Transcription
Toward Trauma-Informed Home Visiting:Addressing Depression and SocialSupportRobert T. Ammerman, PhD1,2Alonzo T. Folger, PhD1,21 Cincinnati Children’s Hospital Medical Center, University of Cincinnati College of Medicine,Department of Pediatrics2 Every Child Succeeds, Cincinnati, Ohio
Interpersonal Traumatic Experiences Physical Abuse Sexual Abuse Emotional Abuse Witnessing Violence Physical and Sexual Assault Intimate Partner ViolenceSource: Stress, Trauma, and Resilience Lab.San Francisco State University
Source: Centers forDisease Control andPrevention
Epidemiology of Childhood (0-18) TraumaticExperiences Adverse Childhood Experiences (ACEs): Abuse, Neglect andexpanded to Household Dysfunction Prevalence of ACEs: 15.2% with 4 or more ACEs High ACEs 0-5 years 2.7-3.5† fold higher risk for poorKindergarten outcomes High ACEs 0-18 years 4-12‡ fold higher risk for alcoholism,drug abuse, depression, and suicide attempts†Jimenez‡ Felitti,(2016), Fragile Families and Child Wellbeing Study, MCHJ(1998), ACEs Study, Am J Prev Med
Cumulative ACEs and Mental Health
Protective Factors as ACE Buffers? Interpersonal Supports Emotional Health Meaningful Engagement(e.g. my life as meaning) Physical HealthBehaviorsSource: Gouin, Caldwell, Woods, Malarkey (2017) Ann. Behav. Med
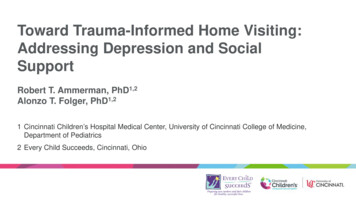
Every Child Succeeds Home Visiting Regional home visiting program: Southwest Ohio &Northern Kentucky families Network of 9 community-based agencies that enroll1,500 mothers annually Eligibility Criteria: first-time mothers who are 18years, unmarried, living in poverty, and/or who have lateentry into prenatal care Goals: positive parenting; healthy home environment;optimal development
Interpersonal trauma experiences ofmothers in ECS home visitingN 806Trauma 74.1%2 68.9%
MaternalAdverseChildhoodExperiences(ACEs)28.8% with 4 ormore ACEs
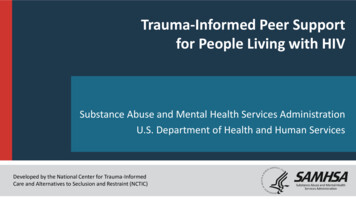
ACE Total Score in ECS Sample and CDC 2009 Five StateSurvey, Female Sample (18-24 1%21.0%17.1%13.2%15%10.5%7.6%10%5%0%012HV sample3CDC 4
Profiles of Maternal ACE Exposure (ECS)Emotional AbusePhysical AbuseSexual AbuseEmotional NeglectPhysical NeglectHousehold IPVHousehold (Drugs)Household (Men. ill)Household (Prison)Household (Div.)Mother #1: Reported experiencingmany ACEsMother #563: No ACEs
Maternal interpersonal trauma and negativeoffspring social-emotional development
Maternal Trauma History to Offspring DevelopmentAdapted from Folger et al (2017)
Maternal Trauma Linked to Infant Epigenomeand Increased Vulnerability?Early exposure tomaternal distressInfant social-emotionalfunction
Trauma, Depression, and SocialSupportRelationships in Home Visiting
Impact in Home VisitingN 220 first time mothersEligible and enrolled in either:- Nurse-Family Partnership- Healthy Families AmericaProvided data throughout the first 18 months of home visiting
Dimensions assessed:-Demographic factorsChildhood Trauma Questionnaire (CTQ)Beck Depression Inventory-II (BDI-II)Interpersonal Support Evaluation List (ISEL)Parenting Stress Inventory-Short Form (PSI)Measurement occasions:- Enrollment, 9-months post enrollment, 18-months post enrollment
Model to be testedEnrollment9 dMaltreatmentDepressiveSymptomsCovariates18 MonthDepressiveSymptoms
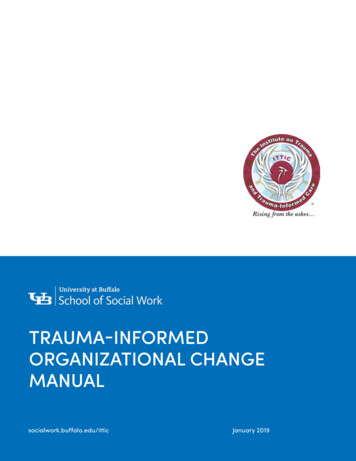
9 MonthEnrollment-.31***SocialSupport.78***18 siveSymptomsAfter controlling demographics andPSI severity at 9 monthsShenk, Ammerman, et al., (2017), Prevention Science.26*Model Fit:TLI:RMSEA:SRMR:.97.04.03
-.31***Enrollment9 MonthSocialSupportSocialSupport18 enk, Ammerman, et al., (2017), Prevention 26*
Conclusions Trauma predicts increased parenting stress at 18 monthsof home visiting Both social support and depression are the ways in whichtrauma predicts parenting stress Timing is important Home visiting may not be as effective for mothers with ahistory of maltreatment in childhood More efficient targeting may improve home visiting effects
Course of Depression (BDI 13 @enrollment and/or 9 months) in homevisitation (N 806)74.8%withtraumahistoryNon-DepDep55.8%44.2%12% receivemental healthtreatmentHome visitingalone has noimpact onAmmermanet al., 2009depression
Depression and parenting and parenting stress
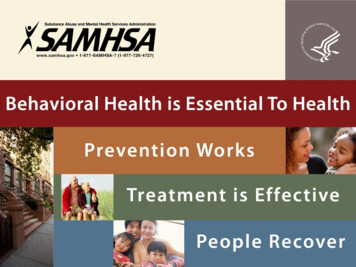
BDI-II Scores at Pre-Treatment, Post-Treatment, &Follow-Up35BDI-II Score3025201510IHCBTTHV5PrePostAssessment Time PointF 7.9, p .01FU
Social Support Using ISEL Scale (Total)IH-CBTTHV9085807570656055504540PreF 5.1, p .01PostFU
Treatment of depression & past history of sexual abuse
Predictors of symptom status at post-treatment14IH-CBTsessions12Home visits1086420SymptomaticBDI-II at post-txt: 9Asymptomatic 8Ammerman, R.T., Peugh, J.L., Putnam, F.W., & Van Ginkel, J.B. (2012). Predictors of treatmentresponse in depressed mothers receiving In-Home Cognitive Behavioral Therapy and concurrenthome visiting. Behavior Modification, 36, 462-481.
What is trauma-informed home visiting?Current conceptualization: Understanding of trauma and its effects Increased awareness and recognition ALSO:–––––Identification of depressionPrevention and treatment of depressionIncreasing natural social supportsBuilding positive social networksTiming of interventions
What can we do in home visiting to make itmore trauma informed? Mood management– Pleasant events– Cognitive reframing– Overcoming avoidance Social network and support–––––Social network analysisReconnecting with lost social resourcesAccessing underutilized resourcesSocial skillsReducing social anxiety and building confidence
Depression-preventionInformation about depressionScreeningSupporting mothersMaking referralsExamples: Pleasant activitiesResourcesAvailable for free downloadat the SAMHSA store:http://store.samhsa.gov/
Next steps Developing new interventions for use in home visitingGreater emphasis on depression and social supportGreater appreciation for timing of strategiesIncorporating intervention into home visitingModifying curriculum and training
Questions and Comments?
Epidemiology of Childhood (0-18) Traumatic Experiences Adverse Childhood Experiences (ACEs): Abuse, Neglect and expanded to Household Dysfunction Prevalence of ACEs: 15.2% with 4 or more ACEs High ACEs 0-5 years 2.7-3.5 † fold higher risk for poor Kindergarten outcomes High ACEs 0-18 years 4-12 ‡