Transcription
AAFP ChronicPain ToolkitHOP20012003
AAFP Chronic Pain ToolkitINTRODUCTIONChronic pain is commonin the U.S., with anywherefrom 11% to 40% of theadult population reportingdaily pain.1 Approximatelyone-third of patientsexperiencing pain receivea pain medication.2 Whilethe number of prescriptionsfor pain managementhave declined in recentyears,3 opioid misuseremains a significant publichealth crisis. Roughly21-29% of patients whoare prescribed opioidsfor chronic pain willmisuse them.4The solutions to thispublic health crisis includecontinued emphasis onimproving chronic paincare, increasing researchinto pain and painmanagement, improvingtraining for physicianswho manage chronicpain, and increasedpublic awareness.Scope and PurposeThis toolkit serves as oneprimary care solutionto assist in the effectiveassessment, diagnosis,and management ofchronic pain. It provides abrief overview of currentevidence, along withuseful tools and resourcesto manage chronic painand related issues. Thesesections and tools canbe used together orseparately, depending onthe needs of the practice.Toolkit Sections*Section TitleDescriptionLocation1. Pain AssessmentOverview of appropriate strategies and diagnostic tools tosupport chronic pain assessment in patientsJump to section2. Functional and OtherAssessmentsOverview of strategies and supporting tools for the diagnosticJump to sectionassessment of functional activity and other coexisting conditionsin patients, including mental and emotional health, quality of life,and other psychological factors3. Pain ManagementOverview of strategies and considerations for effective acute and Jump to sectionchronic pain management in patients4. Opioid PrescribingOverview of opioid prescribing as related to the treatmentof chronic pain, including information and resources for safeprescribing; risk mitigation and monitoring; opioid conversionand tapering tools; and opioid resources for patientsJump to section5. Opioid Use Disorders:Prevention, Detection,and RecoveryOverview and resources to support opioid use disorderprevention; recognition and assessment; and treatment andrecoveryJump to section* External tools or resources included in this toolkit do not constitute or imply an endorsement by theAmerican Academy of Family Physicians (AAFP). Views and opinions expressed in external websitesor documents do not necessarily reflect those of the AAFP and are intended to help physicians intheir treatment of patients with chronic pain. The AAFP has no control over the content of externalwebsites or accuracy of all content contained by those external websites.AcknowledgementsWe would like to thank the following individuals for their contributions to the content and designof the toolkit.Panel of Family Medicine Experts:AAFP Project Leadership Team:Benjamin Crenshaw, MDCarissa van den Berk-Clark, PhD, LMSWDaniel Mullin, PsyD, MPHLynn Fisher, MDMolly E. Rossignol, DO, FAAFP, FASAMWayne Reynolds, DOCory Lutgen, BSMelanie Bird, PhD, MSAMNatalia Loskutova, MD, PhDThe AAFP Chronic Pain Toolkit was developed by the AAFP with funding support (inpart) by grant no. 6H79TI080816 from the Substance Abuse and Mental Health ServicesAdministration (SAMHSA). The views expressed in written conference materials ofpublications and by speakers and moderators do not necessarily reflect the official policiesof the U.S. Department of Health and Human Services (HHS); nor does mention of tradenames, commercial practices, or organizations imply endorsement by the U.S. government.References1. Centers for Disease Control and Prevention. Prevalence of chronic pain and high-impact chronic pain amongadults — United States, 2016. MMWR. 2018;67(36):1001-1006.2. Harrison JM, Lagisetty P, Sites BD. Trends in prescription pain medication use by race/ethnicity among USadults with noncancer pain, 2000-2015. Am J Public Health. 2018;108(6):788-790.3. Centers for Disease Control and Prevention. U.S. opioid dispensing rate maps. Accessed January 7, l#: :text lion%20opioid%20prescriptions4. National Institute on Drug Abuse. Opioid overdose crisis. Accessed January 7, overdose-crisisHOP200120031AMERICAN ACADEMY OF FAMILY PHYSICIANS
AAFP Chronic Pain ToolkitPAIN ASSESSMENT Section 1OVERVIEWAssessment of chronic pain should be multidimensional. Consideration should be given toseveral domains, including the physiological features of pain and its contributing factors,with physicians and other clinicians assessing patients for function, quality of life, mentalhealth, and emotional health.In addition to a complete medical and medication history typically obtained at an office visit,documentation should be obtained about pain intensity, location, duration, and factors thataggravate or alleviate pain.A physical exam should include musculoskeletal and neurological components, asappropriate. Diagnostic testing and imaging may also be considered for some types ofchronic pain. Many organizations, including the AAFP, recommend against imaging forlow back pain within the first six weeks of treatment unless there are reasons for theimaging. These reasons may include concerns of underlying conditions, such as severe orprogressive neurological deficits, or if osteomyelitis is suspected.1Periodic reassessments of chronic pain and treatment should focus on evaluatingimprovements in physical health; mental and emotional health; progress towards functionaltreatment goals; and effectiveness and tolerability of medications for chronic paintreatment.Currently, there are no universally adopted guidelines or recommendations for assessmentof chronic pain. The use of appropriate assessment tools can assist in diagnosticassessment, management, reassessment, and monitoring of treatment effects. Multipletools are available, with many embedded in electronic health record (EHR) systems.Pain Assessment ToolsThe table on the next page includes selected tools for pain assessment included in thistoolkit, along with links and reference to additional tools. Assessments about other relevantdomains are covered in Functional and Other Assessments (Section 2).2AMERICAN ACADEMY OF FAMILY PHYSICIANS
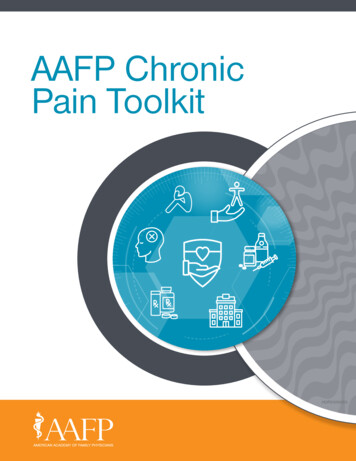
AAFP Chronic Pain ToolkitPain Assessment Tools in ToolkitNameUseScoringDescriptionLocationBrief PainInventory(BPI) ShortFormAssess pain severityand impact on dailyfunction Worst pain score: 1-4 mild pain Worst pain score: 5-6 moderate pain Worst pain score: 7-10 severe painFillable PDF completed inapproximately five minuteswith the patientJump to tool in toolkit.Pain severity can be calculated byaveraging responses of questions 3-6.Pain interference can be calculated byaveraging responses of questions 9a-9g.Pain,Enjoymentof Life andGeneralActivity(PEG) ScaleAssess paininterference withenjoyment of life andgeneral activity Mild pain 0-11 or 0 to 4 Moderate pain 12-20 or 4 to 7 Severe pain 21-30 or 7-10Three-question assessment Jump to tool in toolkit.of pain takes 1-2 minutesPEG score is calculated by an average ofquestions 1-3Additional Pain Assessment ToolsNumeric PainRating Scale(NPRS)2Rate pain intensityScores range from 0-10 points, withhigher scores indicating greater painintensity.Evaluates one aspect asures/numeric-pain-rating-scaleEvaluates pain experiencedonly in the past 24 hoursor “an average painintensity”Verbal Rating Describe pain intensityScale (VRS)3Use when the NPRScannot be used No pain Mild pain Moderate pain Severe painWord options describe pain interactive-pdf-003.pdfWong-BakerFACES PainRating Scale4Series of faces range from 0 for a happyface (no hurt) to 10 for a crying face(hurts worst)Faces depict the pain thepatient experiencesDescribe pain intensityUsed for children andadultsAssess quality andMcGill PainQuestionnaire intensity of pain(MPQ)5Monitor pain overtime and determineeffectiveness s one aspect ofpain—intensityScores are calculated by summing values Numerical intensity scaleassociated with each wordSet of descriptor wordsScores range from 0 (no pain) to 78and a pain drawing(severe -pain-questionnaireFor additional resources on assessment algorithms, visit the Institute for Clinical Systems Improvement’sguideline, Pain; Assessment, Non-Opioid Treatment Approaches and Opioid Management.References1. A merican Academy of Family Physicians. Imagining for low back pain. Choosing Wisely . Accessed January 7, 2021. ack-pain.html2. Shirley Ryan AbilityLab. Numeric Pain Rating Scale. Accessed January 7, 2021. n-rating-scale3. Jensen MP. The 0-3 Verbal Rating Scale (VRS). Accessed January 7, 2021. ive-pdf-003.pdf4. Wong-Baker FACES Foundation (2020). Wong-Baker FACES Pain Rating Scale. Accessed January 7, 2021. https://wongbakerfaces.org/5. Shirley Ryan AbilityLab. McGill Pain Questionnaire. Accessed January 7, 2021. -questionnaire3AMERICAN ACADEMY OF FAMILY PHYSICIANS
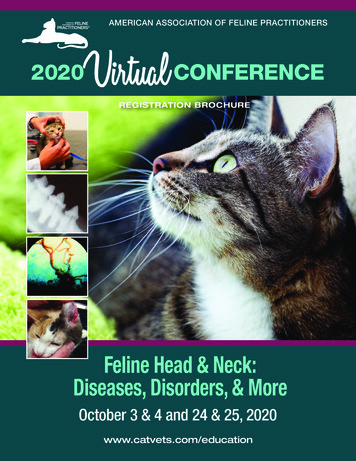
AAFP Chronic Pain ToolkitChronic PainManagementToolkitBrief Pain Inventory ! 23 445 C 6 7BB ! C84BJ6GL;74E C9 6?6QE497549 C94;5DAB @5 9?6 6EB @BCN?9 ? E@ E2B6;;; 9S: B6 5 59;B9Eh9 J4:7B A6794 4BGB4 H4B2)CI *&DB #C ;JEA656@749B;C@ D9B;6E96;94@) F59 ,, 4 7-/ 4)') % ;E94 B5 B R4 5 J67A :DB;E2P2S7 -@ ; E 6 5 5JK69BET6E94 D9BO;gVWXE6O YaZf4 YJG75; 5G:;[E\YZ894 6E E7[\bcB5 B94B9dYU@f 594BVW9XfY 9C G5;f J675DB;EB9;9 2egijklm1hqror 0B9pq 4Eop.GB MOB#'B 45 1n 26 66]R 9CJU2 (BB ':5D8&7 %12e O 1 " sqxstyuqqsrvqzqt{rs wg2S:: BB 95;BE99h 4J 6:7B 1n59DOB;gE4f6J7OG5 ;5G:;E894 6E E7@f 594B9f 9C G5;f J6egijklm1pqqror5DB;EB9;9 hop72sqxstyuqqsrvqzqt{rs s s wi2S:94 B B 5 5Bh9B 8J 67DB;EfJG;5G:;E894 6E E7@f 594B9f 9C G5;f wj2S5:;8 B49 hE 56R1nB9 J675DB;EfJG;5G:;E894 6E E7@f 594B99 :: 46R@7G4DOegijklm1rEJ674B hpq;2opBqosrxsqytqusqrzvqq{trwSB8 16AOUsed by permission of Charles S. Cleeland, PhD., Pain Research GroupCopyright 2021. All rights reserved.HOP 200120034AMERICAN ACADEMY OF FAMILY PHYSICIANS
AAFP Chronic Pain ToolkitBrief Pain Inventory, page 2 ! l2} # 4 95J 9469 :;7C# 4 B ;E59 r ! @9 Og5hE: G O: 59A 452 6C E 5@ ? 4GC; C65;GBRG:9;@ 9674EG B456E5 : ;DJ 6A 745BG5 G E9 DB8;B ; )*;&B ######5 # 894 'EE9 A 6B599@J@667 E59 94D B6;65RE)# , E;e 5E9ts74JB:@hf67 G# ,-#./# 0)'# )%# #-M@ 4C6;GBR9@;67EG 45 :; A2 R1o57h gh ih jh kh lh mh 1h h 6 ( B; '6 &94S % M G 9 C1oBB n;5 6h2BEDm 2 k " 59; 594B9C G5;f 46R?C75;E894 DB 9Og4675 ?Dhoz B r ; E4B ;9JOegijklm1ohoz w s 2 6h6o t s tC1 s Oegijklm1ohoz w s 2 }Bh:L;E8 1 o ts sf;:;9 tJOegijklm1ohoz w s 2 P6h5@B:}1 o ts65LF;OEG:7C ef694Rg65L67i9 ;C 94j 46@ kBEC4l67s R 6m1o 5LtHhoz w s 2 h:B9;6E 1 o tsR;946O94 5D e6D:s t gijklm1ohoz w s 2 :h o ts t tD1 sOegijklm1ohoz w s 2 Eh1 o ts 6J@ EO96A:;As egijklm1oohz w s SB8 O6A «¡¡ ¡ ¡ ¡ § s tª §OUsed by permission of Charles S. Cleeland, PhD., Pain Research GroupCopyright 1991. All rights reserved.HOP 200120035AMERICAN ACADEMY OF FAMILY PHYSICIANS
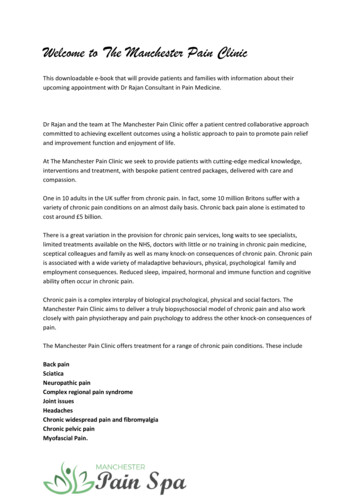
AAFP Chronic Pain ToolkitPEG SCALE ASSESSING PAIN INTENSITY AND INTERFERENCE(Pain, Enjoyment, General Activity)1. What number best describes your pain on average in the past week?0123456No Pain78910Pain as bad as you can imagine2. What number best describes how, during the past week, pain has interfered with your enjoyment of life?01234567Does not interfere8910Completely interferes3. What number best describes how, during the past week, pain has interfered with your general activity?01Does not interfere2345678910Completely interferesComputing the PEG ScoreAdd the responses to the three questions, then divide by three to get a mean score (out of 10) on overallimpact of points.Using the PEG ScoreThe score is best used to track an individual’s changes over time. The initiation of therapy should result in theindividual’s score decreasing over time.SourceKrebs EE, Lorenz KA, Blair MJ, et al. Development and initial validation of the PEG, a three-item scale assessing pain intensity and interference.J Gen Intern Med. 2009;24(6):733-738.6
AAFP Chronic Pain ToolkitFUNCTIONAL AND OTHER ASSESSMENTS Section 2OVERVIEWIn addition to pain itself, a comprehensive assessmentof chronic pain should cover other domains, includingfunction, impact on daily activities, quality of life,mental health, and comorbidities and conditions thatmay require additional assessment and management.1Examples of conditions that might be impacted orcontribute to changes in quality of life include anxiety,depression, trauma, stigma, substance use disorder,and pain-related factors, such as pain catastrophizingor kinesiophobia.1Functional and General Health ToolsCurrently, there are no universal guidelines for pain-relatedfunctional assessment. Many validated, self-reportingtools are available to assess the impact of chronic pain.The use of appropriate assessment tools can assist infunctional and general psychosocial evaluation.The table below includes selected tools for functionalassessment and coexisting conditions included in thistoolkit, along with links and references to additionaltools assessing function and general health.Functional Assessment and General Health rtedEvaluate and monitor physical,Outcomes Measurement mental, and social health inInformation Systemadults and children(PROMIS ) Global HealthSum of response score with highscores reflecting better functioningTen-item global health Jump to tool in toolkit.assessment toolShort Form HealthSurvey (SF-36)Routine monitoring andassessment of care outcomes inadult patientsScoring process described item-short-form/scoring.htmlGeneric, coherent,and easilyadministered qualityof-life measuresJump to tool in toolkit.Work Productivity andActivity ImpairmentQuestionnaireMeasure impairment in work and Response reviewactivitiesSix-item, validatedquestionnaireJump to tool in toolkit.Functional GoalsAssist with setting functionalN/Agoals for paints with chronic painGoal-settingworksheetJump to tool in toolkit.Tables of Functional Assessment Instruments and Coexisting Conditions ToolsTable A. Considerationsfor Common CoexistingConditionsAdditional resources, tools, and considerations for common coexisting conditions to beconsidered in chronic pain assessmentsJump to table in toolkit.Table B. SelectedCondition SpecificFunctional AssessmentOverview and links to a select list of functional assessment instrumentsJump to table in toolkit.References1. Williams DA. The importance of psychological assessment in chronic pain. Curr Opin Urol. 2013;23(6):554-559.7AMERICAN ACADEMY OF FAMILY PHYSICIANS
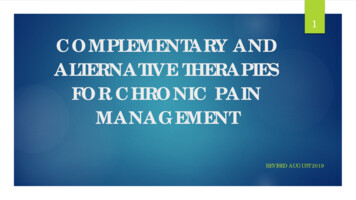
AAFP Chronic Pain Toolkit(PROMIS Scale v1.2–Global Health)GLOBAL HEALTHPlease respond to each question or statement by marking one box per row.ExcellentVery letelyMostlyModeratelyA LittleNot at ldModerate543GLOBAL01 — In general, would you say your health is:GLOBAL02 — In general, would you say your quality of life is:GLOBAL03 — In general, how would you rate your physical health?GLOBAL04 — In general, how would you rate your mental health, includingyour mood and your ability to think?GLOBAL05 — In general, how would you rate your satisfaction with your socialactivities and relationships?GLOBAL09R — In general, please rate how well you carry out your usual socialactivities and roles. (This includes activities at home, at work and in yourcommunity, and responsibilities as a parent, child, spouse, employee, friend, etc.)GLOBAL06 — To what extent are you able to carry out your everyday physicalactivities such as walking, climbing stairs, carrying groceries, or moving a chair?In the past 7 days GLOBAL10R — How often have you been bothered by emotional problemssuch as feeling anxious, depressed or irritable?Severe Very SevereGLOBAL8R — How would you rate your fatigue on average?21GLOBAL7R — How would you rate your pain on average?012345678910No PainWorst painImaginable13 April 2018 2010–2018 PROMIS Health Organization (PHO)8
AAFP Chronic Pain Toolkit9
AAFP Chronic Pain Toolkit10
AAFP Chronic Pain Toolkit11
AAFP Chronic Pain Toolkit12
AAFP Chronic Pain Toolkit13
AAFP Chronic Pain Toolkit14
AAFP Chronic Pain ToolkitWork Productivity and ActivityImpairment QuestionnaireChronic PainManagementToolkitThe following questions ask about the effect of your health problems on your ability to work and perform regularactivities. “Health problems” are defined as any physical or emotional problem or symptom. Please fill in the blanksor check the appropriate box, as indicated.1. Are you currently employed (working for pay)?If NO, check “NO” and skip to question 6.YesNo2. During the past seven days, not including today, how many hours did you miss from work becauseof your health problems?Include hours you missed on sick days, times you went in late, left early, etc., because of yourhealth problems. Do not include time you missed to participate in this study.HOURS3. During the past seven days, not including today, how many hours did you miss from work becauseof any other reason, such as vacation, holidays, time off to participate in this study?HOURS4. During the past seven days, not including today, how many hours did you actually work?(If “0”, skip to question 6.)HOURS5. During the past seven days, not including today, how much did your health problems affect your productivity whileyou were working?Think about days you were limited in the amount or kind of work you could do, days you accomplished less thanyou would like, or days you could not do your work as carefully as usual. If health problems affected your workonly a little, choose a low number. Choose a high number if health problems affected your work a great deal.Consider only how much health problems affected productivity while you were working.Health problems had noeffect on my daily activities01Health problems completely preventedme from doing my daily activities23456789106. During the past seven days, not including today, how much did your health problems affect your ability to do yourregular, daily, non-work activities?“Regular activities” are defined as the usual activities you do, such as work around the house, shopping,childcare, exercising, studying, etc. Think about times you were limited in the amount or kind of activities youcould do and times you accomplished less than you would like. If health problems affected your activities onlya little, choose a low number. Choose a high number if health problems affected your activities a great deal.Consider only how much health problems affected your ability to do your regular, daily, non-work activities.Health problems had noeffect on my daily activities01Health problems completely preventedme from doing my daily activities2345678910Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibilityof a work productivity and activity impairment instrument.PharamcoEconomics 1993; 4(5):353-65HOP 2001200315AMERICAN ACADEMY OF FAMILY PHYSICIANS
AAFP Chronic Pain ToolkitChronic PainManagementToolkitFunctional GoalsWhich, if any, activities are limited due to pain? (Check all that apply)walkingsexual activityrelationships (family, friends)exerciseworkself-care (bathing, dressing, eating)sleephouseworkOther:Which activites are most important to you?Provider: Work with patient to determine realistic goals and on an action plan to achieve these goals.ActivityGoalActionReassess improvement/decline in function at regular intervals.HOP 2001200316AMERICAN ACADEMY OF FAMILY PHYSICIANS
AAFP Chronic Pain ToolkitTable A. Considerations for Common Coexisting ConditionsAssessmentDomainsMental HealthCommonConditionsAnxietySelected Additional ResourcesGeneral AnxietyDisorder-7 (GAD-7)www.aafp.org/afp/2015/0501/p617.htmlPatient 1015/p508.htmlAlcohol, Smokingand SubstanceInvolvementScreening Test(ASSIST)ASSIST: www.who.int/substance abuse/activities/assist test/en/Trauma and/orPTSDPost-traumatic StressDisorder (PTSD)Checklist for duced QoLSee tools included inthis ia/fulltext/2007/03000/a primer on health related quality of lifein.49.aspxFunctionallimitationsSee tools included in this tf-fact-sheetstigma 508-2019-08-13.pdfPain RelatedPsychologicalFactorsPainCatastrophizingPain CatastrophizingScale need-knowDepressionSubstance Use/Substance UsedDisorders efault/files/GAD-7 Anxiety-updated 0.pdfwww.aafp.org/dam/AAFP/documents/patient DA Drug Screening eening qr.pdfSBIRT (screening, brief intervention, and referral to treatment forsubstance use): phobiaChemical coping/self-medication17SelectedAssessment ToolsTampa Scale Factsheet/PainAlcohol.pdfwww.tac.vic.gov.au/ data/assets/pdf file/0004/27454/tampascale kinesiophobia.pdf
AAFP Chronic Pain ToolkitTable B. Selected Condition Specific Functional Assessment ToolsKnee Injury and Osteoarthritis Outcome Score (KOOS)Tool: www.koos.nu/koos-english.pdfScoring: www.koos.nu/KOOSscoring2012.pdf18West Haven Yale Multidimensional Pain Inventory (WHYMPI/MPI)Tool: www.va.gov/PAINMANAGEMENT/WHYMPI MPI.aspQuick Disabilities of Arm, Shoulder and Hand (QuickDASH)Tool: dash.iwh.on.ca/about-quickdashHip Disability and Osteoarthritis Outcome Score (HOOS)Tool: www.koos.nu/
AAFP Chronic Pain ToolkitPAIN MANAGEMENT Section 3OVERVIEWPain management is determined primarily by whether pain is acute or chronic. Management of chronic painshould be individualized, patient-centered, and based on shared decision making and goals of treatment.Considerations for determining acute versus chronic pain can be found in the table on the next page.Pharmacological treatment of pain should use the lowest effective dosage for pain relief and functional improvement.Both pharmacological and non-pharmacologic treatments have shown to be effective in managing pain. Evidence forthe effectiveness of various treatments for chronic pain can be found in the table on the next page.Management of chronic pain is covered by several different guidelines and systematic reviews with varyingrecommendations based on location and type of chronic pain.In response to the opioid public health crisis, new guidance recommends non-pharmacologic and non-opioidsas first-line therapies, when clinically appropriate.1 If an opioid is considered for treatment, the lowest effectivedosage for pain relief and functional improvement should be used.Guidelines and Evidence ReviewsThe following are recent evidence reviews and evidence-based guidelines for primary care physicians and otherclinicians in addressing acute and chronic pain: The American College of Physicians (ACP) and the AFFP jointly developed the clinical practice guideline,Management of Acute Musculoskeletal Pain, which includes evidence-based recommendations forpharmacologic and non-pharmacologic management of acute pain resulting from musculoskeletal injuries.2 The ACP developed, and the AAFP endorsed, the clinical practice guideline, Low Back Pain, which includesevidence-based recommendations for management of acute and chronic low back pain with an emphasis onnon-pharmacologic and non-opioid therapies as first-line treatment.3 The U.S. Department of Health and Human Services’ Pain Management Best Practices Inter-Agency TaskForce developed the report, Pain Management Best Practices, which is a comprehensive document outliningdifferent approaches for the treatment of pain.4Two evidence reviews developed by the Agency for Healthcare Research and Quality (AHRQ) summarize andprovide assessment of the quality of current evidence on pharmacologic and non-pharmacologic treatment ofchronic pain: Nonopioid Pharmacologic Treatments for Chronic Pain5 Noninvasive Treatments for Low Back Pain619AMERICAN ACADEMY OF FAMILY PHYSICIANS
AAFP Chronic Pain ToolkitChronic Pain Management ToolsThe table below includes selected tools for chronic pain management in this toolkit, along with links and referenceto additional tools.Chronic Pain Management Tools in ToolkitNameDescriptionLocationTable C. ManagementConsiderations Based on PainType: Acute Versus Chronic PainOverview of background and managementconsiderations for acute versus chronic painJump to table in toolkit.Table D. Chronic PainTreatments OverviewOverview of pharmacologic and non-pharmacologictreatment options for chronic pain with evidencebased indicationsJump to table in toolkit.Chronic Pain Patient HandoutTwo-page patient handout lists chronic paintreatment options and provides information ontreatment goalsJump to tool in toolkit.Additional Chronic Pain Management ToolsPain Self-Management StrategiesSelf-management resource guide for patients withchronic QRI ntary HealthApproaches for Chronic Pain:What the Science SaysCurrent evidence on complementary health products ntary-healthand practices for managing chronic . Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain — United States, 2016. MMWR Recomm Rep. 2016;65(1):1-49.2. American Academy of Family Physicians. Management of acute musculoskeletal pain. Clinical Practice Guideline. Accessed January 8, s/musculoskeletal-pain.html3. American Academy of Family Physicians. Low back pain. Clinical Practice Guideline. Accessed January 8, s/back-pain.html4. Pain Management Best Practices Inter-Agency Task Force. Pain management best practices. U.S. Department of Health and Human Services. AccessedJanuary 8, 2021. ctices-draft-final-report-05062019.pdf5. Agency for Healthcare Research and Quality. Nonopioid pharmacologic treatments for chronic pain. Accessed January 8, fault/files/pdf/nonopioid-chronic-pain.pdf6. Agency for Healthcare Research and Quality. Noninvasive treatments for low back pain. Accessed January 8, fault/files/pdf/back-pain-treatment research.pdf20AMERICAN ACADEMY OF FAMILY PHYSICIANS
AAFP Chronic Pain ToolkitTable C. Management Considerations Based on Pain Type: Acute vs. Chronic Pain21CharacteristicsAcute PainChronic PainDurationNormal healing duration; 3-6 monthsProlonged duration 6 monthsFunctionPhysiologic (protective)Pathologic (non-protective)CauseAcute illness, injury, trauma, surgery or other medicalprocedureInjury, chronic illness, cancer, may have noindefinable pathologyCharacteristicsUsually nociceptive; sharp, localized, sudden/gradualonsetUsually a combination of nociceptive andneuropathic, dull, aching, generalized,persistentTreatment options(non-inclusive list no inany particular order)Nonsteroidal anti-inflammatory drugs (NSAIDS),acetaminophen, opioids, nerve bocks, ketamine, musclerelaxants, pain-reducing modalities (e.g., immobilization,heat/cold, and elevation), graded exercise of the affectedbody area, physical therapy. Opioids are not recommended for acute low back pain.Non-opioid analgesics, physical therapy,cognitive behavioral therapy, rehabilitation,exercise, integrative medical therapies(e.g., yoga, relaxation, tai chi, massage, andacupuncture), opioids on a case-by-case basisGoals of treatmentPain Resolution Resolve underlying cause:- Facilitate recovery- Reduce pain- Minimize side effects- Prevent chronic painPain Control Restore function:- Restore function (physical, emotional, social)- Decrease pain (e.g., treat underlying cause,minimize medication use)- Correct secondary consequences(e.g., maladaptive behavior)
AAFP Chronic Pain ToolkitTreatment Options for Chronic PainThis table outlines different classes of medications and non-pharmacological treatments with indications for use inchronic pain. While pain management is a major issue in the United States, the evidence is still limited, especial
Pain, Enjoyment ; of Life and . General Activity (PEG) Scale Assess pain ; interference with . enjoyment of life and general activity Mild pain 0-11 or 0 to 4 Moderate pain 12-20 or 4 .