS: F[1, 3] .03, ns). Thus,p r e m o r b i d intellectual f u n c t i o n i n g was n o t related tot r e a t m e n t response in this sample.Finally, recall that o n e individual participated in bothgroups. As a post-hoc analysis, we e x a m i n e d this participant's pre- a n d p o s t t r e a t m e n t BAVQ-R a n d PSYRATSscores for each group (Figure 1). The participant showedi m p r o v e m e n t in his or her beliefs regarding auditory hal7030 a -PS'tRATS100Fte-groupIPost-group1 Pre- roup2 Post-goqo2Figure t. Scores on the clinical measures for the individual whoparticipated in both groups.This study evaluated the effects of a group cognitivebehavioral therapy for inpatients with persistent auditoryhallucinations. The results revealed that distress associated with symptoins was r e d u c e d at the e n d of the treatm e n t a n d that this i m p r o v e m e n t did n o t differ as a function of protocol length. That is, the two t r e a t m e n t groupsthat differed in protocol length both showed significantreductions in multiple d i m e n s i o n s of auditory hallucinations such as distressing beliefs about the voices a n d frequency of auditory hallucinations.Perhaps the most i m p o r t a n t extension of this study toprevious work in this area is that it was c o n d u c t e d onlywith inpatients. Individuals who are hospitalized often experience more severe symptoms than outpatients, a n dthe fact that i m p r o v e m e n t was seen even in this symptomatic a n d chronically ill p o p u l a t i o n suggests that the treatm e n t has good potential. Further, the clinical utility ofthis t r e a t m e n t appears to be quite good. I n other words,this study shows that group CBT is a clinicaUy feasible intervention for auditory hallucinations a n d has promisingdirect clinical benefits. A self-report measure was administered to the participants of the second group at the conclusion of treatment, a n d all participants reported feelings of greater control over their voices, less distressassociated with their voices, a n d greater knowledge a b o u ttheir voices. All of these i m p r o v e m e n t s were attributed toparticipation in the group.It is u n c l e a r what a c c o u n t e d for the lack of t r e a t m e n td u r a t i o n effects. O n e possibility is that the clinical effectsare solnewhat rapid. The f i n d i n g that intellectual funct i o n i n g did n o t limit participants' abilities to benefit fromthe group indirectly supports this hypothesis, as onem i g h t expect persons with cognitive i m p a i r m e n t s to benefit from greater frequency of treatment. Therefore, theeffectiveness of the briefer group CBT suggests that thisi n t e r v e n t i o n may be a cost- a n d t/me-efficient m e t h o d fordelivering psychosocial treatments.T h e r e are a few limitations to this study, such as thelack of a control group, r a n d o m assignment to groups,follow-up assessments, a n d b l i n d i n g of raters. Althoughlack of a control group may appear to be the most important limitation, it should be n o t e d that almost all of the
98P i n k h a m e t al.participants were long-term, chronic patients who showedlittle to n o i m p r o v e m e n t i n t h e i r a u d i t o r y h a l l u c i n a t i o n so v e r t h e c o u r s e o f t h e i r stay a t t h e h o s p i t a l . T h u s , it islikely t h a t t h e i m p r o v e m e n t s s e e n h e r e c a n b e a t t r i b u t e dt o t h e i n t e r v e n t i o n r a t h e r t h a n t r e a t m e n t as usual. 7 However, g i v e n t h e o t h e r l i m i t a t i o n s m e n t i o n e d a b o v e , t h e s eresults should be interpreted with caution, and addit i o n a l trials s h o u l d b e c o n d u c t e d to r u l e o u t p o s s i b l e c o n f o u n d s t h a t t h r e a t e n i n t e r n a l validity. N o n e t h e l e s s , t h eh e u r i s t i c a n d c l i n i c a l v a l u e o f t h i s s t u d y s h o u l d n o t b e ignored. On average, individuals reported significantlyless distress a s s o c i a t e d w i t h t h e i r voices f o l l o w i n g treatm e n t , a n d all m e a s u r e s i n d i c a t e d f a v o r a b l e r e s u l t s . A d d i t i o n a l l y , t h e e f f e c t sizes f o r t h e t e s t s o f t h e a m o u n t o fchange on each measure from pre- to posttreatmentw e r e all l a r g e . T h i s is p a r t i c u l a r l y p r o m i s i n g g i v e n t h en a t u r a l i s t i c s e t t i n g o f t h i s s t u d y a n d s m a l l s a m p l e size.I n all, it a p p e a r s t h a t g r
In this article, we describe a pilot study that investigated the effectiveness of group cognitive behavioral therapy (CBT) for auditory hallucinations. . tial attempt to apply important clinical techniques devel- oped in the United Kingdom, particularly those that focus on reduction of auditory hallucinations, to work with inpatients in the .