Transcription
Assessing drug synergy incombination therapiesAdam Palmer, Ph.D.Laboratory of Systems PharmacologyHarvard Medical School
OutlineIntroductionPharmacokinetic and pharmacodynamic drug interactionsDrug interactions depend on the phenotypeExperimental designFixed dosesDose gradientsAnalysis of drug interactionsDifferent null hypotheses:Pharmacological independencePharmacological additivityStatistical independenceCheckerboards Gaddum (1940) Loewe (1928) Chou-Talalay (1984) Bliss (1939)Experimental design revisitedClinical relevanceDemonstration of Isobologram analysis
Introduction - Why combination therapy?Clinical Benefit Stronger pharmacologic effect Hinders evolution of drug resistancein viruses, bacteria, and cancers Clinical trials show superior outcomes for the right combinationssome drug combinations are both more effective and less toxicsome drug combinations are both less effective and more toxicResearch Use Combined perturbations reveal functional interactions betweencellular processes Drug interactions depend on mechanism of drug action
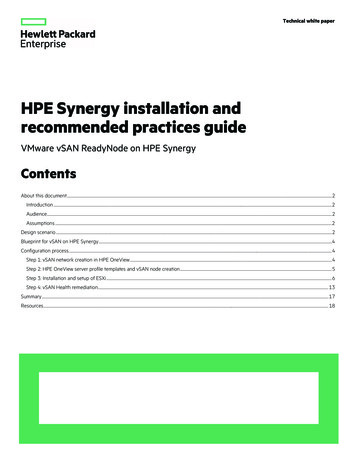
What do we mean by “drug interactions”?Pharmacokinetics What the body does to the drugAbsorption, Distribution, Metabolism, Excretion (ADME)Drug AConcentrationof drug Ain serumTimeDrug Aadministered
What do we mean by “drug interactions”?Pharmacokinetics What the body does to the drugAbsorption, Distribution, Metabolism, Excretion (ADME)In medicine and physiology, “drug interaction” means pharmacokinetic interaction.The kinetics of drug A are changed in the presence of another drug B.Drug BDrug AConcentrationof drug Ain serumTimeDrug A and Drug Badministered
What do we mean by “drug interactions”?Pharmacodynamics What the drug does to the body (or cell) DrugResponseTargetTo molecular biologists, “drug interaction”usually refers to pharmacodynamic interaction. Drugs in combination have unexpectedpotency, e.g. by dose response function.When both drugs exert the same effect,Interpreting drug interactions is complicated.Responseto drugtreatmentDose administered
Caution: drug interactions can vary by endpointDrug treatments usually affect more than one phenotype.A combination therapy could have:Stronger effect on phenotype #1Weaker effect on phenotype #2 Drug interactions must be understood in context of the phenotype.Examples:In skin cancers with BRAF mutation,Combination of BRAF MEK inhibition has- More tumor inhibition- Less skin toxicityTo a toxicologist, “drug synergy” is bad because it refers to harmful effects(alcohol barbiturates)
[Drug B]Experimental Design[Drug A]
Experimental DesignDose gradientsEfficient[Drug A]CheckerboardComprehensive[Drug B][Drug B][Drug B]Single dosesLeast effort[Drug A][Drug A]
Experimental Design[Drug B]CheckerboardComprehensivePractical for pairs only.Most insightful data:Reveals drug interactionsat all ratios between drugs[Drug A]
Experimental Design[Drug B]Dose gradientsEfficientDepends onchoice ofdrug ratio(angle)[Drug A]More effort than single-dose bya fixed factor (eg. 8 more points)Easily scales to triple-, quadrupledrug combinationsNeed to chose a ratio betweendrugs (angle)Analysis can be attentive todose-response function Robust assessment ofinteractions at the chosen ratioFixed ratio combination[A] : [B] 1 : 5Mixed in equal potency “Equipotent” (on a chosen readout)
Experimental Design[Drug B]Dose gradientsEfficientMight missinteractions ifpotencies areimbalanced.Depends onchoice ofdrug ratio(angle)[Drug A]More effort than single-dose bya fixed factor (eg. 8 more points)Easily scales to triple-, quadrupledrug combinationsNeed to chose a ratio betweendrugs (angle)Analysis can be attentive todose-response function Robust assessment ofinteractions at the chosen ratioFixed ratio combination[A] : [B] 1 : 1Mixed in equal concentration “Equimolar”
Experimental Design[Drug B]Single dosesLeast effortEasily scales to triple- ,quadruple-drug combinationsDepends onchoice ofeach drug’seffect[Drug A]High-throughput screeningData has limited value:no analysis of dose-response prone to false-positiveinteractions
Experimental DesignCannot reliably detect a change in drug potency less than the increments in drug concentration.Solution: Small-step serial dilutionsTransfer700 µL1200 µL1000 nMdrug in mediaTransfer700 µL400 µLmediaTransfer700 µL400 µLmediaTransfer700 µL400 µLmediaTransfer700 µL400 µLmedia400 µLmedia
Experimental DesignCannot reliably detect a change in drug potency less than the increments in drug concentration.Solution: Small-step serial dilutions1000 nMdrug in media636 nMdrug405 nMdrug 258 nMdrug164 nMdrug104 nMdrug
Analysis of drug interactionsIdentifying drug interactions depend on the “no interaction” null-hypothesis.Null-hypotheses are based on the observed drug responsenot a model of mechanism.If “Synergy” means “stronger than my mechanistic model predicts”, then:(1) a genuinely powerful combination isn’t classed as synergistic if it is predictable(2) synergy/antagonism changes as your knowledge and model changes.Descriptions based on the dose-response are empirical,and do not depend on current state of understanding.Explained well by Berenbaum (1989) What is Synergy? Pharmacological Reviews
Analysis of drug interactionsIdentifying drug interactions depend on the “no interaction” null-hypothesis.Null-hypotheses are based on the observed drug responsenot a model of mechanismGaddum (1940): Pharmacological IndependenceAre two drugs more or less powerful than one drug?Loewe (1928): Pharmacological Additivity:Are drugs (A B) more or less powerful than (A more A), or (B more B)?Also measured by the Chou-Talalay ‘Combination Index’Bliss (1939): Statistical Independence of toxins:In a population, is each individual’s probability of death from drug Astatistically independent of the probability of death from drug B?These are different questions.Not alternative ways to ask the same question.
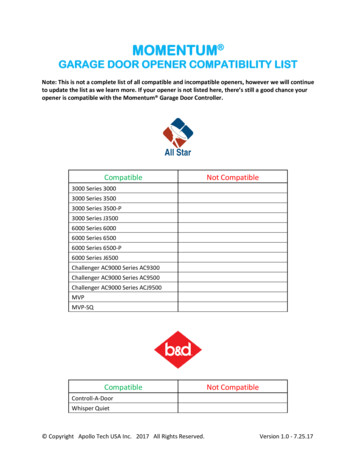
Gaddum (1940) Pharmacological independenceDose α of drug A has a certain strength of effect.[Drug A]How much drug A is needed to have the same effect when drug B is added?[Drug B]
Gaddum (1940) Pharmacological independenceDose α of drug A has a certain strength of effect.How much drug A is needed to have the same effect when drug B is added? 1μM drug BNo change No interaction[Drug A]α[Drug B]
Gaddum (1940) Pharmacological independenceDose α of drug A has a certain strength of effect.How much drug A is needed to have the same effect when drug B is added? 1μM drug B[Drug A]αNo change No interactionLess drug A is needed Synergy[Drug B]
Gaddum (1940) Pharmacological independenceDose α of drug A has a certain strength of effect.How much drug A is needed to have the same effect when drug B is added?More drug A is needed Antagonism 1μM drug B[Drug A]αNo change No interactionLess drug A is needed Synergy[Drug B]
Gaddum (1940) Pharmacological independenceSimple analysis when only one drug produces the effect studied.What if both drugs have this effect?Independence[Drug A]α[Drug B]β
[Drug B]Isobologram analysis[Drug A]
Isobologram analysis[Drug B]Points with a particular strength of drug effect(e.g. 50% inhibition – can use any threshold)[Drug A]
[Drug B]Isobologram analysisIsobole contour line of equal drug effect[Drug A]
Isobologram analysisLike contour maps in geography:0%20%40%60%80%
Example of isobologram analysisInterpretation after a break / questions
Gaddum (1940) Pharmacological independenceαIndependence[Drug A]AntagonismSynergy[Drug B]β
Loewe (1928) Pharmacological additivityThe only certain expectation is that a drug ‘combined’ with itselfproduces straight-line isoboles[Drug A]α[Drug A]α
Loewe (1928) Pharmacological additivityThe only certain expectation is that a drug ‘combined’ with itselfproduces straight-line isoboles[Drug A]α[Drug A]αLinear drug scale
Loewe (1928) Pharmacological additivityThe only certain expectation is that a drug ‘combined’ with itselfproduces straight-line isobolesα6 0 65 1 6[Drug A]4 2 63 3 62 4 61 5 60 6 6[Drug A]αLinear drug scale
Loewe (1928) Pharmacological additivityLinear drug scale
Loewe (1928) Pharmacological additivityCan measure over logarithmic concentration gradient,and analyze over linear concentration gradients
Loewe (1928) Pharmacological additivityFor two different drugs, additivity is not a prediction but a point of referencefor the readout, regardless of mechanism.Additivity achieving a stronger effectneeds the same increasein drug A or drug B
Loewe (1928) Pharmacological additivityAdditivity is predicted when two drugs bind the same pocket with the same effect.For two different drugs, additivity is not a prediction but a point of reference.Synergy achieving a stronger effectis easier with a second drug.
Loewe (1928) Pharmacological additivityAdditivity is predicted when two drugs bind the same pocket with the same effect.For two different drugs, additivity is not a prediction but a point of reference.Antagonism achieving a stronger effectis harder with a second drug.
Loewe (1928) Pharmacological additivityDefinitions of “independence”, “synergy”, “antagonism” are argued,but Loewe’s additivity is undisputed.Gaddum called additivity a special case of synergy:Fig. 65, Gaddum (1942) Pharmacology
Chou-Talalay (1984): the Combination Index[Drug B]Loewe’s additivity model simplified for fixed-ratio combinations[Drug A]
Chou-Talalay (1984): the Combination IndexLoewe’s additivity model simplified for fixed-ratio combinations[Drug B]IC50 BIC50 A B[Drug A]IC50 A
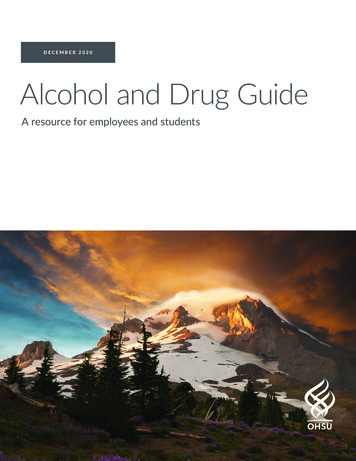
Chou-Talalay (1984): the Combination IndexLoewe’s additivity model simplified for fixed-ratio combinations(0, IC50 B)[Drug B](a, b)Combination Index [Drug A](IC50 A, 0)ab IC50 AIC50 B
Chou-Talalay (1984): the Combination IndexLoewe’s additivity model simplified for fixed-ratio combinations(0, IC50 B)[Drug B]C.I. 1 AntagonismC.I. 1 AdditiveCombination Index C.I. 1 Synergy[Drug A](IC50 A, 0)ab IC50 AIC50 B
Chou-Talalay (1984): the Combination IndexLoewe’s additivity model simplified for fixed-ratio combinations(0, IC50 B)[Drug B]Analysis valid at any ratioCombination Index [Drug A](IC50 A, 0)ab IC50 AIC50 B
Chou-Talalay (1984): the Combination IndexLoewe’s additivity model simplified for fixed-ratio combinations(0, IC50 B)Analysis valid at any ratio[Drug B]or with a fixed dose of drug BCombination Index (a, b)[Drug A](IC50 A, 0)ab IC50 AIC50 B
Bliss (1939): Statistical Independence of toxinsPopulation of toxin-treated individuals(e.g. cells, or people; originally insect eggs)
Bliss (1939): Statistical Independence of toxinsPopulation of toxin-treated individuals(e.g. cells, or people; originally insect eggs)PB of killingby Drug BPA of killingby Drug AIf probabilities of death are statistically independent,then PA B 1 – (1 – PA) (1 – PB)Bliss method can apply to other probabilities of “yes/no”events in populations, e.g. enzymes active or inhibited.Not scientifically valid to analyze quantitative phenotypes,e.g. blood pressure, length of cell cycle.
Bliss (1939): Statistical Independence of toxinsBliss is not appropriate for growth inhibition:Uninhibitedgrowth
Bliss (1939): Statistical Independence of toxinsBliss is not appropriate for growth inhibition:UninhibitedgrowthCytostatic
Bliss (1939): Statistical Independence of toxinsBliss is not appropriate for growth inhibition:UninhibitedgrowthCytostaticBy Bliss Independence,two cytostatic drugswould be expected tohave a strongly cytotoxiceffect in combination.
Bliss (1939): Statistical Independence of toxinsStatistical interaction assessed by Bliss givesno information about pharmacological interaction.[Drug B]?[Drug A]Bliss synergy can occur with Loewe antagonism.Bliss antagonism can occur with Loewe synergy.These methods ask different questions,and Bliss method lacks attention to dose response shape.Survival:80% 15%100% –Bliss method identifies drugs as ‘synergistic’ with themselves,when doses are at the tipping point of a steep dose-response.Survival0% –012DoseThese points explained well by Berenbaum (1989) What is Synergy? Pharmacological Reviews
Analysis of drug interactionsSynergy: “work together”Antagonism: “struggle against”Modern“Antagonism”can produceclassic “synergy”Modern “synergy”is not necessaryfor stronger effectand clinical benefitClassical interpretation: (Gaddum)Synergy:Two drugs Strongest one drugNo interaction:Two drugs Strongest one drugAntagonism:Two drugs Strongest one drugModern interpretation: (Loewe,Synergy:Two drugs No interaction:Two drugs Antagonism:Two drugs or Combination Index, or Bliss)“sum of parts”“sum of parts”“sum of parts”Definitions of ‘no interaction’ are different.Modern use of ‘synergy’ or ‘antagonism’depends on the expected sum of parts.
Experimental Design Revisited[Drug A]CheckerboardComprehensive[Drug B]Depends onchoice ofeach drug’sdose / effectDose gradientsEfficient[Drug B][Drug B]Single dosesLeast effortDepends onchoice ofdrug ratio[Drug A]Pharmacological Additivity (Loewe):[Drug A]Isobologram analysisCombination Index (Chou-Talalay)Pharmacological Independence (Gaddum)Statistical Independence (Bliss)
Experimental Design RevisitedDose gradientsEfficient[Drug A][Drug B][Drug B][Drug A][Drug A]Can calculate“excess over additive”CheckerboardComprehensive[Drug B][Drug B][Drug B]Single dosesLeast effort[Drug A][Drug A]
Clinical RelevanceIs drug synergy necessary for clinical benefit?Complicating factors: Synergy of desired effect vs. Synergy of toxic side effects Synergy vs. Individual drug potency Synergy vs. Slowing evolution of drug resistance Synergy vs. Addressing heterogeneity
Three rationales for combination cancer therapyPharmacologicaladditivity or synergyS. Loewe (1928) Ergeb. Physiol.Gaddum (1940) PharmacologyWithin-tumorheterogeneityL. Law (1952) Cancer ResearchBetween-tumorheterogeneityE. Frei 3rd, et al. (1961)Blood
Figure adapted fromEmil Frei 3rd, et al.Blood (1961) 18:431
Independent actionexplains the clinicalefficacy of many2-drug combinationtherapies for acuteleukemiaFigure adapted fromEmil Frei 3rd, et al.Blood (1961) 18:431
Independent action explains the clinical efficacyof many combination therapies for metastatic cancersPalmer & Sorger (in review)
Conducting Isobologram analysisResponse grid
Conducting Isobologram analysisResponse grid 3D coordinates
Conducting Isobologram analysisResponse grid 3D coordinates
Conducting Isobologram analysisResponse grid 3D coordinates Interpolation(recommend first-order interpolation)
Conducting Isobologram analysisResponse grid 3D coordinates Interpolation Contour plot
Calculating Combination Index[Drug B]IC50 B(a, b)abCombination Index IC50 AIC50 B[Drug A]IC50 A
Stronger effect on phenotype #1 Weaker effect on phenotype #2 Drug interactions must be understood in context of the phenotype. Examples: In skin cancers with BRAF mutation, Combination of BRAF MEK inhibition has - More tumor inhibition - Less skin toxicity To a toxicologist, "drug synergy" is bad because it refers to harmful effects