Transcription
Beyond Trauma:A Healing Journey for WomenTraining provided by:Twyla Wilson, LCSW112 Swift AvenueDurham, NC 27705Phone: 919-801-9087twyla.lcsw@gmail.comCurriculum written by:Stephanie S. Covington, Ph.D., L.C.S.W.Center for Gender and JusticeInstitute for Relational DevelopmentLa Jolla, justice.orgKSAODSAugust 19, 2015Louisville, KY
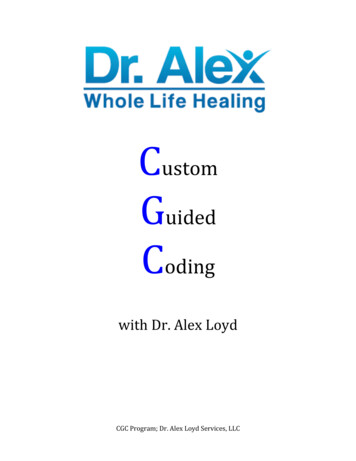
Beyond Trauma:A Healing Journey for WomenBeyond Trauma:A Healing Journey for WomenCrisis Danger & OpportunityTraining provided by:Twyla Wilson, LCSWDurham, NCKSAODSAugust 19, 2015Louisville, KYWritten by:Stephanie S. Covington, Ph.D., L.C.S.W.Center for Gender and JusticeInstitute for Relational DevelopmentLa Jolla, CA S. Covington, Ph.D., 2015Levels of Violence Childhood Adolescence Adult Street (workplace and community) Consumer Culture Media War Planet S. Covington, 2015 S. Covington, Ph.D., 2015Homicide Rates for Men Ages 15 - 24Around the WorldGlobal Violence(Rate per 100,000)Japan 1.6 million people worldwide die each yearfrom violence. More than 51,000 areAmericans.England & Wale sCanadaFr anceGe r m anySw itze r landGr e e ceDe nm ar kNe the r landsNor w aySw e de n Suicide accounts for 54% of violent deathsglobally, homicide for 35% and war and otherarmed conflict 11%.SpainAus tr iaIr e landPolandPor tugalScotlandFinlandAus tr aliaIs r ae lNe w Ze aland37.2ItalyUnite d State sSource: World Health OrganizationCenters for Disease Control and Prevention05101520253035 S. Covington, Ph.D., 2015 S. Covington, Ph.D., 2015KSAODSAugust 19, 2015Louisville, KY1
Beyond Trauma:A Healing Journey for WomenStatisticsStatisticsThe following statistics illustratehow pervasive interpersonal violence isin the lives of women and girls. 1 in 6 women will be sexually assaulted in her lifetime,with college age women 4 times more likely to be sexuallyassaulted (RAINN, 2007). More than half of rapes occur before age 18 and 22%occur before age 12 (CDC, 2009b). A woman is battered every 15-18 seconds (UnitedNations Commission on the Status of Women, 2000). Approximately 1.5 million women are raped orphysically assaulted by an intimate partner each year inthe US. Women under 24 years of age suffer thehighest rates of rape (NOW, 2010). There is one sexual assault every about every twominutes. (FBI CIUS, 2008). 1 in 5 girls and 1 in 10 boys are sexually victimized beforeadulthood (Nat’l Center for Missing and ExploitedChildren, 2008). In homes where DV occurs, children are seriously abusedor neglected at a rate that is 1,500% higher than thenational average for the general population (Children’sDefense Fund Ohio, 2009). S. Covington, Ph.D., 2015 S. Covington, Ph.D., 2015StatisticsStatistics Children from violent homes have a higher tendency tocommit suicide, abuse drugs and/or alcohol, and commitviolence against their own partners and children (Whitfield,Anda, Dube, and Felitti, 2003). More than 30 million children in the U.S. live in low-incomefamilies, and 14 million children live in poverty (Wight,Chau, and Aratani, 2010). While both male and female children are at risk for abuse,females continue to be at risk for interpersonal violence intheir adolescence and adult lives (Covington & Surrey). At least 50% of child abuse and neglect cases areassociated with parental drug or alcohol abuse (ECMEF,2008). One or more parents were responsible for 70% of childfatalities caused by abuse or neglect (HHS, 2008a). Children born into poverty risk exposure to violence that isso high they are guaranteed to be affected by trauma(Women’s Law Project, 2002). In 2005, 1,181 women were murdered by their intimatepartner -- more than 3 women murdered per day (FVPF,2009b).StatisticsStatistics If a victim of domestic violence, a woman is 80%more likely to have a stroke, 70% more likely todrink heavily or to have a heart attack, 60% morelikely to have asthma (FVPF, 2009d). 1/3 of women in state prison and 1/4 in jails saidthey had been raped (BJS, 1999). While relationship violence happens to women ofevery race and ethnic background, AfricanAmerican women are physically assaulted at arate that is 35% higher than Caucasian women,and about 2-1/2 times the rate of women of otherraces. (National Coalition Against DomesticViolence, 2000). Every year there are 2 million injuries from domesticviolence (CDCP, 2008). S. Covington, Ph.D., 2015 Women in prison reported childhood abuse at arate almost twice that of men; abuse of women asadults was eight times higher than the rate formen (Messina et. al., 2001). Between 23-37% of female offenders reportedthat they had been physical or sexually abusedbefore the age of 18 (BJS, 1999).KSAODSAugust 19, 2015Louisville, KY2
Beyond Trauma:A Healing Journey for WomenViolence Against WomenSexual Assault GraphViolence against women is so pervasive that the UnitedNations has addressed and defined violence againstwomen as “any act of gender-based violence that resultsin, or is likely to result in, physical, sexual or psychologicalharm or suffering to women, including threats of such acts,coercion or arbitrary deprivations of liberty, whetheroccurring in public or private life.”(United Nations General Assembly, 1993).Bureau of Justice Statistics S. Covington, Ph.D., 2015Sexual Assault Graph S. Covington, Ph.D., 2015Moral Challenges 19th century - slavery 20th century - totalitarianism 21st century – brutalityagainst women and girls(NY Times 9/23/09)Bureau of Justice Statistics S. Covington, Ph.D., 2015 S. Covington, Ph.D., 2015Two Kinds of SufferingDefinition of TraumaThe diagnostic manual used by mental healthproviders defines trauma as: Natural Createda) exposure to actual or threatened death,serious injury or sexual violation. (American Psychiatric Assoc. [APA] DSM-5) S. Covington, Ph.D., 2015 S. Covington, Ph.D., 2015KSAODSAugust 19, 2015Louisville, KY3
Beyond Trauma:A Healing Journey for WomenDefinition of Trauma (cont.)Definition of Trauma (cont.) The exposure must result from one or more of The disturbance, regardless of its trigger,causes significant distress or impairment inthe individual’s social interactions, capacityto work, or other important areas offunctioning.the following scenarios in which the individual: directly experiences the traumatic event; witnesses the traumatic event in person; learns that the traumatic event occurred to a close family member or close friend;(It is not the physiological result of another medicalcondition, medication, drugs or alcohol.) experiences first-hand repeated or extremeexposure to aversive details of the traumaticevent (not through media, pictures, television ormovies unless work-related). (American Psychiatric Assoc. [APA] DSM-5(American Psychiatric Assoc. [APA] DSM-5) S. Covington, 2015 S. Covington, Ph.D., 2015)POSTTRAUMATIC STRESSDISORDERPOSTTRAUMATIC STRESSDISORDER (con’t.)Presence of one or more of the following: Recurrent, involuntary ,intrusive symptoms, such asdreams, memories related to the traumatic event(s) Dissociative symptoms, including flashbacks, on acontinuum including complete loss of time Intense or prolonged psychological stress at exposureto internal or external cues Marked physiological reactions to internal or externalcues that symbolize or resemble an aspect of thetraumatic event(s)Persistent avoidance of stimuli after the event: avoidance or efforts to avoid distressing memories,thoughts, or feelings about or closely associated withthe traumatic event(s) Avoidance of or efforts to avoid external reminders thatarouse distressing memories, thoughts or feelingsNegative alterations in cognitions and mood associatedwith the traumatic events(s)as evidenced by two or moreof the following:Inability to remember an important aspect of thetraumatic event(s) not due to use of drugs or alcohol,head injuryPOSTTRAUMATIC STRESSDISORDER (con’t.)POSTTRAUMATIC STRESSDISORDER (con’t.) Persistent and exaggerated negative beliefs orexpectations about oneself, others, or the worlde.g. “I am bad; No one can be trusted; the world iscompletely dangerous, My whole nervous system iscompletely ruined”Persistent, distotred cognitions about the cause orconsequences of the traumatic event(s) that lead theindividual to blame him/herself or othersPersistent negative emotional statee.g. fear, horror, anger, guilt, or shame Marked or diminished interest or participation insignificant activities Feelings of detachment or extrangement from others Persistent inability to experience posibtive emotionse.g. inability to experience happiness, satisfaction, orloving feelingsMarked alterations in arousal and reactivity associatedwith the traumatic events(s), beginning or worsening afterthe traumatic event(s) occurred as evidenced by two ofthe following:KSAODSAugust 19, 2015Louisville, KY4
Beyond Trauma:A Healing Journey for WomenPOSTTRAUMATIC STRESSDISORDER (con’t.)POSTTRAUMATIC STRESSDISORDER (con’t.) Irritable behavior and angry outbursts (with little orno provocation) typically expressed as verbal orphysical aggression toward people or objects Reckless or self-destructive behavior Hypervigilance Exaggerated startle response Problems with concentration Sleep disturbance(Present for more than one month) G) the disturbance causes clinically significant distressor impairment in social, occupational, or other importantareas of functioning H) the disturbance is not attributable to thephysiological effects of a substance or another medicalcondition Specify “With dissociative symptoms” ifdepersonalization (feeling detached, or an impartialobserver) or derealization (feeling unreality ofsurroundings such as dreamlike, unreal, distant ordistorted) are present Specify “With delayed expression” if full criteria are notmet until at least 6 months after the eventHistorical TraumaTrauma and Substance Abuse Across generationsThe women with more experiences of trauma hadmore severe substance abuse issues. Massive group trauma Examples include: Native Americans, AfricanAmericans, Holocaust survivors, Japanese internmentsurvivors S. Covington, Ph.D., 2015 S. Covington, Ph.D., 2014Source: Johnson, Cottler, O’Leary, & Abdallah, 2010Abuse and Substance UseSubstance UseAbuse within the first five years of life is significantlyassociated with substance use in girls as young as twelve,through the teen years, and in the early twenties.Women who experience more than one sexual assault are3.5 times more likely to either start or increase thefrequency of their substance use than women with onlyone assault experience. S. Covington, Ph.D., 2014Source: Lansford, Dodge, Pettit, & Bates, 2010 S. Covington, Ph.D., 2014Source: McFarlane, Malecha, Gist, Watson, Batten, Hall, & Smith, 2005KSAODSAugust 19, 2015Louisville, KY5
Beyond Trauma:A Healing Journey for WomenSexual Abuse and Mental HealthPost-traumatic Stress Disorderand Substance AbuseWomen who have histories of sexual assaultcommonly experience multiple factors: 65 percent experience PTSD 51 percent experience depression 82 percent develop anxiety 49 percent become dependent on alcohol 61 percent use illicit substances 44 percent experience thoughts of suicide 19 percent attempt suicideWomen’s abuse of drugs and alcohol often isreported to start at the same time as symptoms ofpost-traumatic stress disorder begin, in contrast tomen, who more often begin substance abuse prior toPTSD symptoms. S. Covington, Ph.D., 2014Source: Campbell, Dworkin, & Cabral, 2009 S. Covington, Ph.D., 2014Source: Sonne, Back, Diaz, Randall, & Brady, 2003America Has an Incest ProblemAmerica Has an Incest Problem(January 2013)(January 2013)Child sexual abuse impacts more95% of teen prostitutes andAmericans annually than cancer, AIDS, gunat least 35% of female prisonersviolence, LGBT inequality, and thewere abused as kids.mortgage crisis combined.32 S. Covington, Ph.D., 2013Fontaine, January 2013. “America Has an Incest Problem”. The Atlantic.33 S. Covington, Ph.D., 2013Fontaine, January 2013. “America Has an Incest Problem”. The Atlantic.America Has an Incest ProblemAmerica Has an Incest Problem(January 2013)(January 2013)Sexually abused youth are:Incest is the single biggest commonality Twice as likely to be arrested for a violencebetween drug and alcohol addiction, mentaloffense as adultsillness, teenage and adult prostitution, Twice the risk for lifelong mental health issuescriminal activity, and eating disorders. Twice as likely to attempt or commit teen suicide34Fontaine, January 2013. “America Has an Incest Problem”. The Atlantic. S. Covington, Ph.D., 201335 S. Covington, Ph.D., 2013Fontaine, January 2013. “America Has an Incest Problem”. The Atlantic.KSAODSAugust 19, 2015Louisville, KY6
Beyond Trauma:A Healing Journey for WomenThe Longest Waris the One Against WomenThe Longest Waris the One Against Women (cont.)By Rebecca SolnitHomicide 1976-2005 88.8% men 11.2% womenHomicide (guns) 91.3% men 8.7% womenHomicide (multiple victims) 93.5% men 6.5% 0Published on Thursday, January 24, 2013 by TomDispatch.com S. Covington, 2015 S. Covington, 2015R. Solnit, 2013The Longest Waris the One Against Women (cont.)The Longest Waris the One Against Women (cont.) Most perpetrators of violence are menPandemic of violence by menagainst women, both intimate and Doesn’t mean all men are violentstranger violence Men also suffer violence, largely at thehands of other men S. Covington, 2015R. Solnit, 2013 S. Covington, 2015R. Solnit, 2013Men, Violence & Trauma“What I have concluded from decades ofworking with every kind of violentcriminal is that the way to prove one’smanhood to gain respect is to commita violent act.” 75 percent of student suspensions, expulsions, gradefailures, special-education referrals, school-violencecasualties, and all other assaults are for boys 75 percent of teenage suicides are boys 70 percent of all suicides are boys/men- James Gilligan 80 percent of the homeless are boys/men(Lyme et al., 2006) S. Covington, 2015 S. Covington, 2015KSAODSAugust 19, 2015Louisville, KY7
Beyond Trauma:A Healing Journey for WomenMen, Violence & TraumaHow Men Respond to Trauma(cont.) 80 percent of homicide victims are men 93 percent of prison inmates are men 99 percent of executed prisoners are men (in the lastdecade, 700 men and 10 women)(Lyme et al., 2006) Men respond differently to similar events: “No big deal” “Just get over it” “Suck it up” “Don’t be a wimp” “Never let them see you sweat” “Pull yourself up by your bootstraps!” “Suffer in Silence” But the real reason is . S. Covington, 2015 S. Covington, 2015“Real Men Can Handle Anything!”What does the prevalencedata tell us? Many people with trauma histories haveoverlapping problems with mentalhealth, substance abuse, physicalhealth and are victims or perpetrators ofcrime. Victims of trauma are found across allsystems of care. S. Covington, 2015 S. Covington, 2015Source: NASMHPD 2008Therefore We need to presume the people we serve have ahistory of traumatic stress and exercise “universalprecautions.” **Universal expectationsUniversal design S. Covington, 2015 S. Covington, 2015(Source: NASMHPD 2008)KSAODSAugust 19, 2015Louisville, KY8
Beyond Trauma:A Healing Journey for WomenTheoretical FoundationTreatment StrategiesThe theories related to gender and substanceabuse (and any other relevant treatmentservices) that create the framework of thoughtfor program development.This is theknowledge base that creates the foundationupon which the program is developed.The approaches used in the program thatcreate the therapeutic process. These arethe ways in which theory is operationalized(how theory is applied). S. Covington, Ph.D., 2015 S. Covington, Ph.D., 2015Core Principlesof Trauma Informed CareTheoretical Foundations Safety (physical and emotional)Relational Theory & FemalePsychological Development Trustworthiness ChoiceAddiction Theory Collaboration Trauma Theory Empowerment(Fallot & Harris, 2006) S. Covington, Ph.D., 2015 S. Covington, Ph.D., 2015Trauma Specific ServicesTRAUMA SPECIFICServices designed specifically to address violence,trauma, and related symptoms and reactions. The intent Beyond Trauma:A Healing Journey for Womenof the activities is to increase skills and strategies thatallow survivors to manage their symptoms and reactionswith minimal disruption to their daily obligations and to Healing Trauma:Strategies for Abused Womentheir quality of life; and eventually to reduce or eliminatedebilitating symptoms and to prevent further Beyond Violence:A Prevention Program for Womentraumatization and violence. S. Covington, Ph.D., 2015KSAODSAugust 19, 2015Louisville, KY9
Beyond Trauma:A Healing Journey for WomenBeyond Trauma:Healing Trauma:A Healing Journey for WomenStrategies for Abused Women11 sessions5 sessionsEvidence-Based Researched in Residential treatment Women’s prison Drug courtListed on NREPP S. Covington, Ph.D., 2015 S. Covington, 2015Trauma Materials for WomenDefinition of Evidence-based ATRIUM (Dusty Miller) Beyond Trauma (Stephanie Covington)Evidence-based practice (EBP) isdefined as the integration of the bestavailable research and clinical expertisewithin the context of patientcharacteristics, culture, values, andpreferences. Healing Trauma (Stephanie Covington) Seeking Safety (Lisa Najavits) TREM (Maxine Harris)Trauma Materials for Men M-TREM (Roger Fallot)(APA Presidential Task Force, 2005) S. Covington, 2015When is Someone Ready for TraumaProcessing?Beyond Anger and Violence:A Program for Women She/he is able to use some safe coping skills She/he has no major current crises or instability(e.g., homelessness or domestic violence) She/he is willing to do this type of work She/he can reach out for help when in dangerFacilitator Guide She/he is not using substances to such a severedegree that emotionally upsetting work mayincrease her/his useParticipant Workbook S. Covington, 201559 S. Covington, Ph.D., 2015KSAODSAugust 19, 2015Louisville, KY10
Beyond Trauma:A Healing Journey for WomenA Culture Shift:THERAPEUTIC APPROACHESChanges in Understanding and Practice Relational-Cultural Group Therapy Psychodynamic Cognitive-Behavioral Experiential Therapeutic Community Mutual Help Thinking differently as a prelude to actingdifferently Thinking differently initiates and sustainschanges in practice and setting Acting differently reinforces and clarifieschanges in understandingSource: Roger Fallot, Ph.D.A Culture Shift: Scope of Changein a Distressed SystemEmerging Paradigm Involves all aspects of program activities, setting,relationships, and atmosphere (more thanimplementing new services) Involves all groups: administrators, supervisors,direct service staff, support staff, and consumers(more than service providers) Involves making trauma-informed change into anew routine, a new way of thinking and acting(more than new information)Source: Roger Fallot, Ph.D. S. Covington, 2015Values-Based Services Gender-responsiveTrauma-informedCulturally competentRecovery-oriented S. Covington, 2015Three Critical andInterrelated IssuesChildhood Traumatic EventsLargest Effect-Mental HealthSubstance Abuse Psychotropic medicationMental Health Mental health treatmentTrauma Attempted suicide Traumatic stress(Messina & Grella, 2005) S. Covington, Ph.D., 2015 S. Covington, Ph.D., 2015KSAODSAugust 19, 2015Louisville, KY11
Beyond Trauma:A Healing Journey for WomenAddiction – Trauma – Mental Health IssuesA Repetitive Cycle of RiskIncarcerationAreas of SeparationHomelessnessViolence andTraumaTrainingTreatmentSubstance AbuseCategorical FundingMental HealthProblemsRoger Fallot, Ph.D.What does the prevalencedata tell us? S. Covington, Ph.D., 2015Therefore Many people with trauma histories haveoverlapping problems with mentalhealth, substance abuse, physicalhealth and are victims or perpetrators ofcrime.We need to presume the women weserve have a history of traumatic stressand exercise “universal precautions.” Victims of trauma are found across allsystems of care.(Source: NASMHPD 2008)(Source: NASMHPD 2008) S. Covington, Ph.D., 2015Beyond Trauma: A Healing Journeyfor Women S. Covington, Ph.D., 2015Key Elements(Staff and Clients)Three Modules:Violence, Abuse and Trauma Learn what trauma/abuse isThe Impact of Trauma on Women’s Lives Understand typical responsesHealing from Trauma Develop coping skillsIntegrates cognitive-behavioral, expressive arts,guided imagery, and relational therapy. S. Covington, Ph.D., 2015 S. Covington, Ph.D., 2015KSAODSAugust 19, 2015Louisville, KY12
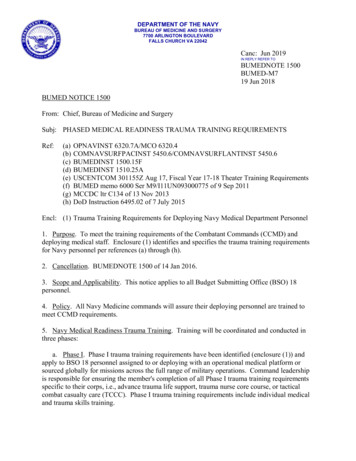
Beyond Trauma:A Healing Journey for WomenProcess of TraumaDisorders Related to Trauma andSubstance Abuse in Women’s LivesTraumatic EventOverwhelms the physical and psychological coping skillsResponse to TraumaDisorders Related to Trauma and Substance Abuse:Fight, Flight, Freeze or FaintAltered state of consciousness, Body sensations, Numbing,Hyper-vigilance, Hyper-arousal, Collapse Depressive Disorders NOS22.9%Sensitized Nervous SystemChanges in the BrainBrain–Body Connection Major Depressive Disorders17.5% Post traumatic Stress Disorders16.3%Psychological and/or Physical Distress Neurotic Anxiety Disorders13.8% Bipolar Disorders13.7%Current stressors, Reminders of trauma (triggers)Sensations, Images, Behavior, Affect, MemoryMental and/or Physical ietyHarmful Behaviorto SelfHarmful Behaviorto OthersPhysicalHealth IssuesSubstance abuseEating disordersSelf-injurious behaviorSuicidal actionsAggressionViolenceRagesThreatsLung DiseaseHeart diseaseAutoimmune disordersObesityAdapted from:Stephanie S. Covington, Beyond Trauma: A Healing Journey for Women, 2003, Center City, MN: Hazelden.Peter Levine, Healing Trauma: A Pioneering Program for Restoring the Wisdom of Your Body, 2008, Boulder, Colorado: Sounds True. Mood or Dysthymic Disorders5.3% Psychotic Disorders4.8% Personality and Misc. Disorders5.8%Source: Patterns of Comorbidity among Women with Childhood Interpersonal Trauma, Mental Health Disorders, and Substance RelatedDisorders. Journal of Behavioral Health Services & Research (in press) S. Covington, Ph.D., 2015 S. Covington, Ph.D., 2015Post-traumaticStress DisorderPost-traumaticStress Disorder (cont.) Re-experiencing the event through nightmares andflashbacks. Numbing of general responsiveness (feelingnothing most of the time) Avoidance of stimuli associated with the event (forexample, if a woman was raped in a park, she mayavoid parks, or if she was assaulted by a blonde man,she may avoid men with blonde hair). Hyper-vigilance (constantly scanning one’senvironment for danger, whether physical oremotional) Estrangement (the inability to be emotionally close toanyone) Exaggerated startle response (a tendency to jumpat loud noises or unexpected touch) (DSM – IV) S. Covington, Ph.D., 2015Post-traumaticStress Disorder (cont.) S. Covington, Ph.D., 2015Disorders Related toPost-traumatic Stress Disorder Depression Anxiety Panic disorder Phobic disorder Substance abuse Physical disordersThree Symptom Clusters: Re-experiencing Numbing and Avoidance HyperarousalSource: Davidson, J. (1993) “Issues in the diagnosis of posttraumatic stress disorder.”In American Psychiatric Review of Psychiatry, Vol. 12 S. Covington, Ph.D., 2015 S. Covington, Ph.D., 2015KSAODSAugust 19, 2015Louisville, KY13
Beyond Trauma:A Healing Journey for WomenDr. Peter LevineDEVELOPMENTAL TRAUMADISORDER Waking the Tiger: Healing Trauma In An Unspoken Voice: How the BodyReleases Trauma and Restores GoodnessBessel van der Kolk, M.D.The Trauma CenterBrookline, MAwww.traumacenter.orgEmail: moreinfo@traumacenter.org traumahealing.orgTraumaTrauma: Stages of RecoveryThree Group ModelsSyndromeStage OneStage TwoStage ThreeHysteria(Janet tion litationRe-experiencingtraumaIntegration oftraumaCombat trauma Trust, stressScurfield (1985) managementeducationRecoveryStage OneRecoveryStage TwoRecoveryStage ThreeTherapeutictaskSafetyRemembranceand ent, psGroupSource: Herman, 1992, 1997Source: Herman, 1992, 1997 S. Covington, Ph.D., 2015 S. Covington, Ph.D., 2015TraumaTraumaThree Group ModelsThree Group ModelsRecoveryStage OneRecoveryStage TwoRecoveryStage ThreeConflicttoleranceLowLowHighStable, slowturnoverTime limitOpen-ended orrepeatingFixed nstructuredSurvivor groupInterpersonalpsychotherapygroupRecoveryStage OneRecoveryStage TwoRecoveryStage Very highGroupGroupExampleTwelve-stepprogramsSource: Herman, 1992, 1997Source: Herman, 1992, 1997 S. Covington, Ph.D., 2015 S. Covington, Ph.D., 2015KSAODSAugust 19, 2015Louisville, KY14
Beyond Trauma:A Healing Journey for WomenWhen is a Woman Ready forTrauma Processing?Trauma SpiralTransformation She is able to use some safe coping skills She has no major current crises or instability (e.g.,homelessness or domestic violence) She is willing to do this type of work She can reach out for help when in dangerTrauma(constriction) She is not using substances to such a severedegree that emotionally upsetting work mayincrease her useHealing(expansion) S. Covington, Ph.D., 2015 S. Covington, Ph.D., 2015When is a Woman Ready forTrauma Processing?Secondary Traumatic Stress(STS) Her suicidality has been evaluated and taken intoaccount Compassion fatigue She is in an ongoing system of care that is stableand consistent, with no immediate plannedchanges (e.g., discharge from inpatient unit orresidential program) Burnout Vicarious traumatization S. Covington, Ph.D., 2015 S. Covington, Ph.D., 2015Vicarious Traumatization SpiralKey Elements(Prevention) EmpathicEngagement Self-CarePractices Repeated exposureto trauma histories ProfessionalSupports Traumatic StressSymptoms ClinicalSupervision Apathy/Cynicism Re-connectionto hope/meaningVicarious Trauma(constriction)(Staff and Clients) Learn what trauma/abuse is Understand typical responses Develop coping skillsIntervention(expansion)KSAODSAugust 19, 2015Louisville, KY15
Beyond Trauma:A Healing Journey for WomenWhat Makes a Good Facilitator?The following qualities in a facilitator will help toensure a positive group experience: Trustworthy Credible Available Reliable, consistent Hopeful Warm, compassionate Emotionally matureWhat Makes a Good Facilitator?(cont.) Healthy boundaries, respects confidentiality Committed to and interested in women’s issues Multi-cultural sensitivity and responsiveness Appropriate gender - a female should facilitate theall-female groups S. Covington, Ph.D., 2015 S. Covington, Ph.D., 2015What Makes A Good Facilitator?Role of the Facilitator(cont.) If a trauma survivor, she needs to feel confidentthat she is at a place in her own recovery that willallow for healthy and positive outcomes for herselfand the women in the group. Content expertise, if possible Skills as a facilitator Begin and end on time Maintain structure of the group Move the group through the content of eachsession Lead by example by having appropriateboundaries and containing your feelings Allow each woman to have her own experience ofthe group S. Covington, Ph.D., 2015 S. Covington, Ph.D., 2015“Therapeutic culture”has these elementsWhat Makes a Difference? Creating a safe environment Listening to her story Empathy Attachment: a culture of belongingContainment: a culture of safetyCommunication: a culture of opennessInvolvement: a culture of participation andcitizenship Agency: a culture of empowerment(Haigh) S. Covington, Ph.D., 2015KSAODSAugust 19, 2015Louisville, KY16
Beyond Trauma:A Healing Journey for WomenTen Principles ofTrauma-Informed ServicesTen Principles ofTrauma-Informed Services (cont.)1. Trauma-Informed Services Recognize theImpact of Violence and Victimization onDevelopment and Coping Strategies2. Trauma-Informed Services Identify Recoveryfrom Trauma as a Primary Goal3. Trauma-Informed Services Employ anEmpowerment Model4. Trauma-Informed Services Strive to MaximizeChoices and Control Over One’s OwnRecovery5. Trauma-Informed Services Are Based in aRelational Collaboration6. Trauma-Informed Services Create anAtmosphere That Is Respectful of Survivor’sNeed for Safety, Respect, and Acceptance7. Trauma-Informed Services EmphasizeStrengths, Highlighting Adaptation OverSymptoms and Resilience Over Pathology8. The Goal of Trauma-Informed Services Is toMinimize the Possibilities of RetraumatizationTen Principles ofTrauma-Informed Services (cont.)What would be observedin a setting?9. Trauma-Informed Services Strive to BeCulturally Competent and to Understand EachPerson in the Context of Their LifeExperiences and Cultural Background10. Trauma-Informed Agencies Solicit ConsumerInput and Involve Consumers in Designing andEvaluating ServicesTrauma InformedNot Trauma Informed Recognition of highprevalence of trauma Assess for traumatichistories & symptoms Lack of education ontrauma prevalence &“universal precautions” Cursory or no traumaassessment Recognition of cultureand practices that are retraumatizing “Tradition of toughness”valued as best careapproachElliot, D.E.; Bjelajac, P.; Fallot, R.D.; Markoff, L.S.; Reed, B.G. Trauma-Informed orTrauma-Denied: Principles and Implementation of Trauma-Informed Services forWomen. Journal of Community Psychology, July, 2005., 33(4): 461-477.Source: NASMHPD 2008 S. Covington, Ph.D., 2015What would be observed in asetting?What would be observedin a setting?Trauma InformedNot Trauma Informed Power/Control minimized– constant attention toculture Staff demeanor, tone ofvoice Power
A Healing Journey for Women KSAODS August 19, 2015 Louisville, KY 1 Beyond Trauma: A Healing Journey for Women Training provided by: Twyla Wilson, LCSW Durham, NC KSAODS August 19, 2015 Louisville, KY Written by: Stephanie S. Covington, Ph.D., L.C.S.W Center for Gender and Justice Institute for Relational Developmen La Jolla, CA