Transcription
COGNITIVE BEHAVIOR THERAPYFOR SUBSTANCE USE DISORDERS:FROM THEORY TO PRACTICEHeather G. Fulton, PhD, RPsyc
LEARNING OBJECTIVES Describe overall theory of CBT, CBT for SUD specifically,and how this model guides individualized treatment Identify how a functional analysis can assist inconceptualization and tailoring of interventions within CBTfor SUD Differentiate between different types of coping skillsinterventions Refer to list of resources for further information on CBT forSUDs2
CBT Survey question Familiarity with CBT?3
4
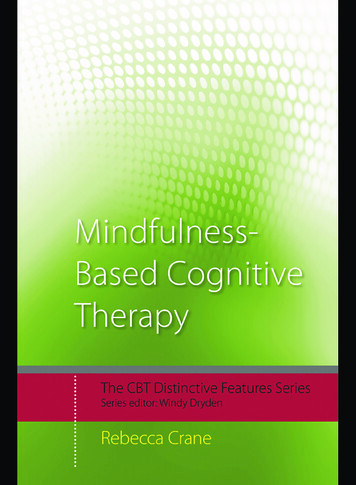
CBT MODELSamesituationbut howwe thinkabout itchangesouremotionsandbehaviorsThought: It’s a bear!Behavior: Run!Emotion: FearThought: It’s a baby deerBehavior: Slowlyturn around, takeout cameraEmotion: Curiosity?Excitement?5
CBT MODELThoughts/CognitionsBehaviorsEmotions6
CBT ensations“Hot cross bun” modelPadesky model7
WHAT ACTUALLY HAPPENS IN CBT? Techniques and strategies based on presenting problemsand client Common key elements throughout Collaborative relationship “coach”Interventions guided by individualized conceptualizationPresent-focusedIdentification of client goalsTime-limited, goal-focused sessionsSessions have a collaborative agenda; are structuredPsychoeducationOut of session practice* & review*avoid the term “homework”8
IS CBT EFFECTIVE? MANY studies on CBT “First line” or “best practice” for numerous disorders Supporting evidence for:ooooooooDepression & other mood disordersPTSDOCDAnxiety disorders (GAD, phobias, etc)Substance UsePsychosisChronic PainEtc For Reviews, check out: Tolin, , D.F. (2010). Is cognitive behavioral therapy more effective than other therapies? Ameta-analytic review. Clinical Psychology Review, 30, 710-720. Hoofman et al. (2012). The Efficacy of Cognitive Behavioral Therapy: A Review of Metaanalyses. Cognitive Therapy Research, 26(5), 427-440.9
CBT FOR SUBSTANCE USE DISORDERRelapsePreventionCoping SkillsTraining(Marlatt)(Monti, Kadden, Carroll)*Not reviewing Contingency Management, Motivational Interviewing,Community Reinforcement Approaches, Community Reinforcement andFamily Training, other couple, family or child-focused therapies10
CBT FOR SUD CBT for SUD found to be effective as monotherapy & incombination with other approaches- including olysubstance dependencee.g., Dutra et al., 2008; Magill & Ray, 2009; McHugh et al.,2010; Gates et al., 2016; Ray et al., 201811
QUESTIONS SO FAR?12
CASE EXAMPLECarl Male, 30s Alcohol Use, Cocaine use (intranasal), past history of hallucinogenand cannabis use Alcohol Use Disorder – mild Cocaine Use Disorder- severe Last use of cocaine and alcohol was 30days ago Comorbid depression, GAD Goal for treatment: “to get my use under control” “Probably not use any cocaine” Would like to drink alcohol socially still*details changed to protect confidentiality13
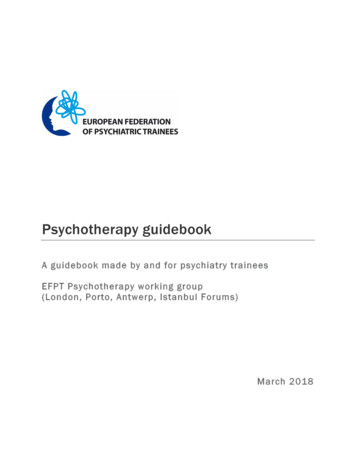
THEORY Addiction is a learned behavioro Classical conditioning (learned associations), operant conditioning(learning through consequences)o Biological, pharmacological, social contexts also play a roleMitcheson et al., 2010; Hendershot et al., 201114
Emotion photo credit: Ohio State UniversityYou feelanxiousOvertime this canYou feelanxiousLearning byYou take substances associationand feel more calm Learning byconsequencebecome You feel like you want to use substancesYou’re not sure how else to calm downapart from using substances 15
THEORY Addiction is a learned behavioro Classical conditioning (learned associations), operant conditioning(learning through consequences)o Biological, pharmacological, social contexts also play a role Addiction emerges and is maintained in an environmentalcontexto E.g. availability of substances, learning from peers/parents, socialdeprivation (e.g. other rewards), cultural influences Addiction is developed and maintained by thoughtpatterns and processeso E.g. outcome expectancies, permission to use, self-efficacy, affective stateMitcheson et al., 2010; Hendershot et al., 201116
CBT/RP ModelMarlatt & Gordon, 198517
Marlatt & Gordon, 198518
(transient over time)(stable over time)19
CBT FOR SUBSTANCE USEPrimary tasks of treatment:(1) Identify antecedents and determinants of substanceuse:-What specific needs are substances beingused to meet ?(2) Develop skills that provide alternative ways ofmeeting those needs20
FUNCTIONAL ANALYSIS Builds individualized conceptualization Fancy word for simple procedureo “slow mo’ replay”What was happening: Before During After21
22
CBT FOR SUBSTANCE USEPrimary tasks of treatment:(1) Identify antecedents and determinants of substanceuse:-What specific needs are substances beingused to meet ?(2) Develop skills that provide alternative ways ofmeeting those needs23
Recognizeantecendants,determinantsAvoid triggersIDwhen possibleUnderstand needs that substances being used to meetImprovePractice toIncreasePrevent lapses relapsesCopingOther ways tomeet needs?Challenge myths,beliefs24Marlatt & Gordon, 1985; Carroll, 1998
COPING SKILLS TRAINING Use tracking/ functional analysiso Thoughts, emotions and behaviors before, during, & aftercraving or useo Positive and negative consequences of use/no use Focus on present, current symptoms (thoughts, feelings,behaviors) Psychoeducation & address skill deficitso PRACTICE25
BASIC COPING SKILLSEveryone is different- ‘different tools in toolbox’ExperimentEmotion Regulation Distraction (esp. exercise) Talk to someone Mindfulness urge-surfing Examine & challenge self-talk, beliefs (outcome expectancy, permission giving, etc.) Keeping slip/lapse/use in perspective F#%* it FactorInterpersonal Refusal Skills AssertivenessOrganizational/problem solving difficulties Scheduling, agenda disorganization & time spent using Remember the negative consequences “play the tape through” Remembering values & goals Increasing pleasurable, meaningful activities including social connection and belonging alternativereinforcersCarroll, 1998; McHugh, Hearon & Otto, 2010; Mitcheson et al., 2010;26Allen et al., 2018; Ellingsen etal., 2018
BASIC COPING SKILLS CONTINUED Adjust for cognitive/learning abilities Rehearsal Imaginal exposure and/or rehearsal Behavior experiments Repetition Reminders can helpModifiedfrom SUBIWorkbook,2005;Carroll’swork27
CARLKey coping skills Identifying high risk situations Alone Using alcohol Feeling guilty, ashamed, hopeless, out of control Testing thoughts I’m just going to mess up later anyways, it’s hopeless I need a break (and cocaine will give it to me) People will judge me if they knew my history Doing fun activities that give a sense of mastery and pleasure Laundry, organizing things Biking Referral to couples counselling; meeting with partner about how to help cope Reviewed successful coping in high risk situations*details changed to protect confidentiality28
CARL Tapered last sessions (1x/week, 1x/2-3weeks, 1x/month) Had not used cocaine for 7months – despite encountering high risksituations (e.g. offers, seeing former dealer) Decided to avoid alcohol use for now Ongoing couples therapy Promoted in job*details changed to protect confidentiality29
ult/files/cbt.pdf30
REFERENCES Allen, A.M., Abdelwahab, N.M., Carlson, S., Bosch, T.A., Eberly, L.E., & Okuyemi, K. (2018). Effect of briefexercise on urges to smoke in men and women smokers. Addictive Behaviors, 77, 34-37. Carroll KM. A cognitive-behavioral approach: Treating cocaine addiction (NIH Publication 984308) Rockville, MD: National Institute on Drug Abuse; 1998 Dutra, L., Stathopoulou, G., Basden, S., Leyro, T.M., Powers, M.B., & Otto, M.W. (2008). A Meta-AnalyticReview of Psychosocial Interventions for Substance Use Disorders. The American Journal of Psychiatry, 165(2),179-187. Ellingsen, M.M., Johannesen, S.L., Martinsen, E.W., & Hallgren, M. (2018). Effects of acute exercise on drugcraving, self-esteem, mood and affect in adults with poly-substance dependence: Feasibility and preliminaryfindings. Drug and Alcohol Reviews, 37(6), 789-793. Gates, P.J., Sabionoi, P., Copeland, J., Le Foll, G., & Gowing, L. (2016). Psychosocial interventions forcannabis use disorders Psychosocial interventions for cannabis use disorder. Cochrane Database ofSystematic Reviews 2016(5), 1-135. DOI: 10.1002/14651858.CD005336.pub4 Hendershot C. S., Witkiewitz K., George W. H., & Marlatt G. A. (2011). Relapse prevention for addictivebehaviors. Substance Abuse Treatment, Prevention, and Policy, 6(1), 17. Hoofman et al. (2012). The Efficacy of Cognitive Behavioral Therapy: A Review of Meta-analyses. CognitiveTherapy Research, 26(5), 427-440.31
REFERENCES Magill, M. & Ray, L.A. (2009). Cognitive-Behavioral Treatment With Adult Alcohol and Illicit Drug Users: A MetaAnalysis of Randomized Controlled Trials. Journal of Studies on Alcohol and Drugs, 70(4), 516-527). Marlatt G.A. & Gordon, J.R. (1985). Relapse prevention. New York: Guilford Press. McHugh, R.K., Hearon, B.A., & Otto, M.W. (2010). Cognitive-Behavioral Therapy for Substance Use Disorders.Psychiatric Clinics of North America, 33(3), 511-525. Mitcheson, L., Maslin, J., Meynen, T., Morrison, T., Hill, R., & Wanigaratne, S. (2010). Applied Cognitive andBehavioural Approaches to the Treatment of Addiction: A Practical Treatment Guide. Chichester, UK: John Wiley &Sons. Padesky, C.A., & Mooney, K.A. (1990). Clinical tip: Presenting the cognitive model to clients. InternationalCognitive Therapy Newsletter, 6, 13-14. Ray, L.A., Bujarski, S., Grodin, E., Hartwell, E., Green, R., Venegas, A., Lim, A.C., Gillis, A., & Miotto, K. (2018).State-of-the-art behavioral and pharmacological treatments for alcohol use disorder. The American Journal ofDrug and Alcohol Abuse, 45(2), 124-140. The Substance Use Brain Injury Project Team. (2005) Client Workbook. Retrieved /SUBIClientWorkbook.pdf Tolin, D.F. (2010). Is cognitive behavioral therapy more effective than other therapies? A meta-analytic review.Clinical Psychology Review, 30, 710-720. Witkiewitz, K., & Marlatt, G. A. (2004). Relapse Prevention for Alcohol and Drug Problems: That Was Zen, ThisIs Tao. American Psychologist, 59(4), 224-235.32
Tolin, , D.F. (2010). Is cognitive behavioral therapy more effective than other therapies? A meta-analytic review. Clinical Psychology Review, 30, 710 -720. Hoofman et al. (2012). The Efficacy of Cognitive Behavioral Therapy: A Review of Meta - analyses. Cognitive Therapy Research, 26 (5), 427-440. 9